Article Text

Abstract
Aggressive early treatment of meningococcal disease can reduce mortality. This relies on prompt recognition and treatment of the complications of septicaemia and meningitis, appropriate ongoing intensive care where necessary, and adequate management of multiple organ failure. Most children with meningococcal disease survive intact, but long term sequelae are increasingly recognised and make follow up essential. New treatments continue to be evaluated, but none has so far proven to be effective in further reducing morbidity or mortality. Simple, timely therapeutic manoeuvres may greatly improve the prospects for survival.
- meningitis
- meningococcal infection
- treatment
- aPC, activated protein C
- BPI, bactericidal permeability increasing protein
- ECMO, extracorporeal membrane oxygenation
- HAS, human albumin solution
- ICP, intracranial pressure
- PEEP, positive end expiratory pressure
- PIC, paediatric intensive care
- PICU, paediatric intensive care unit
Statistics from Altmetric.com
- aPC, activated protein C
- BPI, bactericidal permeability increasing protein
- ECMO, extracorporeal membrane oxygenation
- HAS, human albumin solution
- ICP, intracranial pressure
- PEEP, positive end expiratory pressure
- PIC, paediatric intensive care
- PICU, paediatric intensive care unit
Meningococcal infection remains an important health problem in children, with significant mortality and morbidity. In 2001, 2053 cases of meningococcal disease in children aged less than 15 years were notified to the Public Health Laboratory Service in England and Wales.1
While an effective vaccine is now available to prevent serogroup C disease, there is at present no effective vaccine against serogroup B infection, which is responsible for the majority of cases in the UK.2 Prompt recognition and aggressive early treatment are the only effective measures. This requires immediate administration of antibiotic therapy, and recognition and treatment of patients who may have shock, raised intracranial pressure (ICP), or both.3,4 Encouragingly, mortality has fallen in recent years. This has been caused by various factors such as the centralisation of care of seriously ill children in paediatric intensive care units; the establishment of specialised mobile intensive care teams; the development of protocols for the treatment of meningococcal infection; and the propagation of guidance by the Department of Health and the meningitis charities.5,6
RECOGNITION
The key to improvement in outcome is early recognition of disease and aggressive therapy. The most common features of meningococcal disease are a non-blanching rash, meningitis, and/or septicaemia.7 Up to 20% of cases may have no rash, or an atypical maculopapular rash.8 Meningitis alone is present in about half of patients with meningococcal disease; septicaemia alone is present in about 10%, and 40% have a mixed picture.9
Symptoms of meningitis include headache, fever, vomiting, photophobia, lethargy, and neck stiffness. Over 50% of cases have a rash, and up to 20% may have seizures at presentation. Neck stiffness, photophobia, and a positive Kernig’s sign may be absent, particularly in infants and young children.
Septicaemia is characterised by fever, rash, vomiting, headache, myalgia (especially leg pain), abdominal pain, tachycardia, cool peripheries, and hypotension.
The management of children with low grade fever and petechiae, but without overt shock or meningitis is more contentious. The majority of these children do not have meningococcal disease, but it can be difficult to distinguish the early stages of meningococcal disease from more benign conditions such as viral infections, particularly when myalgia is a prominent symptom. It has been proposed that the absence of irritability, lethargy, or decreased peripheral pefusion makes meningococcal disease unlikely.10 However, in our opinion this still risks missing some early cases, and every child with a fever and petechiae should be assumed to have meningococcal disease until proven otherwise. Progression of the disease may take only a few hours, and parents of children who appear well and are sent home with symptoms that appear to be caused by viral infection, should always be told what new symptoms to look out for, and be encouraged to seek further medical attention if there is any change or deterioration in their child’s condition.
Because of the need for immediate institution of treatment in suspected cases, laboratory results are not usually available rapidly enough to help in the initial clinical diagnosis. Even if available, laboratory results may not be helpful in distinguishing meningococcal from viral disease, particularly as in early or fulminant infection, markers such as white blood cell count, C reactive protein, and lumbar puncture may be normal, and thus offer false reassurance.11
PREHOSPITAL MANAGEMENT
Children suspected of having meningococcal disease should immediately be given parenteral penicillin, unless they have a history of previous anaphylaxis to penicillin.12 They should be referred to hospital without delay.
INITIAL ASSESSMENT AND MANAGEMENT IN HOSPITAL
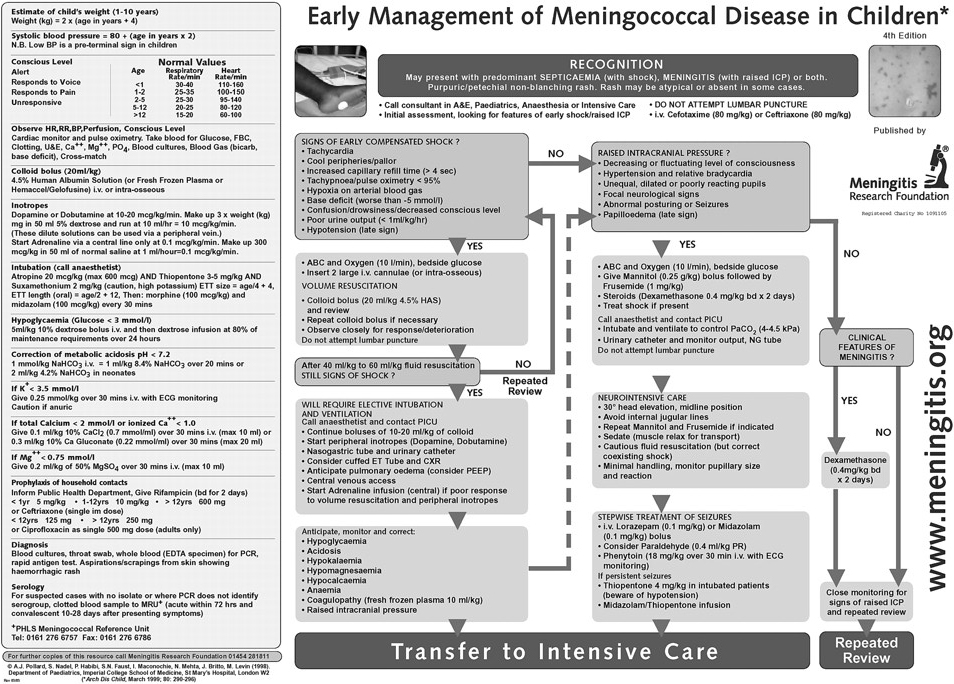
Figure 1 presents a protocol for early management of meningococcal disease in children.
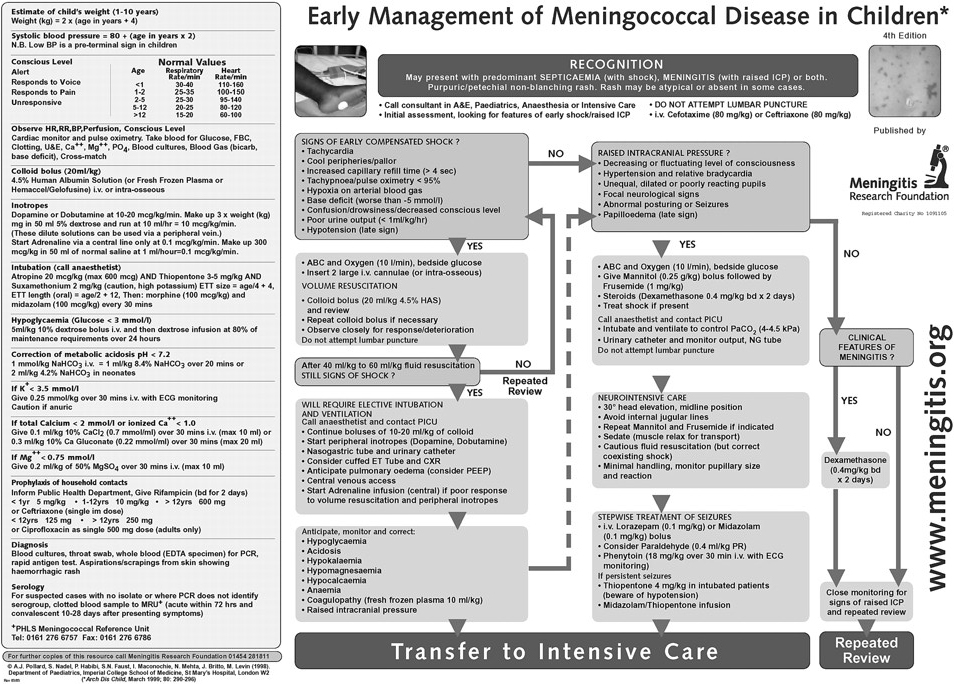
Protocol for early management of meningococcal disease in children.
Immediate assessment
Children with meningococcal disease may develop shock and/or raised intracranial pressure (ICP), which may evolve and progress very rapidly. The responsible consultant should be involved in their management from the outset, and paediatric intensive care (PIC) advice should be sought early. When the diagnosis is suspected, antibiotics should be given promptly (intramuscular or intravenous penicillin or a third generation cephalosporin). Immediate evaluation of airway, breathing, and circulation should be made, high flow oxygen should be given by facemask, and resuscitation instituted as indicated. Intravenous access should be obtained as soon as possible.
Evidence of shock (predominant in septicaemia) and raised intracranial pressure (predominant in meningitis) should be sought urgently.
Diagnostic samples
Blood culture should ideally be taken at the time of intravenous cannula insertion, prior to giving antibiotics. However, on no account should treatment be delayed to allow cultures to be taken. Antibiotics may have been administered before coming to hospital, which may make culture diagnosis even less sensitive. Other useful samples for diagnosis are: an EDTA sample of blood for polymerase chain reaction for meningococcal DNA, serum for latex agglutination test, and acute serology, which should later be paired with a convalescent sample, culture of throat swab, and microscopy and culture of skin scrapings from areas of purpura.13,14
Lumbar puncture should only be done if the recognised contraindications are absent.15 There is some disagreement about when lumbar puncture should be performed.16,17 It may be dangerous in the presence of shock, raised ICP, and coagulopathy, and is unlikely to alter initial management. It is only really helpful in cases where the diagnosis of meningitis is in doubt, or in those with clinical meningitis without any obvious aetiology, or children in a high risk group for meningitis with an unusual organism (that is, neonates, the immunocompromised, or those with ventriculoperitoneal shunt, head trauma, or anatomical defects). It should never be performed in children with circulatory compromise or any evidence of raised ICP.18
Recognition of shock
Recognition of shock and prompt treatment are vital, and may be lifesaving (see fig 2). Shock is recognised by the development of increased heart and respiratory rate for age, unexplained metabolic acidosis, reduced urine output, hypoxia and often an alteration of mental status, all of which result from reduced end organ perfusion. Prolonged capillary refill time and cool skin and peripheries will be present, but are relatively non-specific signs of compensated shock. Hypotension is a late sign. Children are able to compensate for the loss of up to 25–40% of their blood volume without developing hypotension, and therefore may have normal blood pressure until shock is advanced.19 Preservation of higher mental function may occur, despite decompensated shock, which may make observers underestimate the degree of cardiovascular collapse. In addition, depressed mental status will occur in patients with raised ICP, who may also have poor peripheral circulation because of altered brain stem function. This may be confusing even to experienced medical practitioners. However, in the presence of raised ICP, blood pressure is usually normal or high, with a normal or relatively slow heart rate for age. These signs, together with the absence of a metabolic acidosis, usually distinguish raised ICP from shock.20–22

{kind=link}
{kind=link}
Clinical mechanisms of shock and the sites of action of treatment.
The pathophysiology of shock in meningococcal septicaemia is discussed in detail in another article in this series.23
Treatment of shock
Treatment of shock requires rapid stabilisation of the airway and breathing, intravenous access, and replacement of circulating volume. Initially, a bolus of 10–20 ml/kg of fluid should be given rapidly (over five minutes). This may improve objective measures of circulation, such as heart rate, urine output, metabolic acidosis, and skin perfusion. It should be followed by immediate re-evaluation of airway, breathing, and circulation, and administration of further boluses of fluid if signs of shock persist.24 Large volumes of fluid resuscitation may be required, as increased vascular permeability means that fluid administered for resuscitation will continue to extravasate. Up to 60 ml/kg of fluid may be given in the first hour without increasing the risk of cerebral or pulmonary oedema.25
Much controversy surrounds the optimal resuscitation fluid for critically ill childen. Until 1998, 4.5% human albumin solution (HAS) was widely, although not universally, used. In that year, a systematic review of studies which evaluated the use of albumin or crystalloid as resuscitation fluid in various clinical settings suggested that mortality was higher when albumin was used.26 None of the studies was in children with sepsis, and other systematic reviews have shown conflicting results.27 No properly conducted studies of the optimal resuscitation fluid for children with septic shock have been performed. In our, and others’ experience of using 4.5% HAS in children with meningococcal disease, there has been a demonstrable significant reduction in mortality.4–6 In addition, it has been shown that crystalloid solutions rapidly leak from the circulation, even in the normal state, and therefore their circulatory expanding effects are, at best, short lived in sepsis.28 We continue to use and to advocate the use of 4.5% HAS for volume resuscitation in children with meningococcal sepsis.
If shock persists after the administration of 40 ml/kg of fluid within an hour, further fluid administration will be required to optimise circulating volume. Endotracheal intubation and mechanical ventilation will be required to protect the airway and maintain adequate oxygenation and ventilation, as pulmonary oedema is likely to develop. In addition, early, elective intubation and ventilation improve the outcome of septic shock and reduces the risk of fulminant pulmonary oedema developing by the use of adequate positive end expiratory pressure (PEEP).29 Experienced anaesthetic support should be sought for intubation in a shocked child, and transfer to intensive care will be required. An inotrope such as dopamine or dobutamine may be advisable, and is safely commenced via a peripheral cannula to support the circulation prior to tracheal intubation, as rapid sequence induction may precipitate a dramatic fall in blood pressure in a child with hypovolaemia. If circulatory instability persists following intubation, adrenaline or other vasoactive agents may be safely started once central venous access has been established.
Other complications that may arise during the initial resuscitation include: hypoglycaemia, metabolic acidosis, hypokalaemia, hypomagnesaemia, hypocalcaemia, anaemia, coagulopathy, and raised ICP.30 These should be actively sought and treated simultaneously with fluid resuscitation if found to be present.
Recognition of raised intracranial pressure
Patients with meningococcal meningitis, rather than septicaemia may develop raised ICP.
Evidence of raised ICP includes: fluctuating or deteriorating level of consciousness; normal or high blood pressure in the presence of a slow or normal heart rate; unequal, dilated, or poorly reacting pupils; focal neurological signs, or abnormal posturing; seizures; and papilloedema. One confounding factor is that a decreased level of consciousness may occur in shocked patients because of cerebral hypoperfusion, or because of hypoglycaemia. However, the level of consciousness should improve in these conditions once the cause has been treated.
Care should be taken not to confuse the poor peripheral circulation seen in shock (see above), with the vasoconstriction often seen with raised ICP, where abnormal neurology may be associated with delayed capillary refill time without evidence of shock. In this circumstance, when poor peripheral perfusion is associated with absence of a metabolic acidosis in blood gases, together with relative bradycardia, normal or high blood pressure, and other neurological signs, it should be assumed that abnormal neurology is caused by raised ICP.22
Treatment of raised intracranial pressure
Patients with clinical evidence of raised ICP require intervention to attempt to optimise cerebral perfusion. They should have their airway protected by tracheal intubation, and breathing controlled by mechanical ventilation to keep the partial pressure of carbon dioxide (pCO2) in the normal range. In the absence of shock cautious diuretic therapy using mannitol and furosemide may reduce cerebral oedema and improve cerebral blood flow. Cautious fluid restriction may be useful, but fluid balance requires careful monitoring, and any coexisting shock should be treated aggressively.15,31
Any seizures should be treated according to standard protocols.20 Lumbar puncture is contraindicated in patients where raised ICP is suspected.
TRANSFER TO INTENSIVE CARE
Initial resuscitation and stabilisation inevitably take place at the hospital where the child first presents. Following this, some patients will require transfer to a regional paediatric intensive care unit (PICU). Early discussion is advisable to facilitate optimal treatment, and to identify which patients will need transferring. These will be children who require intubation and ventilation for persistent shock after administration of 40 ml/kg of fluid within an hour, or who require ongoing treatment of raised ICP. These patients require a secure airway, controlled mechanical ventilation, and secure central venous and arterial access for ongoing cardiovascular support and monitoring. Because of the potential instability of these children, transport should only be carried out by specialised and experienced personnel. Because much of the intervention occurs at the admitting hospital, early and frequent discussion with the regional PICU is desirable, before the transfer team arrives.32
ONGOING MANAGEMENT
The principles of management in intensive care are the same as those during initial resuscitation, and attention to maintaining the airway, breathing, and circulation are most important. Shock, multiple organ failure, and raised ICP remain the main complications. Each organ system requires careful attention.
Airway
Maintenance of a secure and appropriately sized airway remains paramount. Reintubation may be hazardous because of fulminant pulmonary oedema and coagulopathy. It is therefore mandatory that the initial intubation should be with an appropriately sized and sited endotracheal tube. Because of the likelihood of development of pulmonary oedema, often requiring the use of high ventilation pressures, a cuffed endotracheal tube of appropriate size is optimal in all age groups.
Breathing
Pulmonary oedema often occurs early in meningococcal disease, even before fluid resuscitation takes place, because of the presence of increased vascular permeability and myocardial dysfunction. Pulmonary oedema may be exacerbated by the administration of large volumes of resuscitation fluid. There is no evidence that either crystalloid or colloid resuscitation fluid is any more effective in the prevention of extravascular fluid accumulation in the lung. Treatment of pulmonary oedema requires ventilation with high PEEP to maintain adequate oxygenation. Breathing may be further compromised by pleural effusion, or splinting of the diaphragm by ascites. If severe, these may be relieved by drainage.
Circulation
Further fluid boluses may be required to optimise intravascular volume, and the need for these may be guided by central venous or pulmonary capillary wedge pressure measurement. In addition, impaired myocardial contractility and vasoparesis may require high dose vasoactive drug administration, usually with adrenaline or noradrenaline. However, shock may be unresponsive to high dose inotropes. There is some evidence that refractory shock may be more common in children with impaired adrenal gland responsiveness.33,34 We advocate the use of hydrocortisone (1 mg/kg six hourly) in patients with a poor response to high doses of vasopressors. This is distinct from the use of high dose dexamethasone in the treatment of meningitis (see below). There is no evidence to suggest that use of high dose corticosteroids is beneficial in the treatment of septic shock.35 Efforts to improve the circulation in refractory shock also include the use of experimental agents or modes of therapy (see below).36
Neurological
Patients who have raised ICP require neurointensive care as described above; other patients require continued vigilance for the development of raised ICP. Seizures or focal neurological signs should be sought, which means that muscle relaxants should be used cautiously. Long term neurological effects of meningitis, such as hemiplegia, ongoing seizures, or deafness may become apparent while on the intensive care unit. There are no properly conducted studies of the use of high dose steroids in meningococcal meningitis. However, their use has been shown to reduce hearing loss and other neurological sequelae in other forms of bacterial meningitis.37,38 We use high dose steroids in children with clinical evidence of meningitis without shock, even if they have not had a lumbar puncture.
Metabolic
Multiple electrolyte and glucose derangements may be ongoing and require frequent monitoring and correction. Hypoglycaemia, hyperglycaemia, acidosis, hypokalaemia, hypomagnesaemia, and hypocalcaemia may all need treatment as during the acute presentation. Aggressive correction of metabolic derangements is required to maintain the correct milieu for optimal organ function.
Renal
Acute renal insufficiency may occur, initially as a result of renal hypoperfusion. Most children with shock are oliguric until circulation is restored by adequate fluid resuscitation and inotropic support. If these measures are unsuccessful, or in the presence of severe intractable pulmonary oedema, massive fluid requirements, or severe metabolic derangements, then renal replacement therapy with either haemofiltration or acute peritoneal dialysis may be required. The routine use of high volume haemofiltration in children with sepsis has not been properly studied. Very rarely, long term renal replacement therapy may be required.
Coagulation and haematology
Anaemia, thrombocytopenia, and coagulopathy are common, and transfusions of red cells, platelets, and fresh frozen plasma are frequently required. The understanding that the function of the protein C pathway is deranged in children with meningococcal disease suggests that the use of activated protein C (aPC) may be a logical therapy for children with meningococcal septic shock.23,39 However, there is a likelihood of an increased risk of severe haemorrhage with this treatment, and the routine use of aPC cannot be recommended. A placebo controlled randomised trial of aPC in children with sepsis is now underway.
Skin/limb perfusion
Limbs or areas of skin with extensive purpura may become necrotic. In addition, hypoperfused areas of skin are vulnerable to pressure damage. Compartment syndrome may threaten the blood supply of underlying muscle. Advice from orthopaedic and plastic surgeons may be needed for limb salvage. Fasciotomy and amputation should not be considered until it is felt to be absolutely necessary, and only performed following extensive multidisciplinary discussion.40
Gastrointestinal
Maintenance of enteral feeding is desirable wherever possible, but the combination of gut ischaemia, intestinal oedema, and ascites may make this impossible, and parenteral nutrition may be required. The failure of nasogastric feeding should prompt the consideration of nasojejunal feeding, which in our experience is usually successful.41
MEDIUM TERM COMPLICATIONS ON INTENSIVE CARE
Patients in intensive care are vulnerable to nosocomial infection and iatrogenic complications. Children ventilated for long periods of time may require tracheostomy, and those with multiple organ failure may require long term organ support.
It has recently been recognised that severe psychiatric problems such as the post-traumatic stress disorder may occur both in the affected child and commonly in their parents.42 Appropriate psychological support should be provided for these families.
TREATMENT ON A GENERAL PAEDIATRIC WARD
Patients who have no evidence of shock or raised ICP, or who have responded rapidly to initial treatment of these complications, may be managed on a general paediatric ward. Ideally however, they should be placed on a high dependency unit, at least for the first 24–48 hours of their illness. Shock and/or raised ICP may develop later, or may deteriorate again following initial improvement. These children therefore require very close observation, and monitoring of their pulse, blood pressure, respiratory rate, urine output, and conscious level.
ONGOING WARD MANAGEMENT AND MEDIUM TERM COMPLICATIONS
Children with uncomplicated disease require seven days treatment with intravenous antibiotics. Those treated with third generation cephalosporins require no further treatment; those given only penicillin also require oral rifampicin to eliminate nasopharyngeal carriage. The index case remains infectious, requiring isolation for 24 hours after receiving intravenous ceftriaxone or cefotaxime, or until given oral rifampicin. The consultant in communicable disease control should be notified, and close contacts should receive antibiotic prophylaxis and immunisation if indicated.
Children who have not required intensive care may be well enough to go home after a few days, and depending on community nursing arrangements, many can complete their intravenous antibiotic course at home.
Medium term complications that may be encountered prior to discharge include neurological sequelae, lack of resolution of fever, secondary fever, secondary rash, arthralgia, and antibiotic side effects. Fever should always prompt a search for ongoing or secondary sepsis. Neurological signs or seizures following meningitis need careful evaluation and imaging. Rash and arthralgia may be caused by immune complex disease and may respond symptomatically to non-steroidal anti-inflammatory agents.
NEW TREATMENTS
Early recognition, antibiotics, prompt treatment of shock and raised ICP, and supportive intensive care are still the mainstays of treatment for meningococcal disease. Because of the continued high mortality, attempts to improve outcome have focused on development of adjunctive treatments that may modulate the inflammatory process. The most promising treatments that have been or are being evaluated include the antiendotoxin agents (for example, bactericidal permeability increasing protein (BPI)),43 agents which may inhibit both the activation of coagulation and inflammation (for example, activated protein C),44,45 and methods to remove cytokines and other inflammatory mediators (for example, high volume haemofiltration), but none is yet part of routine clinical practice. There is some anecdotal experience with potent vasopressors such as angiotensin II, vasopressin, and the nitric oxide antagonists in refractory shock. However, experience with these agents is limited, and routine use cannot be recommended. The use of extracorporeal membrane oxygenation (ECMO) for septic shock has fallen out of favour despite initial reports of success.36
FOLLOW UP AND LONG TERM COMPLICATIONS
Most patients who survive meningococcal disease make an excellent recovery. However, about 5% have neurological sequelae, most commonly sensorineural deafness, and all patients should have a hearing test.46 Another 2–5% may suffer from limb or digital ischaemia leading to amputation, or severe skin necrosis requiring grafting. Rarely, there may be long term renal or myocardial dysfunction. Children who have had limb amputations or neurological sequelae require long term multidisciplinary rehabilitation.
Defects in the terminal or alternative complement pathways are known to predispose to meningococcal disease, but most patients with meningococcal disease have no underlying immune deficiency.47 However, we recommend screening for complement and antibody deficiency in convalescence, in an attempt to reduce the likelihood of a second episode of life threatening sepsis.
CONCLUSION
The outcome of meningococcal disease has improved in recent years as a result of improvements in the recognition, resuscitation, stabilisation, transfer, and ongoing care of these children. However, despite these improvements, meningococcal infection remains the main infectious cause of death in children in the UK. Introduction of serogroup C conjugated meningococcal vaccine has been an impressive success, but the challenge remains to develop an effective serogroup B vaccine which will prevent the majority of meningococcal infections in the UK. Worldwide, an effective and affordable multivalent vaccine is the goal for the prevention of this devastating disease.
In the meantime, careful clinical assessment to recognise the disease in its early stage, prompt antibiotic treatment, together with aggressive resuscitation of shock and management of raised ICP, are necessary to provide the best chance of a good outcome.
FURTHER INFORMATION
A flowchart summary of the early management of meningococcal disease (fig 1 in this paper), can be found at the website of the charity and patient support organisation Meningitis Research Foundation (MRF) at www.meningitis.org.
Key points
-
Suspect meningococcal infection in all children with petechiae and fever, but remember that some cases will not have a typical rash
-
Treat immediately with antibiotics
-
Pay attention to airway, breathing, and circulation
-
Assess for shock and raised ICP and treat these early and aggressively
-
Senior doctors should be involved early
-
Early contact with the regional paediatric intensive care unit should be established
-
Large volumes of resuscitation fluid may be required for shocked patients. The choice of fluid is controversial, but we recommend 4.5% human albumin
-
High dose steroids may be useful in patients with meningitis and no evidence of shock
-
Patients who do not require intensive care should be monitored closely for the first 24–48 hours, ideally on a high dependency unit
-
Remember to notify public health and arrange prophylaxis for contacts
-
New adjunctive treatments are under investigation
-
All children who have had possible or suspected meningococcal disease should have a hearing test
Further information can also be found from the National Meningitis Trust at www.meningitis-trust.org.uk and PHLS at www.phls.co.uk.
Acknowledgments
We gratefully acknowledge our colleagues who have been instrumental in developing our current thoughts on the management of meningococcal disease, in particular Professor M Levin, Dr P Habibi, Dr C De-Munter, Dr J Britto, and the nursing staff of the paediatric intensive care unit. We are grateful to the Meningitis Research Foundation for the printing and dissemination of the St Mary’s treatment protocol and for their continued support. Steven Welch is supported by a grant from Children Nationwide. Simon Nadel is participating in EUMENNET (the European Meningococcal Network Study), funded by an EU grant, and has received travel sponsorship from Eli Lilly, the makers of aPC.