Article Text

Abstract
Aims: To compare the clinical efficacy of twice daily oral co-trimoxazole with twice daily oral amoxicillin for treatment of childhood pneumonia.
Methods: Randomised controlled, double blind, multicentre study in outpatient departments of seven hospitals and in one community health service. A total of 1471 children (aged 2–59 months) with non-severe pneumonia were randomly assigned to 25 mg/kg amoxicillin (n = 730) or 4 mg/kg trimethoprim plus 20 mg/kg sulphamethoxazole (co-trimoxazole) (n = 741). Both medicines were given orally twice daily for five days.
Results: Data from 1459 children were analysed: 725 were randomised to amoxicillin and 734 to co-trimoxazole. Treatment failure in the amoxicillin group was 16.1% compared to 18.9% in the co-trimoxazole group. Multivariate analysis showed that treatment failure was more likely in infants who had history of difficult breathing or those who had been ill for more than three days before presentation.
Conclusions: Both amoxicillin and co-trimoxazole were equally effective in non-severe pneumonia. Good follow up of patients is essential to prevent worsening of illness.
- pneumonia
- co-trimoxazole
- amoxicillin
- ARI, acute respiratory infection
- MIC, minimum inhibitory concentration
- OR, odds ratio
- WHO, World Health Organisation
Statistics from Altmetric.com
- ARI, acute respiratory infection
- MIC, minimum inhibitory concentration
- OR, odds ratio
- WHO, World Health Organisation
The World Health Organisation (WHO) estimates that around 3 million deaths occur every year from acute respiratory infections (ARI), mostly in under developed countries.1 WHO has developed a standardised case management strategy to identify and treat pneumonia.2 Specific WHO antimicrobial drug recommendations for treatment of pneumonia are based on data that Streptococcus pneumoniae and Haemophilus influenzae are the most common causes of bacterial pneumonia in developing countries. Based on these findings WHO recommends oral co-trimoxazole and amoxicillin for the treatment of non-severe pneumonia at first level health facilities.3
Pneumonia is a leading cause of childhood death in Pakistan. In 1989, the Pakistan Ministry of Health launched a national ARI control programme. It adopted the WHO recommendation of oral co-trimoxazole as a first line outpatient treatment of non-severe pneumonia, on account of its low cost and twice daily dosage regimen.4
Soon after this, a study conducted in Islamabad/Rawalpindi, Pakistan reported in vitro resistance to co-trimoxazole in 43% of H influenzae and 31% of S pneumoniae blood isolates in children with pneumonia.5,6 Thereafter, from 1990 to 1996 several clinical studies conducted in Pakistan have reported an increasing trend towards clinical treatment failure for non-severe pneumonia with co-trimoxazole.7–10 One study in 1991–92 comparing twice daily co-trimoxazole with thrice daily amoxicillin showed similar clinical efficacy for non-severe pneumonia. The Pakistan ARI Control Programme has explored the possibility of changing from oral co-trimoxazole to amoxicillin for treatment of non-severe pneumonia.
The change from oral co-trimoxazole to amoxicillin has been estimated to cost around $25 million per year in antibiotic costs alone, which is a significant proportion of the national health budget.11 Furthermore, compliance is a major determinant of the success of antibiotic therapy. The choice of dosage for a β lactam antibiotic is based on the proportion of time that serum concentrations exceed the minimum inhibitory concentration (MIC) for the infecting organism.12 Compliance is encouraged when the antibiotic regimen is simple and less frequent, as with co-trimoxazole. Relatively small clinical trials in both children and adults,13–17 have shown that twice daily amoxicillin is equally effective in treating lower respiratory tract infections including pneumonia, compared to the conventional regimen of thrice daily.
In view of the above considerations, the clinical effectiveness of oral co-trimoxazole versus oral amoxicillin twice daily was evaluated in a large group of children with non-severe pneumonia.
PATIENTS AND METHODS
The study was a randomised controlled, double blind, double dummy placebo, multicentre trial, involving eight study sites in six cities of Pakistan (Gilgit, Islamabad, Karachi, Lahore, Multan, Rawalpindi). It was approved by the institutional ethical review boards of the Pakistan Institute of Medical Sciences, Islamabad, Pakistan and the subcommittee on research in human subjects (SCRIHS), WHO, Geneva.
Children aged 2–59 months presenting with cough, difficult breathing, or fast breathing (tachypneoa) were screened. The standard ARI algorithm was used to classify children with pneumonia into the following categories4:
-
Non-severe pneumonia—cough or difficult breathing with fast breathing (respiratory rate ≥50 breaths per minute for children aged 2–11 months; ≥40 breaths per minute for children aged 12–59 months)
-
Severe pneumonia—cough or difficult breathing with lower chest wall indrawing (with or without fast breathing)
-
Very severe pneumonia/disease—cough or difficult breathing with one or more danger signs (convulsions, drowsiness, inability to drink, stridor in calm child, and severe clinical malnutrition).
Children with non-severe pneumonia constituted our study population. A child was excluded if they had severe pneumonia, very severe disease, underlying chronic illness, prior history of two or more episodes of wheeze, acute bronchial asthma, had taken any of the study antibiotics in appropriate doses during the previous 48 hours, or their parents/guardians refused to participate. To ensure follow up at home if needed, only children living within the municipal limits of the urban areas and walking distance in the rural areas were enrolled.
At every site a paediatrician supervised the study and a study physician collected data. Study personnel were trained in standard ARI case management and study methodology at the coordinating centre, Children's Hospital, Islamabad. The site principal investigators carried out regular supervision of the clinical assessment. The study coordinator visited every site for monitoring of clinical and other procedures.
In order to improve the validity of a clinical diagnosis of pneumonia, at every step respiratory rate was counted twice for one minute each within five minutes when the child was quiet, feeding, or asleep. The average of the two readings was taken for assessment purposes. If the average had a decimal value, it was rounded off to the lower digit. If the difference between the two readings was 5 or more, a third reading was obtained. The average was then taken of the two readings with less than five breaths per minute difference. In a child with wheezing, two doses of nebulised salbutamol were given 15 minutes apart and the child was reassessed after 30 minutes for fast breathing. Febrile children were given paracetamol to bring down temperature.
Data were recorded on specially designed autocopy data forms; one copy was sent to the coordinating centre for data entry. Each record had a unique identification number, based on the drug randomisation sequence.
A randomisation scheme was developed for each site using a computer program. A unique number was allocated after eligibility criteria were met and witnessed verbal consent was obtained. The drug assignment was concealed from patients, parents, and study personnel. Children assigned co-trimoxazole received active medicine (4 mg/kg trimethoprim + 20 mg/kg sulphamethoxazole) and amoxicillin placebo twice a day. Children assigned amoxicillin received active medicine (25 mg/kg) and co-trimoxazole placebo twice a day. Oral salbutamol and paracetamol were given when required. Both active and placebo preparations were similar in colour, consistency, and taste. Regular monitoring visits by the national study coordinator from the Children's Hospital, Islamabad were made to all sites during the course of the study.
All enrolled children were regularly reassessed by a study physician three and five days after enrolment. On follow up, in addition to clinical assessment, drug compliance was also determined. Treatment was stopped after five days if the patient was compliant and cured. A child was considered compliant if they had received 80% of the required dose since previous assessment. Poorly compliant children who improved on day 5 were asked to continue with the study medicines for two more days, in order to provide adequate antibiotic for prevention of relapse. Children who did not come for follow up on the specified date were assessed by the study personnel at home. If a patient was “the same” or “worse” on day 3 or day 5, the antibiotic was changed to oral chloramphenicol. Children who developed severe pneumonia, very severe disease, or who did not improve after 48 hours of oral chloramphenicol were referred for inpatient treatment with injectable benzylpenicillin or ampicillin. If injectable therapy could not be instituted, oral cefixime was given for seven days. Children whose treatment was changed were re-evaluated 48–72 hours after change of therapy until cured.
At the follow up visit, “improvement” was defined as slower respiratory rate (either back to normal range for age, or more than 5 lower compared to previous evaluation), better appetite, and less fever. “The same” was defined as still breathing fast (respiratory rate ±5 breaths/minute compared to previous evaluation, or higher than that) and no chest indrawing or danger signs. “Worse” was defined as development of severe pneumonia or very severe disease. “Clinical cure” was defined as return of respiratory rate to age specific normal range at day 5 if compliant or at day 7 if non-compliant. Treatment failures included change of antibiotic therapy, loss to follow up, or death after enrolment.
Statistical analysis
The sample size was calculated to show a difference of treatment outcome among children treated with co-trimoxazole or amoxicillin. We assumed 18% therapy failure among children treated with co-trimoxazole,10 and 12% among those treated with amoxicillin.8 For an α of 0.05 and a β of 0.20, assuming a 20% loss to follow up, the estimated sample size was 1412 from eight sites.
Double data entry was performed and validated using the EPINFO 6.04 software (CDC, Atlanta) at the Children's Hospital, Islamabad. Analysis was carried out on an intention to treat basis using EPINFO 6.04 and SPSS 8.0 software (SPSS Inc., Chicago). Statistical analysis included estimates of odds ratios by univariate analysis. A multivariate model was constructed to look for determinants of treatment failure by forward stepwise logistic regression.
RESULTS
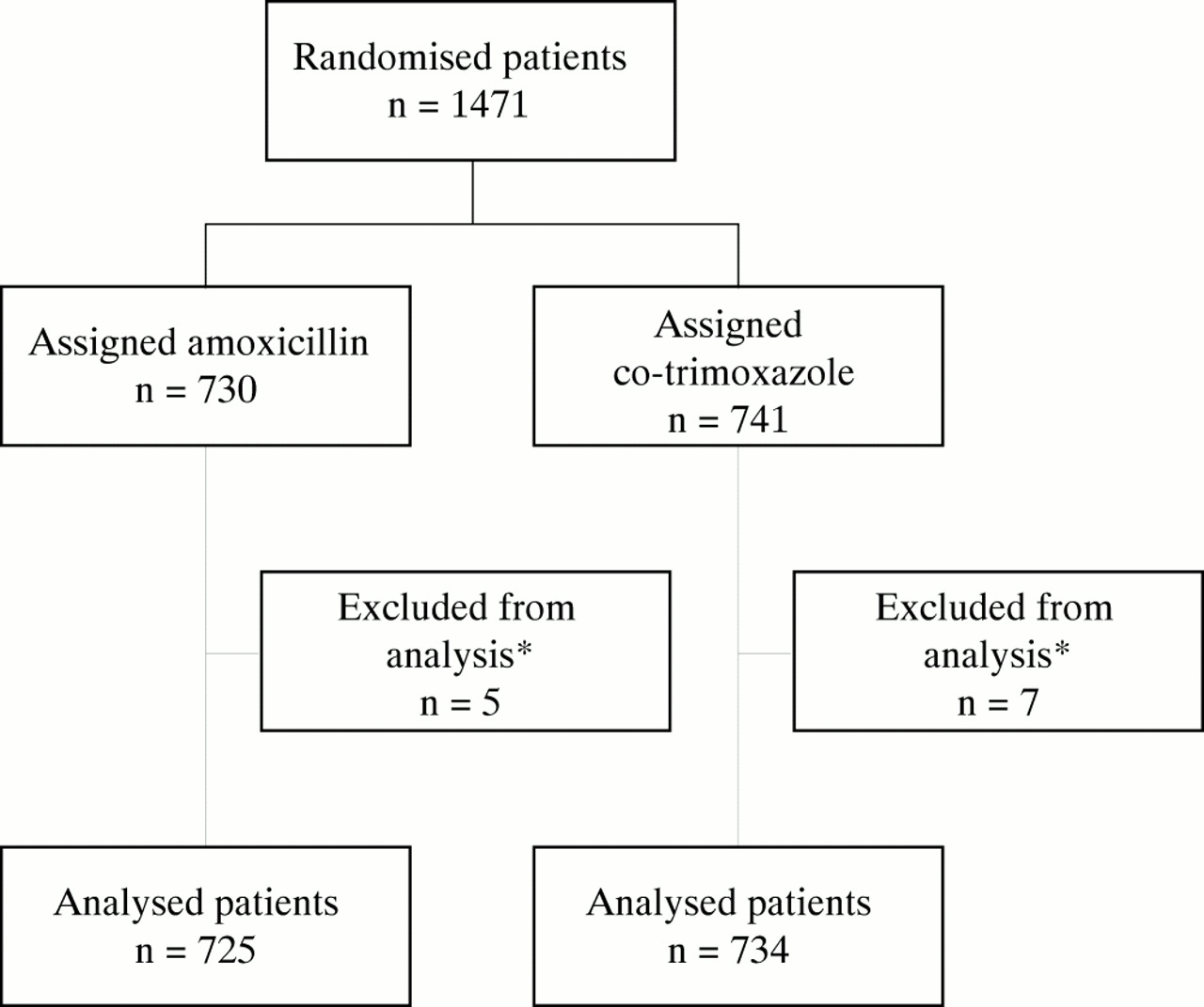
Between January 1998 and October 1999, 1471 children were enrolled. After excluding 12 cases because of protocol violation, 725 received amoxicillin and 734 children received co-trimoxazole (fig 1). The median age was 11 months (range 2–59), with 732 (50%) under 1 year of age. Wheeze was present in 159 children (10.9%) at the time of enrolment. Table 1 presents baseline characteristics of the children.
Baseline characteristics of study patients by treatment groups (n=1459)

Trial profile. *These patients did not fulfil enrolment criteria.
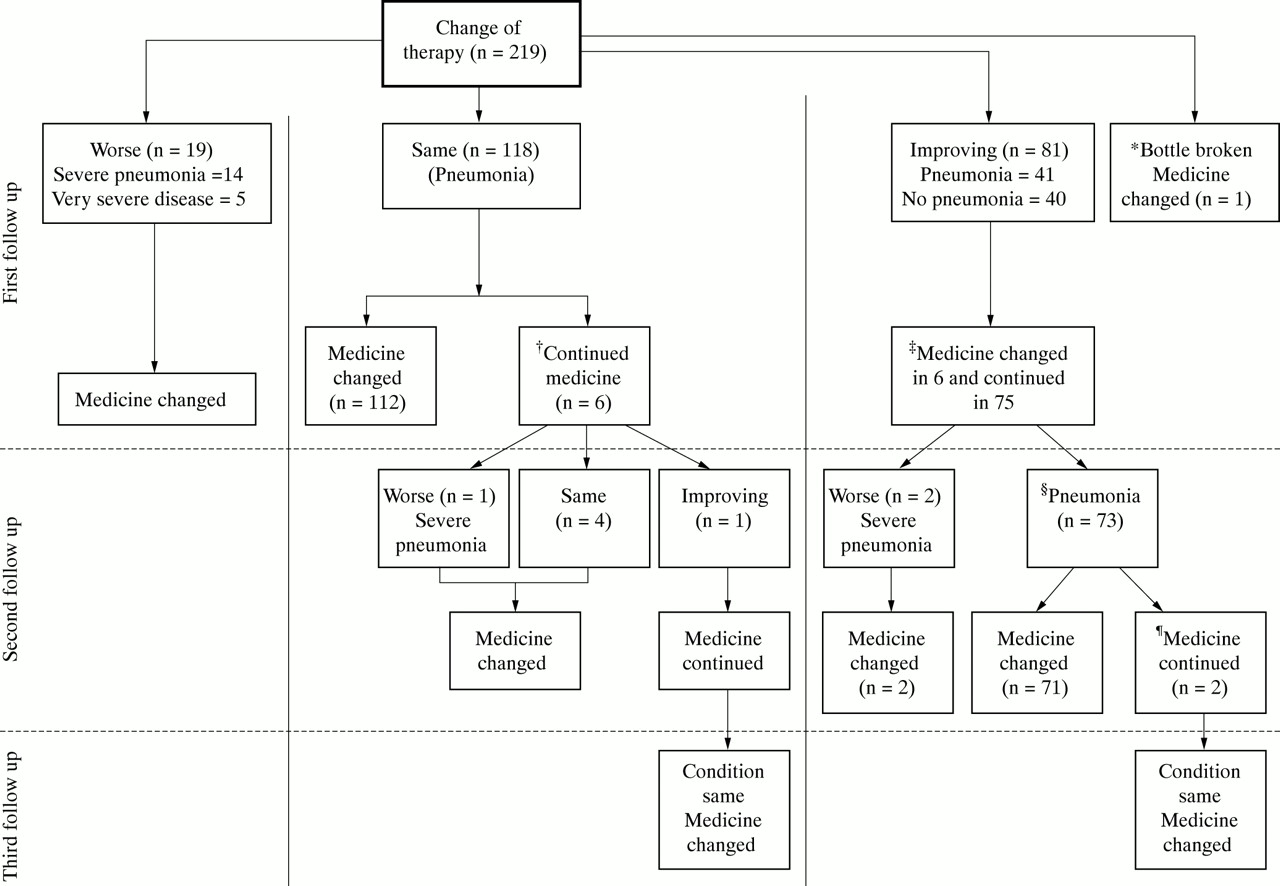
Treatment failure occurred in 256 children (17.5%). Clinical resolution occurred in 608 (83.9%) in the amoxicillin group and 595 (81.1%) in the co-trimoxazole group (OR 0.83, 95% CI: 0.63 to 1.08, p = 0.160). Thirty children were lost to follow up. One child's mother discovered him dead in bed in the morning within 18 hours of enrolment, but the exact cause of his death could not be ascertained (table 2). Of 219 patients requiring change of antibiotic therapy, 146 improved on oral chloramphenicol, 43 on oral cefixime, and 30 needed injectable antibiotics. After the first follow up, 118 remained the same; 19 deteriorated, of whom 14 developed severe pneumonia and five very severe disease (fig 2). In six children who remained the same at the first follow up, antibiotic therapy was not changed; they required a change of therapy on subsequent visits. Of 81 children assessed as improved at the first follow up, 41 who did not have pneumonia developed signs of pneumonia at the second follow up. There was no significant difference between the two therapeutic groups in children who remained the same or improved at the first follow up. Fifteen children deteriorated in the co-trimoxazole group versus six in the amoxicillin group (OR 2.17, 95% CI: 0.75 to 6.56, p = 0.118).
Primary outcome of study patients by co-trimoxazole and amoxicillin
{kind=link}
{kind=link}
Details of patients needing a change in antibiotic therapy (n = 219). *One study bottle was broken and medicine was changed to chloramphenicol; †4 were non-compliant and 2 looked clinically well; ‡3 looked sick clinically, 1 developed rash, and the mothers of 2 were very apprehensive and wanted therapy changed; §6 had improved clinically but respiratory rate was still above age specific cut off value. 5 children also had wheezing; ¶in both the respiratory rate was on borderline age specific cut off value, so treatment was continued.
In the univariate analysis, among baseline characteristics, children less than 1 year of age, with a history of difficult breathing, longer duration of illness, and a high respiratory rate at enrolment were at greater risk of treatment failure (table 3). Antibiotic therapy, weight for age z score, prior use of antibiotics, history of breast feeding, wheeze, and non-compliance to co-trimoxazole (3.4%) or amoxicillin (3.9%) were not significantly associated with therapy failure. In the multivariate model age less than 1 year (OR 1.5, 95% CI: 1.12 to 1.91, p = 0.005), history of difficult breathing (OR 1.61, 95% CI: 1.13 to 2.15 p = 0.006), and duration of illness more than days (OR 1.4, 95% CI: 1.03 to 1.8, p = 0.028) were significantly associated with treatment failure.
Univariate analysis: relation of treatment failure with enrolment variables
DISCUSSION
The results show no significant difference between the clinical efficacy of oral co-trimoxazole and amoxicillin given twice daily for the treatment of non-severe pneumonia in children. However, the clinical failure rate for both co-trimoxazole and amoxicillin was relatively high. When compared with the two previous clinical trials of pneumonia therapy in 2–59 month old children in Pakistan, treatment failure rates of 18.9% with co-trimoxazole are comparable but 16.1% with amoxicillin is higher. In the 1991–92 trial, treatment failure for non-severe pneumonia was 13% with twice daily oral co-trimoxazole and 12% with thrice daily oral amoxicillin.8 In the same trial, younger age and a positive chest radiograph were significantly associated with treatment failure, whereas in the present study, history of difficult breathing, younger age, and longer duration of illness was found significant. In the 1995–96 pneumonia trial of single dose versus double dose co-trimoxazole therapy, the clinical failure rates were 16.6% and 18.1% respectively.10
The increasing treatment failure rate over time for non-severe pneumonia has raised the question of whether we need alternate regimens or antibiotics to meet the challenge of increasing treatment failure rate. Antibiotic recommendations for the current WHO standard ARI case management guidelines3 were based on clinical efficacy of co-trimoxazole and penicillin for the treatment of pneumonia. The WHO guidelines for the treatment of non-severe pneumonia have been shown to be effective in many settings.18
The high treatment failure rate in this study could be caused by one or more of the following factors: (1) increase in antimicrobial resistance of S pneumoniae and H influenzae to both co-trimoxazole and amoxicillin; (2) the aetiology of non-severe pneumonia is non-bacterial in a large proportion of cases; (3) twice daily regimen of amoxicillin is not effective.
(1) Lack of microbiological data from our study makes it difficult for us to correlate the increase in clinical treatment failures with antimicrobial resistance. However, inferences could be drawn from published data. Several studies have failed to show any significant relation between in vitro resistance and clinical outcomes.8,19–21
Normally, if the serum concentrations of an antibiotic exceed the MIC for the infecting bacteria for a reasonable period of time, the disease should be cured. But even using a double dose of co-trimoxazole for the treatment of non-severe pneumonia did not make any difference in clinical outcome.10 In the same study, however, serum concentrations of co-trimoxazole after a double dose were consistently higher and above the MIC values for S pneumoniae and H influenzae for a longer period of time compared to the standard dose (unpublished data, personal communication, S Qazi).
In light of the existing data, the role of increasing antimicrobial resistance in clinical treatment failure for pneumonia remains unclear.
(2) It is possible that some patients with fast breathing enrolled in the study did not have pneumonia, as the sensitivity and specificity of fast breathing (as defined by the WHO to categorise non-severe pneumonia), is around 80%.22 However, distinguishing viral from bacterial pneumonia either clinically or by radiological examination is extremely difficult.23,24 Although enrolment of viral pneumonia cases in our study is possible, mixed viral and bacterial infection are common in children.25–27 We excluded all cases of known bronchial asthma and children who had two or more episodes of wheezing at screening. Nearly 11% of the study patients had wheezing at the time of enrolment. Some clinical treatment failures may have had either bronchiolitis or early hyper-reactive airway disease.
(3) The possibility of high treatment failure rate associated with a twice daily oral amoxicillin regimen seems unlikely. Studies comparing twice and thrice daily amoxicillin regimens in patients with acute lower respiratory infections including pneumonia in children13,15,16 and adults14,17 did not find significant differences in clinical outcome between the two groups. Although not for pneumonia, once daily oral amoxicillin has been used successfully for treating streptococcal pharyngitis.28,29
Despite higher clinical failure rates in this setting in Pakistan, WHO case management guidelines have proved to be very useful. Firstly, two thirds of the clinical failures responded well to oral chloramphenicol, an inexpensive antibiotic. This lends further support to use of chloramphenicol if the first line antibiotic fails. Secondly, WHO recommends counselling and follow up of all cases of pneumonia after two days of antibiotic therapy.30 Under routine care the follow up visits may be infrequent. But 2% loss to follow up in such a large study conducted in the outpatient departments was a major strength. In the present study, counselling at the time of enrolment and on follow up visits, along with visiting patients at home if they did not attend, resulted in good follow up. It is difficult to assess why some children, who were improved at first follow up, had developed fast breathing at the second follow up. The possibility of either a viral infection or an error in assessment cannot be ruled out. It is possible that good follow up in our study did prevent some deaths, which might have resulted from worsening of the initial illness. There is a need to promote and teach good counselling skills and strengthen the health system in order to improve follow up of patients.
Main study limitations were not doing a detailed chest examination using a stethoscope, obtaining chest radiographs, and microbiological cultures in study patients. WHO ARI case management guidelines do not recommend that routinely at a first level facility. Secondly, a longer follow up to identify relapses was not possible because of limited resources. Thirdly, study sites were initially identified to uniformly represent all parts of the country, but for various reasons enrolment rate was very slow in the southern parts of the country and it had to be increased in the northern part of the country. Finally, a third arm with amoxicillin given thrice daily in our study would have strengthened the study considerably.
It is widely believed that oral amoxicillin is more efficacious and safer than oral co-trimoxazole, and some public health professionals are concerned about using co-trimoxazole as a first line antibiotic for the treatment of pneumonia. Their fear is that poor follow up could result in a serious adverse outcome if co-trimoxazole is not successful in treating pneumonia. Co-trimoxazole does not work well for children with severe pneumonia.8 Although no children with severe pneumonia were enrolled in the present study, a higher treatment failure rate for non-severe pneumonia has public health implications where follow up of patients is not possible. Our data do not show that twice daily oral amoxicillin would work significantly better than oral co-trimoxazole for non-severe pneumonia.
Results of our study have identified areas for further research. Firstly, there is a need to collect data on the clinical outcome of non-severe pneumonia data from other developing countries for comparison, especially where antimicrobial resistance rates are not as high as those in Pakistan. Secondly, there is a need to study alternative regimens, such as increasing the dose of oral amoxicillin or the efficacy of the cephalosporin group of antibiotics. Finally, children presenting with wheezing and signs of pneumonia need to be studied in greater detail.
Acknowledgments
We are grateful to Glaxo Wellcome Pakistan and Servipharm (Novartis) Pakistan for the supply of study medicines and their placebos free of charge. The Department of Child and Adolescent Health and Development, World Health Organisation, Geneva provided funding for this study.
REFERENCES
Footnotes
-
Contributorship details for authors follow. All names for study implementation, and data analysis and manuscript preparation appear according to alphabetical order of sites. The first draft of the manuscript was written by Dr Tabish Hazir, and finalised by Dr Shamim Qazi.
-
Protocol development: Dr SA Qazi, Dr Z Rasmussen, Dr A Bari, Dr GN Rehman, Dr Z Kundi.
-
Monitoring of the study: Dr SA Qazi, Dr T Hazir, Dr E Latif.
-
Study implementation: Aga Khan Health Services, Gilgit (*Dr Z Rasmussen); District Headquarters Quarters Hospital, Gilgit (*Dr M Rafi, **Dr M Alam); Children's Hospital, Islamabad (*Dr GN Rehman, **Dr S Ansari); Federal Govt Services Hospital, Islamabad (*Dr A Murtaza, **Dr S Munir); National Institute of Children Health, Karachi (*Dr S Ibrahim, **Dr A Haider); Services Hospital, Lahore (*Dr R Mehmood); Nishtar Hospital, Multan (*Dr I Iqbal); Rawalpindi General Hospital, Rawalpindi (*Dr R Asghar, **Dr S Aslam). *Site coordinator; ** study physician.
-
Data analysis and manuscript preparation: Children's Hospital, Islamabad (Dr T Hazir, Dr GN Rehman, Dr E Latif, Dr S Ansari); Federal Govt Services Hospital, Islamabad (Dr S Munir); Nishtar Hospital, Multan (Dr I Iqbal); Rawalpindi General Hospital, Rawalpindi (Dr R Asghar, Dr S Aslam); WHO, Geneva (Dr SA Qazi); Consultant epidemiologist (Dr A Bari).
Linked Articles
- Atoms