Article Text

Abstract
Tuberculosis cases in children (aged under 15 years) in the National Surveys rose from 308 (rate: 3.3 per 100 000) in 1988 to 408 (4.2 per 100 000) in 1993 and then fell to 364 (3.6 per 100 000) in 1998. The rates in white children were 1.6, 2.0, and 1.1 per 100 000 respectively; in Indian subcontinent children, the rates were unchanged between 1988 and 1993 at around 33 per 100 000 but fell to 23 per 100 000 in 1998. In black African children, the rates were 15, 34, and 71 per 100 000 respectively. From 1988 to 1998, the proportion of cases resident in London more than doubled to 49% (rate: 11.9 per 100 000) and the proportion of cases in children born abroad increased from 13% to 27% in the country as a whole.
Although the overall rate of tuberculosis in children in England and Wales has changed little between 1988 and 1998, the distribution of disease has changed in line with the change in adults. Services for the diagnosis and treatment of tuberculosis in children should be adapted to the changing pattern of disease in this group. Continuous enhanced tuberculosis surveillance will enable more detailed and timely scrutiny of trends in tuberculosis in the future.
- tuberculosis
- epidemiology
Statistics from Altmetric.com
A decline in the incidence of tuberculosis in all age groups was reported in the National Surveys of tuberculosis notifications in England and Wales in the decade from 1978/79 to 1988.1–3 In children (aged less than 15 years) there was a 60% decrease in the number of newly notified cases from 747 in 1978/79 to 294 in 1988. In the National Surveys of 1978/79, 1983, and 1988, data on ethnic and geographical patterns of tuberculosis in children reflected those in adults.1–3 Since the 1988 survey (the last published results on children), data from the subsequent National Surveys in 1993 and 1998 have shown a rise in rates of disease in adults, especially in new arrivals, in urban residents, and in those of black African and “other” ethnic groups.4,5
There are several reasons why it is important to see if these patterns are reflected in tuberculosis in children. Children have newly acquired infections, which have usually been transmitted from an adult.6 The incidence in children is thus a marker of the recent transmission in the population, and levels of drug resistance in children are an indication of patterns of resistance currently being transmitted.
In addition, disease patterns are different in children compared to adults. In children aged less than 2 years, one third of those infected with tuberculosis will develop disease, compared to a 10–15% lifetime incidence for those aged above 5 years.6 They are also more susceptible to severe forms of the disease such as miliary and meningeal tuberculosis, but less likely to have infectious pulmonary disease.6 Thus the descriptive epidemiology of tuberculosis in children not only provides clinicians with an appreciation of the current patterns of disease, but also provides insight into current transmission of infection in the population.
Throughout the past decade there have been changes in recommendations for the treatment and control of tuberculosis.7–10 Current Department of Health policy is for the vaccination of neonates in high risk groups and all tuberculin negative school children aged 10–14 years.10 New arrivals from high incidence areas (⩾40 per 100 000) are recommended for screening and the offer of vaccination if tuberculin negative.10 However, practice varies between districts. In addition, a recent shortage of the BCG vaccine has resulted in a temporary disruption of vaccination programmes in schoolchildren, for which a catch up programme is now underway.11,12 Thus it is important to describe trends of tuberculosis in children in order to provide policy makers with data to inform reviews of national and local control and prevention policies.
We report on the patterns of tuberculosis in children in the 1993 and 1998 National Tuberculosis Surveys and compare them to the results of the 1988 survey.1
METHODS
The study methodologies for the 1988, 1993, and 1998 National Tuberculosis Surveys have been described previously.1,4,5
In brief, in the 1988 survey, medical officers for environmental health sent copies of all notification forms for tuberculosis received in that year to the Medical Research Council Tuberculosis Chest Diseases Unit for cases in children (age less than 15 years) from 2 January to 30 December 1988. These were crosschecked against reports received by the Office of National Statistics.
In the 1993 survey, Consultants in Communicable Disease Control sent copies of all notification forms received throughout the year to the Public Health Laboratory Service Communicable Disease Surveillance Centre. Demographic information was collected on all cases in children in the 12 months but clinical, microbiological, and histological information was only collected from 2 January to 2 July 1993.
In the 1998 survey, local coordinators nominated by each health authority were responsible for collecting the survey forms and forwarding them onwards to the survey team.5 The survey form included a copy of a notification slip, which could be used in lieu of the statutory notification form. Demographic and clinical information was collected on all cases diagnosed throughout the calendar year.
For all three surveys, additional microbiological information on species and susceptibility to antituberculosis drugs were obtained from the regional tuberculosis centres in England and Wales.13
The analyses in this report include both cases with and cases without a history of previous treatment for tuberculosis. Published reports on childhood tuberculosis from previous surveys excluded children who had had previous treatment.1–3 Original data from the 1988 survey has been reanalysed to make it comparable to the 1993 and 1998 analyses and is likely to differ from the results previously published on the 1988 survey.1
For our analysis, site of disease was classified into pulmonary disease, other respiratory disease, and non-respiratory disease. Pulmonary disease was defined as disease of the lung parenchyma and/or bronchial tree. “Other respiratory” disease excluded any disease with pulmonary involvement, but included disease of the pleura and intrathoracic lymph nodes.8
In 1993, no details on site of disease were available on 110 (27%) survey cases, partly because this was not requested in the second half of the survey year. In 1988 and 1998, there were more cases reported with multiple sites of disease compared to 1993, which may be related to changes in the survey format. Hence, comparisons relating to site of disease between surveys are difficult, and detailed results are therefore only described for the 1998 survey.
Estimates of population denominator data were obtained from the Labour Force Surveys for 1988, 1993, and 1998. Results were analysed using Epi Info 6 and SPSS 10.0 (SPSS Inc., Chicago, Illinois).
RESULTS
Cases, age, and sex (table 1)
Number of cases in each survey and exclusions
The total number of cases reported to each survey was 449, 522, and 527 in 1988, 1993, and 1998 respectively. Between 22% and 32% of cases were excluded from each survey, the most common reasons being treatment for latent tuberculosis infection (chemoprophylaxis) in the absence of disease or change to a non-tuberculosis diagnosis. After exclusion, there were 308, 408, and 364 eligible cases respectively.
The overall proportions of males and females were approximately equal in each of the surveys. Equal proportions were also seen within ethnic subgroups of the childhood cases with the exceptions of those in the Indian subcontinent (ISC) group in 1998, of which only 39% were female (data not tabulated). There was no difference in age distribution with gender. White children were generally younger than children of ISC or black African ethnicity in all three surveys.
Ethnicity (table 2)
Cases and annual rates in children (0–14 years) per 100000 for England and Wales by ethnic group
The proportion of cases in white children remained unchanged at 44% between 1988 and 1993, but fell to 26% in 1998. The proportion of cases in ISC children was 45%, 41%, and 33% respectively. In contrast, the proportion of cases in children of black African ethnicity rose from 2% in 1988 to 6% in 1993 and 22% in 1998.
Annual rates of disease 1988–98 (table 2)
The rate of disease in children in England and Wales was 3.3 per 100 000 (95% CI 2.9 to 3.7) in 1988, 4.2 per 100 000 (95% CI 3.8 to 4.6) in 1993, and 3.6 per 100 000 (95% CI 3.2 to 3.9) in 1998.
The rate per 100 000 in white children was 1.6 in 1988, 2.0 in 1993, and 1.1 in 1998. The rate in ISC children changed little between 1988 and 1993 at around 33, but fell to 23 in 1998. The ratio of the rate in ISC children compared to white children has remained similar in magnitude in the past decade (21 in 1988, 16 in 1993, and 21 in 1998).
Rates in children of black African ethnicity more than doubled from 1988 to 1993 and did so again between 1993 and 1998.
Place of birth and year of entry to the UK (table 3)
Number of cases of tuberculosis by ethnic group, place of birth, and survey year, and rates for 1998
The proportion of children known to be born abroad was 13% in 1988 and 10% in 1993, but increased to 27% in 1998. In 1988, of the 39 children born abroad for whom the year of entry was known, 18 (46%) had arrived within the previous five years and 14 (36%) within the previous two years. Four (3%) white children, 33 (24%) ISC children, and two children of black African ethnicity were born abroad.
In 1993, of the 32 children born abroad for whom the year of entry to the UK was known, 28 (88%) had arrived within the past five years and 16 (50%) within the past two years. Only two (1%) white children compared with 21(13%) ISC children and 15 (58%) children of black African ethnicity were born abroad.
In the 1998 survey, of the 72 children born abroad for whom the year of entry to the UK was known, 55 (76%) had arrived within the past five years, and 34 (47%) within the past two years. Of the children born outside the UK whose country of birth was known, 30% were born in Somalia.
In 1998, three (3%) white children, 22 (18%) ISC children, and 49 (61%) black African children were born abroad.
Rates of disease are consistently higher for children born abroad compared with those born in the United Kingdom. For children born in the United Kingdom, the rates in ISC and black African children are 19-fold and 25-fold higher than those for white children.
Age specific rates and place of birth for ISC born in the UK and white children (fig 1)
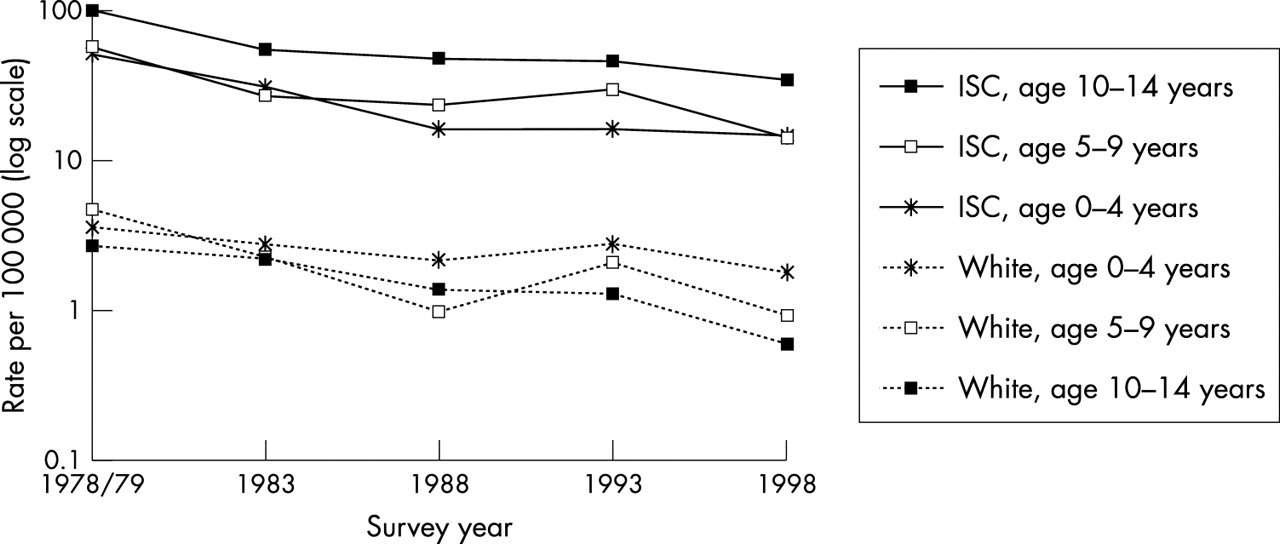
Age specific rates for tuberculosis in children of white and ISC ethnicity (UK born) resident in England.
In order to look at trends in cohorts of children, the age specific rates for children of ISC ethnicity who were born in the United Kingdom and for children of white ethnicity wherever born, are shown in fig 1 for all five surveys (1978/79, 1983, 1988, 1993, and 1998). To compare data with previous surveys, these rates are based on children resident in England only. The data for 1978/79 and 1983 exclude children who had previously been treated. However, as this group only accounted for 1% (1978/9) and 2% (1983) of the total eligible cases, their exclusion is likely to have had only a small effect on the rates.
In both white and ISC children, age specific rates fall with every survey except in 1993. In white children, the highest rate in white children is seen in the 0–4 year age group in every survey.
For ISC children in all age groups, rates fell sharply between the 1978/79 and 1983 surveys and then more gradually from 1988. In contrast to white children, the rate in ISC children generally rises with age and is highest in the 10–14 year age group. Thus the 0–4 year 1988 age cohort shows an increase in rate in the subsequent surveys.
Distribution by NHS region (fig 2)
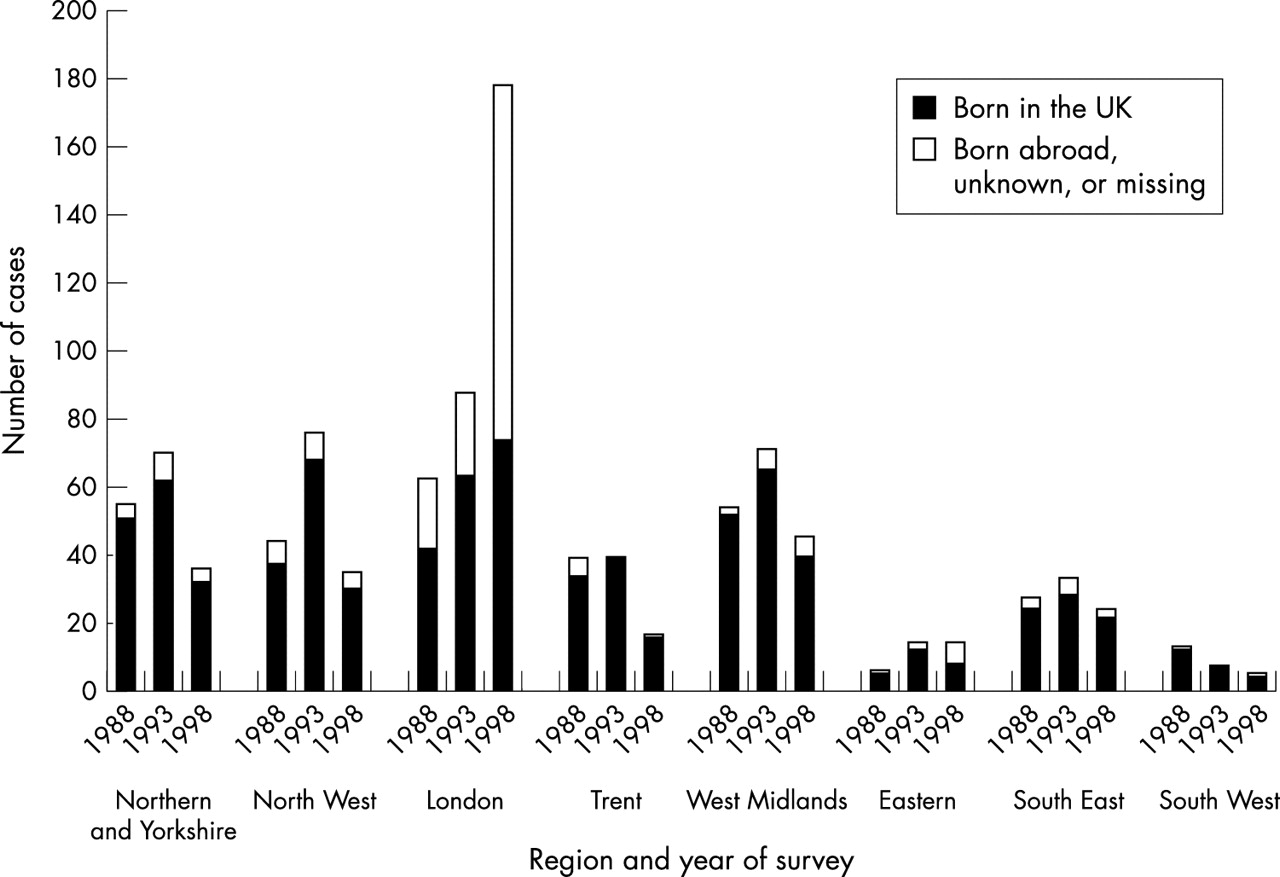
Number of cases of tuberculosis in children in English regions by year of survey and place of birth. Regions are April 1999 NHS regions.
The total number of cases in children in London rose from 63 in 1988 to 88 in 1993 and to 178 in 1998. The rates were 6.7 per 100 000 (95% CI 5.3 to 8.1) in 1993 and 11.9 per 100 000 (95% CI 10.2 to 13.7) in 1998. The proportion of cases in London of white ethnicity fell from 27% in 1988 and 1993 (17 and 24 cases respectively) to 10% (18 cases) in 1998. The rise in cases and the change in proportions within the ethnic groups in London in 1998 are largely related to the rise in black African children; 76 (95%) cases in this group are resident in London. The proportion of cases in London that were known to be born in the UK was 67% in 1988, 72% in 1993, but fell to 42% in 1998. In 1998, 78 (44%) children resident in London were known to be born abroad but only 19 (10%) children resident elsewhere were known to be born abroad.
Site of disease, bacteriology, and clinical investigation (table 4)
Site of disease and number and percentage of specimens and bacteriology results
As in previous surveys, in the 1998 survey only a small proportion (22%) of all children had bacteriological confirmation of disease. Only 207 (57%) children were reported to have had a specimen taken for bacteriology and/or histology. Fifteen children had specimens (12 from peripheral lymph nodes) with histological findings characteristic of tuberculosis, without bacteriological confirmation of the diagnosis.
From comments made on the survey forms, it was reported that for some cases, in which specimens were not obtained, the diagnosis was made on the basis of an abnormal chest x ray and a strongly positive tuberculin (Heaf) test result. At least 74 (20%) children were reported to have been identified as a result of contact tracing. In some of these cases in which no specimens were obtained, culture confirmation in the index case was cited as supporting the diagnosis.
Cases identified through contact tracing were less likely than other cases to have been born abroad, but otherwise they had a similar distribution by ethnic group and site of disease to other cases.
Mycobacterium tuberculosis was the predominant species, cultured in 59, 58, and 61 specimens in 1988, 1993, and 1998. Mycobacterium africanum was cultured in one specimen in 1998 and one in 1993, and Mycobacteruim bovis was cultured from one specimen in 1993 only.
Site of disease by ethnicity in 1998 (table 5)
Sites of disease by ethnic group for cases of tuberculosis in children in the 1998 survey
As in the previous surveys in 1988 and 1993, white children in 1998 had less respiratory disease and more peripheral lymph node disease than ISC or black African children. In total, 14 children had meningeal and/or miliary disease; five were aged under 2 years, two children were aged 2–4 years, two were aged 5–9 years, and five were aged 10–14 years. Three children had both meningeal and miliary disease. All of the 13 children with central nervous system disease were reported to have meningeal involvement.
Drug susceptibility
The number of specimens analysed for drug susceptibility were 49 (82% of all culture positive specimens), 50 (82%), and 61 (75%) in 1988, 1993, and 1998 respectively. We report on resistance to isoniazid and rifampicin only.
In 1988, there were two children with tuberculosis resistant to isoniazid, and no children with multidrug resistant disease. In the 1993 survey, there were three children with mono-resistant disease (two to rifampicin and one to isonaizid). In addition, two children had multidrug resistant disease. Both children were white, born in the United Kingdom, with disease in peripheral lymph nodes. Neither of these children had previous treatment.
In the 1998 survey, one child had disease resistant to isoniazid and one child of ISC ethnicity who had been born abroad and previously treated, had multidrug resistant peripheral lymph node disease.
DISCUSSION
From 1988 to 1998, there was no major change in the overall rate of disease in children (3.3 per 100 000 in 1988 and 3.6 per 100 000 in 1998), although in between these surveys, there was a rise in 1993. As the total number of cases in each survey is small, it is important to ensure that there are no special circumstances that may distort the survey results for a particular year.
The increase between 1988 and 1993 is not restricted to one region (fig 2) and is also seen in the statutory notification reports for children (fig 3).14 The trends in notifications shown in fig 3 indicate that 1993 was the third consecutive year of an increase in notifications. We found no evidence of any relative under-reporting to the surveys; for example, by region, ethnicity, and age, or by survey year. Changes in methodology of the National Survey and in the Labour Force Survey (used for denominator data) may also affect comparisons. Local collection of data by district coordinators in each health authority in the 1998 survey may have affected reporting relative to previous surveys, and hence also the magnitude of the changes seen between 1993 and 1998. There were also changes in design, method, and sampling frame used in the Labour Force Survey when the frequency of data collection changed in 1992 from annual to quarterly, although this should not affect the comparisons from 1993 to 1998.15 There were no unusually large outbreaks involving children in 1993.

{kind=link}
{kind=link}
{kind=link}
Statutory notifications for tuberculosis in children in England and Wales by year.
Among the most important findings over the 10 years is the declining rate in children of both white and ISC ethnicity and the doubling of rate in black African children between each survey. This represents a significant change in the characteristics of the notified population and highlights the value of surveys of this kind.
Two striking changes are the proportion of cases in children who were born abroad (13% in 1988, increasing to 27% in 1998) and the proportion of all cases resident in London (22% in 1993, increasing to 49 % in 1998). In addition, the rate of disease in London increased by 78% from 1993 to 1998.
These results reflect the patterns seen in other developed countries of a rise in the proportion of children born abroad.16,17 The change in the ethnic distribution has also been observed in adults, and may reflect changing trends in migration over this period, suggesting that the rise is partly caused by the diagnosis of prevalent cases of tuberculosis or reactivation of recently acquired infection in new arrivals.5 This adds weight to the importance of new entrant screening, not only in identifying people with disease, but also for identifying people who would benefit from chemoprophylaxis or immunisation. However, even in children born in the United Kingdom, the rates are 19-fold and 25-fold higher in the ISC and black African ethnic groups, compared with the white group. Many of these children may have acquired tuberculosis from local contacts or from visits abroad. Thus these infections are likely to have been amenable to preventative measures such as neonatal immunisation, as well as new entrant screening of adult contacts born abroad. It is important to address the worldwide burden of disease; reducing the mortality and morbidity from tuberculosis in countries of high prevalence with initiatives such as the Global Fund to fight AIDS, tuberculosis, and malaria may also have a subsidiary benefit in reducing infection in new arrivals.
The surveys collect no information on HIV status, but some of the increase in childhood tuberculosis in the black African ethnic group may reflect the greater prevalence of HIV infection in this group with respect to other ethnic groups. Up to June 2001, there were 420 cases of AIDS in children in England and Wales as a consequence of mother to child transmission, of which two thirds were in children of black African ethnicity.18 In 2000, the London region has recommended offering routine HIV testing to all adults diagnosed with tuberculosis (H Maguire, personal communication). This may provide an opportunity to obtain a more accurate assessment of the contribution of HIV to tuberculosis in families.
The increase in incidence with age in children of ISC ethnicity present in the previous surveys has persisted. Thus, despite neonatal immunisation, the 1988 0–4 year age group cohort of children of ISC ethnic origin born in the United Kingdom (fig 1) has not experienced any fall in disease, unlike the parallel cohort of white children. This may be related to poor uptake and the selective provision of neonatal immunisation across districts highlighted in a survey in 1991.11 In addition, it implies that ISC children have an increased exposure to tuberculosis as they get older compared with white children, which is possible given the greater background rate in the ISC community and increasing contact with potentially infectious adults in the UK or abroad. It may be that some ISC children are only identified as having disease when they are screened as part of the schools immunisation programme at 10–14 years, suggesting that the programme may have an additional benefit in identifying children who have tuberculosis.1
The increase in notifications in London partly reflects trends in migration and ethnic demographics. In 1998, 44% of all cases in children in London were known to be born abroad, compared to 10% of cases outside London. However, although the proportion of cases in London known to be born in the UK fell from 67% in 1988 to 42% in 1998, the number of cases in this group rose by 76% during this time. In response to the rise in both adults and children, tuberculosis control was identified as a priority in London. A pan-London tuberculosis group was set up in 1999 and local sector groups are developing various initiatives to improve control such as integrated care pathways, a service standards framework, a pilot of a London-wide tuberculosis register, and a development programme for tuberculosis specialist nurses (H Maguire, personal communication).
As in previous surveys, in 1998, fewer children than adults had disease confirmed by culture or had specimens taken at all, although many of the reports on cases identified through contact tracing cited culture confirmation in the index case as contributing to diagnosis in the contact.5
Pulmonary disease accounted for 48% of cases in 1998, a smaller proportion than in other studies, although the proportion of cases with sputum smear positive disease rose from 13% to 31% of all cases with bacteriology results.19 As in previous surveys, superficial lymphadenitis remains the most common extrapulmonary presentation, and was more common in white children than in other ethnic groups. Mycobacteria other than M tuberculosis can cause higher rates of lymphadenitis, even in areas of high tuberculosis prevalence.20 Although cases were excluded when non-tuberculous mycobacterial disease was cultured in peripheral lymph nodes, it is possible that some of the unconfirmed cases included in the survey are from these species. This would lead to an overestimate of the overall rate and the rate in children of white ethnicity relative to other ethnic groups.
The key trends in childhood tuberculosis described in these surveys are similar to those found in adults with a change in the pattern by ethnic group and increases in cases born abroad and from urban areas.4,5 However, the small rise in overall rate in children from 1988 to 1998 is much less than the rise seen in adults. Furthermore, as disease in children is often a result of recent transmission, the fall in rates in children born in the United Kingdom in the ISC and white subgroups from 1988 to 1998 may reflect improving control of tuberculosis or reduced transmission within the UK.
From 1999, routine surveillance of all tuberculosis cases in England and Wales was enhanced using methodology developed in the 1998 survey. This will make it possible to observe the trends in children and subgroups of children on a continuous basis. By using data from consecutive years, it will be easier to elucidate important trends from the year to year variations, and also to distinguish these trends earlier. Thus the enhanced surveillance will be used to evaluate and inform policy measures, leading to improvements in tuberculosis control and a decline in disease. In the light of the changing distribution of tuberculosis in children and, in particular, the increase in the proportion of cases from ethnic minority groups and born abroad, diagnosis and treatment services must be tailored to enable the most appropriate services to be provided.
Acknowledgments
We acknowledge clinical staff (medical and nursing) contributing the forms in the three surveys, microbiology staff contributing data, district public health staff who collected local survey forms, and survey personnel.