Article Text

Abstract
Aims: To establish the prevalence of behaviour problems and the level of interest in parenting programmes in a population sample of parents of children aged 2–8 years, and to assess to what extent they are associated with socioeconomic factors.
Methods: Postal survey of parents of children aged 2–8 years registered with three general practitioner surgeries; 70% response rate.
Results: One fifth of parents from this population sample were experiencing difficulties with their children’s behaviour. While behaviour problems were more prevalent in the manual social classes, “need” was high across all social groups. Just under a fifth of parents reported prior attendance at a parenting programme and 58% expressed interest in attending in the future. Interest in attending a parenting programme was not class related, but was predicted by the age of the eldest child and the existence of behaviour problems.
Conclusion: Behaviour problems are an important public health issue. Findings support the use of a non-selective approach to the provision of parenting programmes in the UK.
- behaviour problems
- parenting programmes
- survey
- general practice
Statistics from Altmetric.com
Parenting is important for child health and development, particularly the development of good mental health. In the UK, publicly funded health services have been provided to advise, educate, and support mothers for over a century. In the past, advice has focused on the physical aspects of parenting. More recently, the socioemotional aspects have also been emphasised. Mental health promotion is now a national priority and support for parents is recognised as an important element of public health policy.
During the past decade a range of interventions have been developed to help parents improve their parenting. One common approach consists of parenting programmes for groups of 8–12 parents, meeting for two hours weekly for 10–12 weeks. A number of controlled trials1,2 and systematic reviews3–,5 have shown that these groups can improve parenting, the mental health of parents, and the emotional and social development of children.
One argument which has been raised against a population based approach to the provision of parenting programmes is that this would attract parents least in need—that is, those from more highly educated “middle class” families with little evidence of child behaviour problems, while uptake would be poor among families most in need.6
We have investigated the extent to which interest in attending parenting programmes is determined by factors such as socioeconomic status, educational level, and the presence of behaviour problems among the children, in a survey of a representative sample of parents of 2–8 year olds in Oxford.
METHODS
Survey
In July 1999, parents of all children aged 2–8 years inclusive, registered at three general practices in Oxford City, were invited to complete a postal questionnaire for each of these children. The three practices were selected because the sociodemographic characteristics of their patients mirrored those of the general population in the City of Oxford, and because the three practices together serve a discrete geographical area in Oxford. They did not have any practice based parenting groups established at the time of the survey. Questionnaires were mailed to a total of 1155 families with 1788 children. Two further reminder letters and questionnaires were sent to non-responders at three-week intervals. Questionnaires were returned from 800 families, providing data on 1105 children. Sixty three children whose questionnaires were returned marked “not known at this address” were excluded, giving an overall response rate of 70%. A small number of questionnaires were not fully completed, leading to some missing data. The number of responses on which analyses were carried out is indicated by “n” in each table.
Behaviour screening questionnaire
The Eyberg Child Behavior Inventory (ECBI)7 was used to measure children’s behaviour. This parent report measure includes a range of behaviours likely to be present in a child with behaviour problems, and can compare behaviour problems in different populations over time. It is suitable for children aged 2–16 years, and includes items such as “steals” and “gets angry when doesn’t get his/her own way”. The inventory enumerates the number (problem scale) and frequency (intensity scale) of the problem behaviours. It has been shown to be valid and reliable.8
Parents were asked about their marital status, occupation, age at leaving education, accommodation (privately owned, rented, or other), and ethnicity. Data were also collected concerning the child’s age, sex, and position in the family, and previous treatment for behaviour problems.
The social class of the respondent, and their partner where applicable, were coded using the Registrar General’s Social Class Classification.9 Where the respondent and partner’s class differed, the household was classified using the higher category. Parents were also asked to record their age at leaving education and their housing tenure.
Parents’ experience of, and interest in, parenting groups were assessed using the questions: “Have you ever been to a course or a group involved in talking about bringing up children?” (Yes/No); and “Would you be interested in meeting other parents with children of about the same age to talk about children’s development or behaviour, and share skills and tips in coping with children?” (Yes/No/Maybe).
Questionnaire data were coded and entered into SPSS version 9.0. Statistical analyses were carried out using χ2 tests. A logistic regression analysis was carried out with the age of the eldest child, sex, social class, housing tenure, age at leaving education, ethnicity, and the presence of behaviour problems to assess the relative power of these variables in predicting parental interest in attending a parenting group.
RESULTS
The sample
Data on social class was provided by only 700 of the 800 responding families. Among those who completed this question, manual social class parents (27.6%) were under represented in comparison with the population of both Oxford (42.2%) and England (46.3%) recorded in the 1991 census. However, only 31.7% of these parents without social class data left education at 18 or older compared with 48.4% of parents overall in the sample; 23.1% of them were single parents compared with an overall figure of 13.7% single parents in the sample. Thus this apparent under representation may reflect the fact that missing data is more likely among people with lower occupational status. The proportion of families living in rented accommodation was typical of England, but not of Oxford City, which has a higher than average level of rented accommodation because of the high student and visiting academic population. Parents from minority ethnic groups, however, were over represented (13.4% v 8.1% and 4.4%; table 1⇓). Age at leaving education was completed by a higher proportion of respondents than social class: 379 (49.9%) reported leaving education at age 17 or younger and 381 (50.1%) at age 18 or older. Children from single parent families (15.4%) were well represented. This figure (which covers families with children age 2–8 years only) compares well with 1991 census data for England, in which 18.0% of households containing children aged under 16 years were single parent families.
Sociodemographic characteristics of responding families compared with households in Oxford City and England (1991 census)
Childhood behaviour
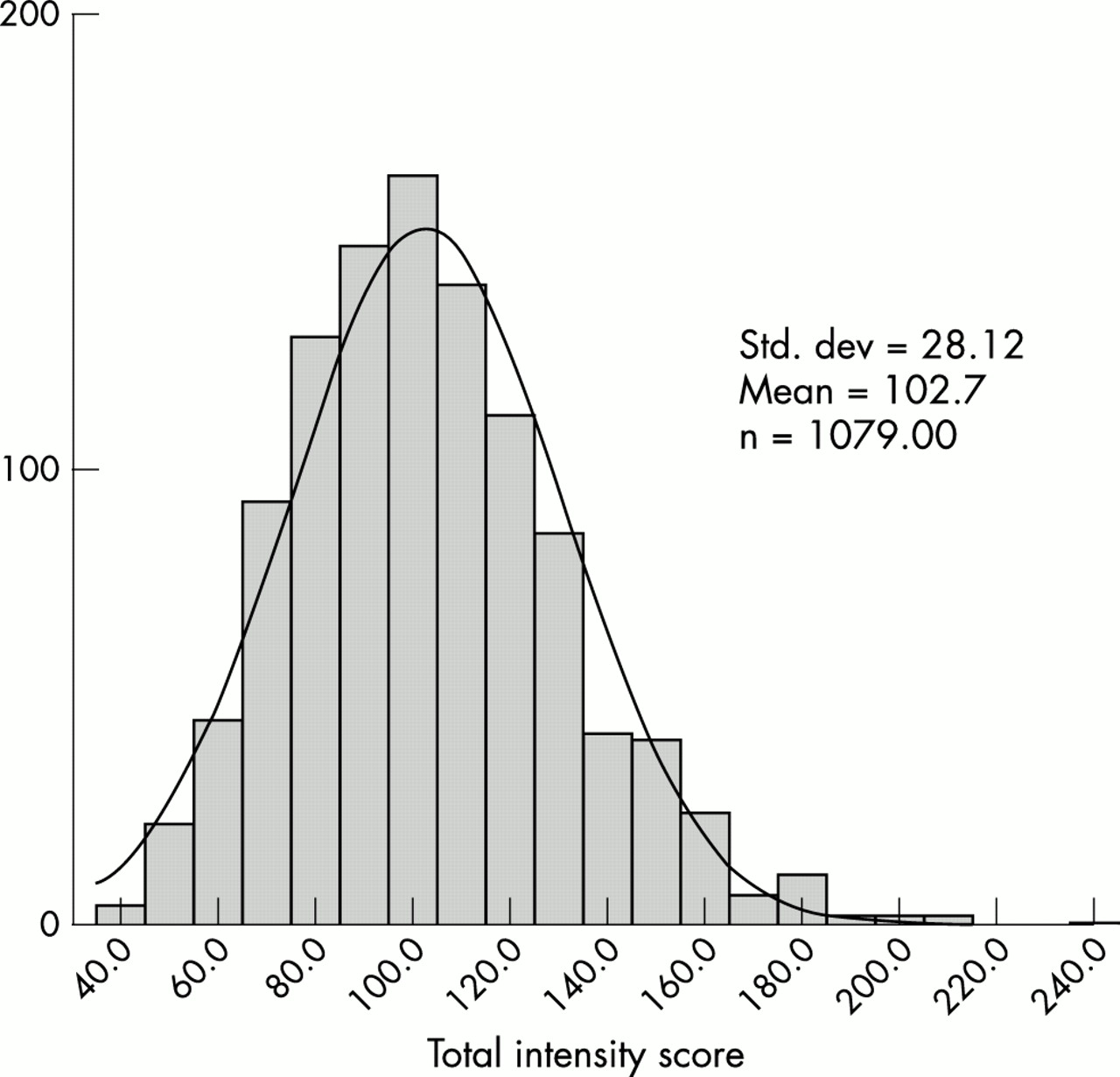
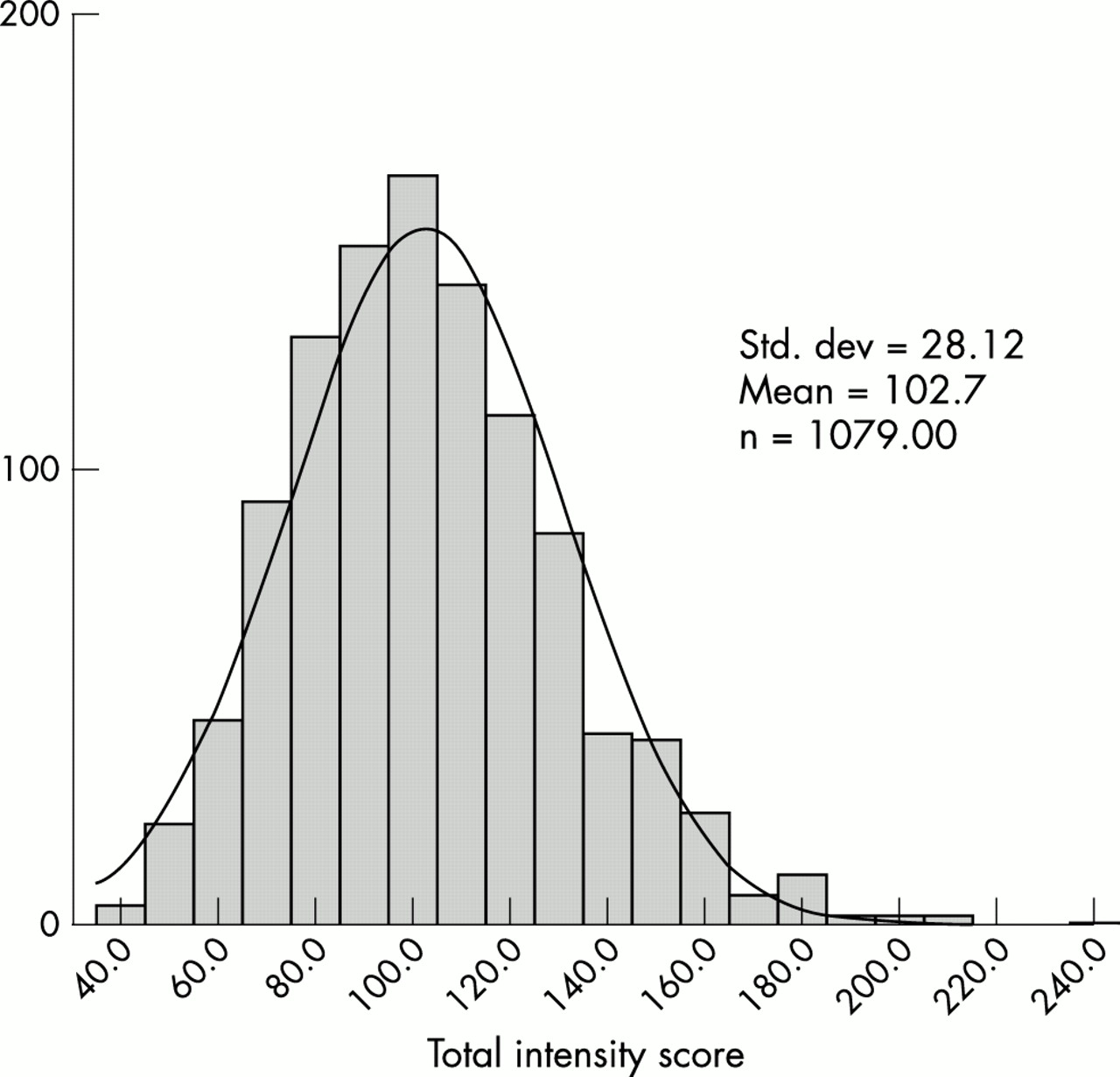
Scores for children on the Eyberg Intensity Scale were normally distributed, with a mean of 102.7 and a standard deviation of 28.1 (fig 1⇓). Using a cut off point of 127 as recommended by Eyberg,7 approximately one fifth of children (17.9%, n = 193) were defined as having a behaviour problem of clinical severity on this scale. Almost twice as many boys (22%, n = 113) scored in the clinical range as girls (14%, n = 80) (p = 0.001).
{kind=link}
Distribution of Eyberg Intensity scores.
The parents of children scoring in the clinical range on the intensity score were more likely to be manual social class (34.4% (n = 65) v 21.3% (n = 106) in non-manual classes) and to have left education at age 17 or younger (28.8% (n = 107) v 21.1% (n = 79) in those leaving at 18 years or more). Children with behaviour problems were also more likely to be living in rented accommodation (34.5% v 19.7% of children in owner occupied accommodation). There was no significant difference in the proportion of children with behaviour problems in one (26.1%) and two parent families (24.2%).
The mean score on the problem scale was 5.6 with a standard deviation of 6.4. The distribution was skewed, with scores ranging between 0 and 35.
Scores on both the intensity and problem scales peaked at age 3. One in four (24.5%, n = 35) 3 year olds scored in the clinical range on the intensity scale compared with one in seven (13.8%, n = 18) aged 2 years, one in five (19.2%, n = 32) at age 4, and one in six (15.6%, n = 26) at 8 years of age. On the problem scale, 9.1% (n = 11) of children were reported as having problem behaviour at 2 years, compared with 20.0% (n = 176) between the ages of 3 and 8 years.
Approximately 3% of children (n = 27) had undergone previous treatment for behaviour problems. Such children were more common among the manual social classes (6.3%, n = 12) than in the non-manual social classes (2.3%, n = 10) (p = 0.004). Two thirds of the children (62.5%, n = 15) who had had previous treatment for behaviour problems still had scores in the clinical range at the time of the survey.
Previous attendance at a parenting programme
Just under one fifth of parents (17.8%, n = 141) reported that they had previously attended a parenting programme. Previous attendance was not significantly associated with social class (17.9% non-manual v 19.5% manual), accommodation type (17.3% owner occupiers v 18.5% rented accommodation), or ethnicity (18.5% white v 15.2% non-white). Single parents were more likely to have attended than parents in two parent families (26.2% v 16.2%, p = 0.008), as were parents of children currently defined as having behaviour problems (24.8% v 16.4% of parents with no children with behaviour problems, p = 0.02) or whose children had previously had treatment for behaviour problems (38.1% v 17.2% of parents whose children had never had treatment, p = 0.01).
Interest in attending a parenting programme
A total of 57.8% of parents stated that they would (13.8%) or might (44.0%) be interested in attending a parenting programme in the future. Approximately one fifth of these parents (19.7%, n = 90) had attended a parenting programme before. Interest in attending a parenting group was associated with the eldest child in the family being aged under 4 years, and with the presence of a child in the family who scored in the clinical range on either the intensity or problem scales of the behaviour inventory. Social class, housing tenure, educational level, single parent status, and ethnic group were not significantly associated with the level of interest (table 2⇓).
Interest in attending a parenting group by sociodemographic and child characteristics
Interest in attending was highest in families where the eldest child was between 2 and 3 years and at least one of the children had a behaviour problem (81.3%), and lowest where neither of these conditions applied (47%) (table 3⇓).
Percentage of parents (n) reporting interest in attending parenting group by age of eldest child and whether any child in the family is in the clinical range for behaviour problems
The results of a logistic regression analysis (table 4⇓) showed that the best predictors of interest in attending a parenting programme were the presence of a child with behaviour problems in the clinical range (p < 0.001) and the eldest child being aged 2 or 3 years (p < 0.001). Social class, housing tenure, educational level, and ethnicity were not significant predictors of interest, nor did they affect the predictive power of age and clinical status. Single parent status remained a significant predictor of interest in attending a group after adjustment for other sociodemographic variables.
Variables which predicted interest in attending a parenting group in a logistic regression analysis
DISCUSSION
The results of this study suggest that the proportion of parents who have attended parenting groups or courses may be much higher than suggested by previous estimates (4% in 1994), and that parental interest in future attendance is high. The validity of these results depends on the representativeness of the sample recruited to this study, and the validity of the questions used in the survey.
The survey sample was unrepresentative in that manual class families were under represented and ethnic minority families over represented compared to norms for the City of Oxford and for England. Some of the under representation of manual classes might be an artefact of under reporting of social class by these groups. Oxford is slightly atypical compared to the rest of the UK, with slightly more non-manual residents than predicted from UK norms. It is however less atypical than its reputation suggests. The distribution of behaviour problems was similar to that found in other populations, as was the higher prevalence of behaviour problems in boys.8,10
Oxford may be atypical compared with other parts of the UK in terms of the availability of parenting programmes. For example, since 1997 there has been a charitable organisation in Oxfordshire called the Parenting Forum, with a membership of 120 groups and individuals interested in the development of parenting education. This Forum is supported by the NHS, Social Services, the Youth Service, Adult Education, Family Services, and the Oxfordshire Council for Voluntary Action. It has developed because the level of interest in, and provision of, parenting education in Oxford was such that providers saw the need for coordination and support. Parents who have attended one of the many programmes on offer in Oxford and have found them helpful, as qualitative studies suggest they do,11 are likely to have recommended the programmes to others and generated further interest. Alternatively, the reported attendance rate at parenting programmes may reflect a broader increase in provision and attendance across the country in the years since previous estimates were generated. Further work is needed to establish the generalisability of our findings beyond Oxford, particularly in post-industrial cities in which child mental health problems are most prevalent.
The questions we used in the survey were developed in order to be inclusive. Parenting groups have a variety of names: parent training or education programmes, parenting groups or courses, or the name of the particular curriculum used, for example, Family Caring Trust or Nurturing Programme. All these programmes enable parents to learn positive parenting practices and techniques, including attention, affection, and positive discipline. It is possible that we may have over estimated attendance, but we have not yet identified any groups which fitted the survey question but not our definition of a parenting programme.
Interest in attending is not the same as actual attendance. It is however important. If the majority of parents had said that they would not be interested in attending a group, our conclusions would have been different. This survey was the prelude to a randomised controlled trial of a parenting programme run by health visitors in general practice,12 and 30% of eligible respondents in this survey went on to consent to enter the trial. There was no social class difference in trial volunteers (p = 0.345). Given the pressure on parents’ time, a 30% response to a single invitation to join the study, consisting of several questionnaires and a 50:50 chance of being offered the parenting group, suggests that the level of interest in parenting programmes we have identified in the survey is real. Of those randomised to receive the parenting intervention, approximately 60% attended the majority of the programme.
The results of this survey confirm the findings of other studies13 indicating that behaviour problems of clinical severity affect one in five children. Children from socioeconomically deprived backgrounds were one and a half times as likely to suffer from behaviour problems as children from non-manual backgrounds. However, the results suggest that the use of a “selective” approach directed at manual social class families would miss two fifths of the children with problems. Approximately two thirds of the children who had already received treatment for behaviour problems continued to have problems of clinical severity at the time of the survey, and most of the children with behaviour problems had received no treatment at all. This suggests that the existing provision of “indicated” interventions may be inadequate. The normal distribution of the Eyberg Intensity score suggests that childhood behaviour problems are a public health problem that would benefit from a population approach. These findings provide theoretical support for the universal provision of parenting programmes, and suggest that the optimum age for provision would be when the first child is aged 3 years or less. Indicated provision may be required in addition to universal programmes. Although our survey showed that most parents were interested in attending a programme, other studies identify minority groups of parents who would be unlikely to take part. These might include the most severely disadvantaged and parents most at risk of abuse. Specially tailored provision is likely to be needed for this group, possibly in the form of home visiting programmes. Such selective provision is not incompatible with universal provision and may even be synergistic.
The observation that the level of interest in attending programmes was predicted, not by social class, but by the presence of behaviour problems, suggests that a universal programme would preferentially attract many of the parents most in need. This contrasts with the view that interest in parenting programmes is predominantly a phenomenon of middle class parents who do not have children with behaviour problems.
The development of parenting programmes is not an alternative to changes in social policy which would make the job of parenting easier. Indeed policies to reduce childhood poverty and develop family friendly employment are likely when combined with parenting programmes to have a synergistic effect on public health.
Acknowledgments
The authors would like to thank the participating parents and general practices participating in this survey. Both the project and the Health Services Research Unit were supported by grants from the NHS Executive South East Regional Office. Dr Jane Barlow and Dr Cecilia Pyper are supported by grants from the Department of Health. This work was approved by the Oxford Applied and Qualitative Research Ethics Committee (formerly NAPREC).
Supplementary materials
Need and demand for parenting programmes in general practice
J Patterson, C Mockford, J Barlow, C Pyper, and S Stewart-Brown
Supplemental Material
[View PDF]