Article Text

Abstract
Aims: To examine the effect of a single dose of human synthetic secretin (HSS) on behaviour and communication in children with autism spectrum disorder (ASD) using an objective measure of communication and social reciprocity and standardised rating scales.
Methods: Randomised, crossover, double blind, and placebo controlled trial of a single intravenous dose of human synthetic secretin (HSS) 2 CU/kg. The 62 subjects (3–8 years) were assigned to group 1 (saline placebo/HSS) or group 2 (HSS/saline placebo). Diagnosis was confirmed by ADI-R (Autism Diagnostic Interview–Revised) algorithm. Severity of symptoms was rated using the CARS (Childhood Autism Rating Scale). Outcome measures included Communication and Symbolic Behavior Scale (CSBS), Ritvo Real-life Rating Scale, weekly Global Rating Scale (GBRS) by parents and teachers, and daily log of gastrointestinal symptoms. The communication subscale of the CSBS, specifying communication function, reciprocity, and social-affective signalling was videotaped and scored by a blinded, trained observer.
Results: Sixty one children completed the study. After randomisation, there were no significant differences in gender, race, age, and parent and teacher GBRS and Ritvo Scale between the two groups. Compared with placebo, secretin treatment was not associated with significant improvement of CSBS standard scores from baseline to 2 or 4 weeks post-infusion. Five children showed clinical improvement in standard scores: two after HSS and three after placebo. There were no significant changes in gastrointestinal symptoms after HSS or saline placebo.
Conclusions: A single dose of intravenous human secretin is not effective in changing behaviour and communication in children with ASD when compared to placebo.
- autistic spectrum disorder
- autism
- secretin
- placebo
- ADI-R, Autism Diagnostic Interview-Revised;
- AE, adverse event;
- ASD, autistic spectrum disorder;
- CARS, Childhood Autism Rating Scale;
- CSBS, Communication and Symbolic Behavior Scale;
- CU, clinical unit;
- GBRS, Global Rating Scale;
- HSS, human synthetic secretin;
- PDD, pervasive developmental disorder
Statistics from Altmetric.com
- ADI-R, Autism Diagnostic Interview-Revised;
- AE, adverse event;
- ASD, autistic spectrum disorder;
- CARS, Childhood Autism Rating Scale;
- CSBS, Communication and Symbolic Behavior Scale;
- CU, clinical unit;
- GBRS, Global Rating Scale;
- HSS, human synthetic secretin;
- PDD, pervasive developmental disorder
A utistic spectrum disorders (ASD) are heterogeneous, complex disorders with deficits in core symptoms of social interaction, communication, and behaviour. Estimates of prevalence rates range from 1 in 1000 to 1 in 160; with most authorities accepting 1 in 500.1 The disorders included in the spectrum (autism, Rett’s disorder, childhood disintegrative disorder, Asperger’s disorder, and pervasive developmental disorder (PDD), not otherwise specified)2 represent a range of severity and underlying aetiologies. Recent research reports implicate a strong genetic predisposition.3 A number of neuropathological abnormalities of prenatal origin have been reported.4 The rate of causally associated medical disorders ranges from 5% to 37%.5,6 In the majority of patients a specific underlying aetiology is not identified. Many untested theories have emerged that purport to explain the core symptoms and associated medical conditions, spawning a range of novel treatments.
Current accepted treatments for children with ASD involve intensive, coordinated programmes of educational, language, developmental, and behavioural intervention.7,8 Evidence gathered over the past 10 years shows that intensive early intervention in optimal educational settings results in improved outcomes in most young children with autism.9,10 Improvements of function may be dramatic; however, complete resolution of symptoms is unusual.11
In 1998 a report on a national television show of the “cure” of a child with autism using secretin precipitated a frenzy of demand for the off-label use of secretin. This programme featured one of three children reported to show an improvement in behaviour following administration of secretin during a diagnostic gastrointestinal procedure.12 The impact of this publicity was magnified by communication through the Internet list serves, chat groups, and support groups to promote this and other treatments. Secretin is one of many treatments that have not withstood the rigour of unbiased study prior to wide dissemination and use. Since the public learned about the purported benefits of secretin treatment a number of well controlled studies have been published (table 1). These studies13–20 have examined the impact of single and multiple dose secretin administration on behaviour in children with autism and uniformly demonstrated lack of efficacy. Despite lack of changes noted by blinded observers on objective measures, parents and other caregivers continue to perceive clinical effects,19 and many families continue to pursue this treatment.21
Peer reviewed studies of secretin treatment in autism
Secretin is a polypeptide (27 amino acids), which is produced in the intestine and released into the bloodstream. It stimulates the release of bicarbonate and water into the duodenum, buffers the acidic contents, and helps pancreatic digestive enzymes work more efficiently. Until recently, physicians primarily used porcine secretin in a provocation test to better characterise gastrointestinal symptoms.22 Porcine derived secretin is given intravenously during gastrointestinal endoscopy for specialised tests of pancreatic function. Doses of 1–2 clinical units (CU)/kg are commonly and safely used in adults (Physicians Desk Reference, 2001). No data are available on the safety of repeated doses. In their series of three patients, Horvath and colleagues12 used a dose of 2 CU/kg of porcine secretin during an endoscopic procedure. They described a decrease in gastrointestinal symptoms and improvement in eye contact, alertness, and expansion of expressive language in the children examined.
The potential mechanism of action of secretin may relate to the presence of secretin receptors in the brains of rats and pigs.23 There is uncertainty about the role of secretin in the human brain. In rats and pigs, the exact role of secretin and of its mechanism of action in the central nervous system has not been determined. The behaviour of rats after secretin infusion has been studied.24 When injected intracerebrally, secretin decreased the locomotor activity of rats. The mechanism for the action of secretin in changing behaviour and function of children with autism is unclear. Some early findings suggest that members of the family of secretin-like hormones may bind to targets in the brain or immune system and result in changes in function or activity.25
The goal of this double blind placebo controlled crossover study was to examine the outcome of synthetic secretin infusion using objective measures of communication and social reciprocity as well as subjective parent, teacher, and clinician rating scales. We designed a 2×2 randomised, crossover, double blind placebo controlled trial of a single intravenous dose of human synthetic secretin (2 CU/kg) in a cohort of 62 children aged 3–8 years. The diagnosis of autism was confirmed by a standardised assessment measure, the Autism Diagnostic Interview–Revised (ADI-R).26 The Communication and Symbolic Behavior Scale,27 which is sensitive to crucial aspects of core symptoms of ASD, was an important outcome measure.
METHODS
Participants
Subjects were 62 children with ASD selected from a convenience sample of 170 families. A total of 98 families completed questionnaires, and 68 children met inclusion criteria (table 2). Diagnosis was confirmed using the ADI-R, a structured parent interview that probes for autistic symptoms in the spheres of social relatedness, communication, and ritualistic or perseverative behaviours. It specifies diagnoses within the autistic spectrum. Two children did not meet the cutoff for ASD using the ADI-R and were excluded.
Exclusion criteria
The nurse coordinator administered the CARS (Childhood Autism Rating Scale)28 as a measure of severity of symptoms of autism. The CARS is a 15 item scale designed to detect and quantify symptoms of ASD. Each item on the CARS is scored on a Likert scale, from 1 (no signs of autism) to 4 (severe symptoms). The maximum CARS score is 60, and the cut off for autism is 30. Scores of 30.5 to 37 are rated as mildly–moderately autistic, and 37. 5 to 60 as severely autistic. The study psychologist determined functional and communicative levels of each child using the Vineland Adaptive Behavior Scales, Interview Edition, Survey form.29 This provided a communication age equivalent and standard score for each child.
Prior to randomisation into a study group, each child underwent laboratory screening tests which included complete blood count with differential, metabolic panel, coeliac panel (serum antiendomysial, antigliadin antibodies, and serum transglutaminase), serum lead, and stool for presence of white blood cells (to rule out inflammatory and infectious pathologies of the intestine). Each family completed a baseline diet record. At baseline, week 2, and week 8 all patients had complete blood count with differential, and a metabolic panel. At each visit a full physical and neurological examination was completed.
One child was excluded because of a lead concentration of 38 μg/dl. Another child was excluded because he had just started a casein/gluten free diet. Two families withdrew before initiation of the study. Thus, the study included 62 children. All parents were informed of the study protocol by the nurse coordinator and written informed consent was obtained from parents. The Institutional Review Board of The Children’s Hospital of Philadelphia approved the study.
Assignment of study drug and treatment procedures
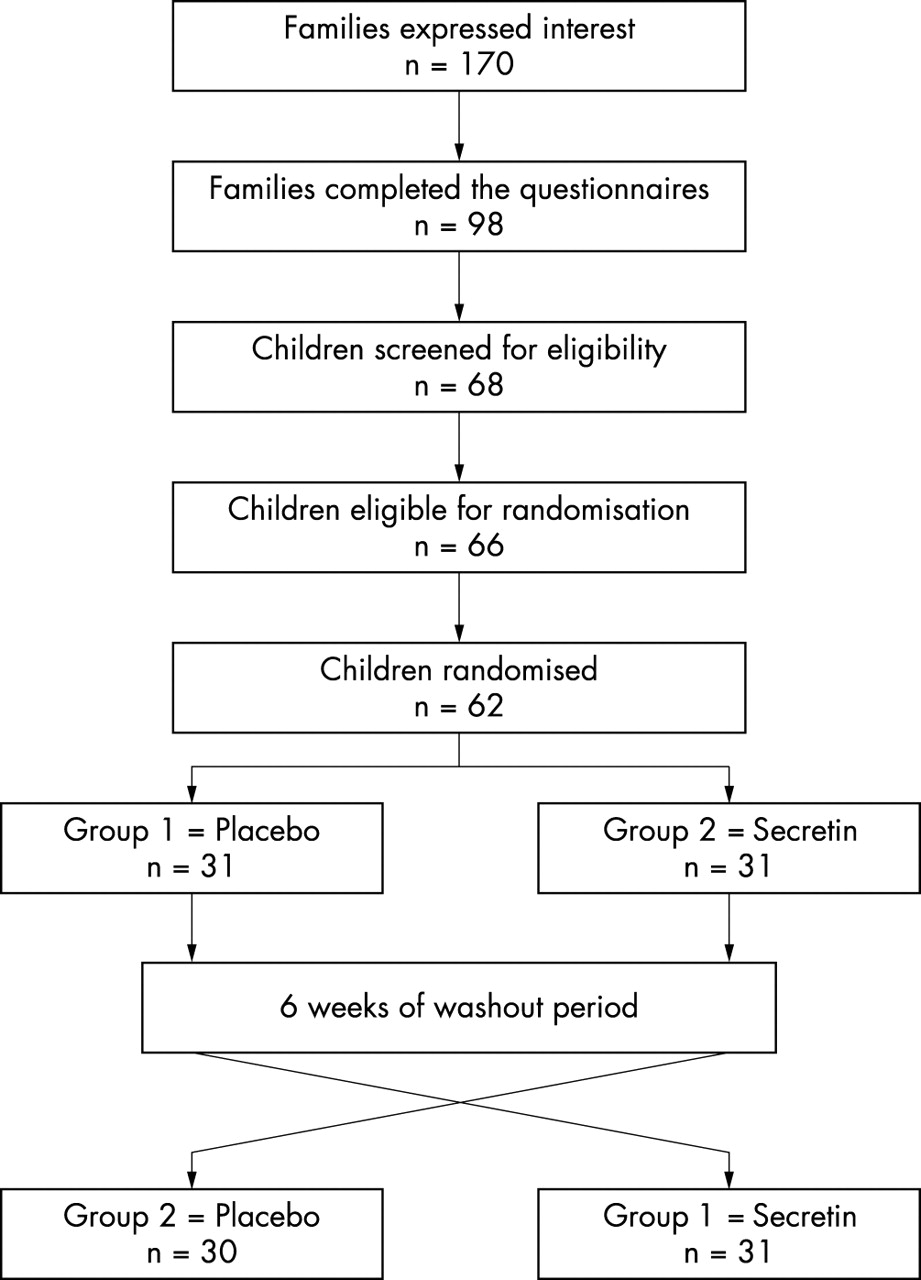
The 62 subjects were randomly assigned to two groups using a computerised randomisation assignment (see fig 1). Group 1 received saline placebo, then crossed over and received human synthetic secretin. Group 2 received human synthetic secretin, then crossed over and received saline placebo. The infusions were separated by a six week washout period. All personnel involved in clinical and neurodevelopmental assessments were blinded to subject’s allocation. The pharmacist and clinical research nurse were not involved in any aspect of the assessments of outcome measures.
{kind=link}
Study design and selection of participants into study.
In this study we used human synthetic secretin (ChiRhoClin, Inc., Silver Spring, Maryland). Participants were fasted for food for four hours prior to receiving each infusion in the Clinical Research Center. Topical EMLA anaesthetic cream (lidocaine 2.5% and prilocaine 2.5% cream, AstraZeneca Pharmaceuticals, LP) was applied locally to two potential intravenous sites by the nurse study coordinator. Each participant was separated from his or her parents during the infusion (since secretin may cause a transient skin rash—the presence of which may unblind the parent to the treatment condition). Vital signs were obtained at baseline, 5, 15, and 30 minutes post infusion. The clinical research nurse placed an intravenous catheter in each child’s arm and a test dose of 0.2 μg was given. If no reaction was noted after one minute, the remaining dose of 2 CU/ kg to a maximum dose of 75 CU was injected slowly over one minute. After five minutes, the participant was returned to his or her parent, and observed closely prior to departure.
Outcome measures
Families and teachers or therapists completed weekly Global Behavior Rating Scales (GBRS). Parents completed a daily log of gastrointestinal symptoms. Study examiners completed the Communication and Symbolic Behavior Scale (CSBS) and Ritvo Real-life Rating Scale30 at baseline and two weeks after each infusion. The occurrence of adverse events (AE) was monitored.
The Global Behavior Rating Scale (GBRS) was devised for this study. It provides a seven point ordinal scale for observers to rate the child’s behaviour over the past week in comparison to his/her behaviour in the week before the initial observations. The ordinal scale was defined as: −3, much worse; −2, moderately worse; −1, little worse; 0, no change; 1, little better; 2, moderately better; and 3, much better. In addition to this rating of general behaviour, parents were asked to rate their child in five additional categories of nighttime sleeping, gastrointestinal symptoms (quality of stools, abdominal pain, vomiting, food variety), daytime wetting, and nighttime wetting.
The Communication and Symbolic Behavior Scale (CSBS)27 is a standardised assessment tool designed to examine communicative, social affective, and symbolic abilities of children. The Communications Temptations section has six selected clusters that can be scored, including communicative function (gestural, vocal, and verbal), reciprocity, and social-affective signalling. These clusters have derived standard scores, with a mean of 10 and a standard deviation of 3. We used the communication composite, which is a sum of the scaled scores for the six selected clusters. The communication composite score was converted to a Language Stage based standard score, with a mean of 100, and standard deviation of 15 (SEM 4.5). The standard score was calculated using the Language Stage of the child, since their chronologic age was greater than 24 months. Language Stages included prelinguistic (0–1 words, 0–1 word combinations), early one-word (2–5 words, 0–1 word combinations), late one-word (6–9 words; 0–1 word combinations), and multiword (10 or more words, 2 or more word combinations).
The Temptations Section of the CSBS was administered to each subject at baseline and 2 weeks ± 4 days post-infusion. Each assessment was videotaped and one therapist, who was blinded to treatment status, scored all the assessments. Two independent clinicians scored 20% of the tapes to provide inter-rater reliability correlation.
The Real Life Ritvo Behavior Scale has five subscales and a global score. The five subscales include sensory motor behaviours, social relations to people, affectual reactions, sensory responses, and language use. Behaviours are coded on a Likert scale (0 = never; 1 = rarely; 2 = frequently; 3 = almost always). Higher scores indicate greater severity of behavioural difficulty. In part II of this study31 we examine factors that parents consider when evaluating progress with novel treatments such as secretin.
Statistics
The two randomisation groups (those receiving placebo first followed by secretin versus those receiving secretin first followed by placebo) were compared on baseline measurements and demographic variables by appropriate statistical tests. Age and CARS total score were compared using the t test for independent samples. Gender, ethnicity, and CARS assessment category were compared using χ2 tests.
Differences between the randomisation groups in various biological parameters were examined using t tests for independent samples or Mann-Whitney rank tests. Chemistry panel and the CBC variables were measured at baseline, at the second week of infusion 1, and at the second week of infusion 2. These Chemistry panel and CBC variables were relatively normally distributed, and the t tests were used to examine differences between groups at each time point separately. The association between occurrence of adverse event and randomisation group was examined using χ2 tests. The primary analyses of this study involved crossover analyses of the Global Behavior Rating Scale (GBRS), the Communication and Symbolic Behavior Scale (CSBS), and the Real Life Ritvo Behavior Scale. The CSBS and the Ritvo were administered at the beginning and at the end of each of the two periods, resulting in a total of four administrations per subject. Change scores were calculated by subtracting the baseline score from the score obtained following treatment, for each of the two periods. The CSBS and the Ritvo change scores were analysed using a SAS Proc Mixed procedure.32 The effects of period, carryover, CARS, CARS-treatment interaction, and treatment were evaluated. CSBS outcome measures included CSBS total standard scores. Ritvo outcome measures included the global Ritvo score. Similarly, repeated measures analysis of covariance were used for the teacher and parent GBRS scores. Summary results of continuous variable are given as mean (SD). Two tailed p < 0.05 were considered statistically significant.
RESULTS
Table 3 shows baseline characteristics of study participants. Subjects were 44–104 months old (mean age 73 months). The sample included 50 males (89.6%) and was 90.3% Caucasian. CARS scores ranged from 28 to 54 (mean 35.8 (SD 5.1)).
Baseline characteristics of study participants
No differences were found between randomisation groups regarding gender, age, and ethnicity. There was a small but statistically significant difference between the two randomisation groups in CARS total score (37.32 (SD 6.23) and 34.31 (SD 3.13), for randomisation groups 1 and 2, respectively; using t test comparing log transformation of the total score, p = 0.020). In addition, CARS assessment was categorised into two groups using 37 as a cut point (<37 = mild/moderate versus ≥37 = severe) and was also significantly associated with the randomisation group, with group 1 having a greater than expected number of severe classifications (χ2 = 10.15, p = 0.003). Therefore, in our analysis, we included CARS category (as a marker for severity) as a covariable.
Over 50% of parents reported gastrointestinal symptoms, including loose stools, constipation, abdominal pain, and severe food selectivity or refusal. There was difference between the groups in distribution of symptoms, and no change in symptoms according to treatment category. SAS Proc Mixed procedure was used to test for the effects of period, carryover, treatment, CARS, and CARS by treatment interaction. The mixed effects model was used to analyse CSBS parent GBRS, teacher GBRS, and Ritvo. Four 2×2 tables (groups × period) were generated presenting means (SD) for CSBS, teacher GBRS, Ritvo, and parent GBRS (table 4). Table 5 presents results from testing the mixed effects models. From this table, the only statistically significant effect was CARS by treatment interaction for parent GBRS (F = 18.30, df = 1,577, p = 0.001), indicating that subjects who had mild/moderate autism tend to do worse with secretin, while subjects having sever autism tend to do better with secretin (table 4D). However, the changes in the parent GBRS scores between the factors are not clinically relevant.
A 2×2 tables presenting sequence by period effects
F statistics with degree of freedom and p values for effects of period, carryover, CARS category (CARS), treatment, and treatment*CARS interaction from SAS proc mixed models analysing CSBS, teacher and parent GBRS, and Ritvo
Biological markers
Differences between the randomisation groups in various biological parameters, chemistry panel, and CBC variables, as well as lead blood, gliadin IgA, gliadin IgG, and tissue transglutaminase, were analysed using appropriate statistical tests. The chemistry panel and the CBC variables were measured at baseline, and weeks 2 and 8. These variables were relatively normally distributed, and differences between the two randomisation groups at each of the time points were examined using t tests (we did not adjust for type I error in this analysis). Measurement of biological markers did not show statistically significant differences before and after infusion in either randomisation group. Blood lead was measured at baseline. Markers for coeliac disease (gliadin A, gliadin IgG, and tissue transglutaminase) were normal in all subjects.
Adverse events
We included temporally associated worsening of behaviour following infusion as an adverse event, while recognising that this begs the question as to whether secretin infusion alters behaviour. AEs included increased liver function tests (n = 3), hyperactivity (n = 2), emotional lability (n = 1), fractures (n = 2), and stomach ache (n = 1). There were a total of nine AEs during the two phases: four during phase 1 and five during phase 2. The nine AEs involved eight subjects, with subject 25 having an AE during both phase 1 and phase 2. There were no differences between the groups in severity, duration, or outcome of AE.
DISCUSSION
This study confirms the outcome of multiple other double blind, placebo controlled studies of the lack of efficacy of secretin in changing core symptoms of autism (table 1). Despite the extensive documentation of the lack of efficacy, reports on the Internet and demand for treatment with secretin still exist, including intravenous, transdermal,33 and sublingual administration.
In this study we attempted to address criticisms of previous studies using secretin as a potential treatment for children with autism. In some of the studies the diagnosis of autism or PDD was made by clinical impression or comparison with DSM-IV criteria or other checklist.14–17 We used the ADI-R to confirm the diagnosis in children previously diagnosed with autism or PDD. In their critique of the study of Sandler and colleagues,14 Horvath et al reported that younger, lower functioning, non-verbal patients with gastrointestinal symptoms were more likely to have a change in gastrointestinal symptoms following secretin administration.34,35 Our subjects showed a range of severity.
Several commentaries have been published implicating shortcomings in selection of outcome measures.36,37 Most of the studies have used combinations of parent questionnaires or diaries, clinical evaluations, and standardised observation tools. The parent questionnaires will address subtle changes parents may detect in their children, but not necessarily core symptoms of autism. Assessment tools, such as the CARS or the Autism Behavior Checklist (ABC)38 are not well suited to assess changes in symptoms of autism. The ABC is a screening tool designed to distinguish children with ASD from those with other disability. The CARS is an observation tool designed to quantify the severity of symptoms of ASD, and there are no standards available to determine the significance in change in the score over time. These measures may not be sensitive enough to detect significant changes in the core symptoms of ASD. Some of the studies included children treated with other medications. The study completed by Chez and colleagues15 included a high percentage of children (80%) receiving centrally acting medication, including anticonvulsants. Finally, most of the studies were completed using porcine secretin, which has a potential for greater side effects, including hypersensitivity.
During the study both parents and study clinicians noted apparent clinical changes in some of the subjects. The outcome measures were selected to examine aspects of social and behavioural skills that have been reported to change with secretin administration—improved eye contact, alertness, and expansion of expressive language,12 and may be more difficult to measure by subjective observation. The CSBS is an ideal tool to quantify changes in core symptoms of autism, including verbal and non-verbal communication, joint attention, three point gaze and others. The combination of parent and teacher/therapist observations makes it more likely to detect subtle changes in the subjects. Despite these different types of outcome measures, no differences could be detected. We tracked gastrointestinal symptoms in the subjects throughout the study. The overall frequency of symptoms (including loose stools, abdominal pain, constipation, and food selectivity or refusal) was high—more than 50% of subjects had symptoms. However, there was no change in frequency of symptoms in subjects after secretin administration, which does not confirm reports from other studies.
Summary and conclusions
A single dose of intravenous human secretin is not effective in changing behaviour and communication in children with ASD when compared to placebo treatment. We do not recommend the use of intravenous human synthetic secretin as a treatment for ASD. Studies documenting lack of efficacy of novel treatments are important tools for educating parents and teachers.
Acknowledgments
This study was carried out with support from the Maternal and Child Health Bureau, Grant No. 2T73 MC 00035 09, the General Clinical Research Center of The Children’s Hospital of Philadelphia, NIH Grant No. RR00240, and Mental Retardation and Development Disabilities Research Center (MRDDRC) NIH Grant No. 3P30 HD26979-04S2. We thank the GCRC nursing staff, Denise DePaul, RN and Ellyn Rebecca, RN, the GCRC medical assistant, Elizabeth Sanchez, and Amy Schwartz for assistance with data entry. We thank the ChiRhoClin Corporation for donating the human synthetic secretin used for this study. Most importantly, we thank the families who allowed their children to participate in this clinical investigation.