Article Text

Abstract
Background: Procalcitonin (PCT), a precursor of calcitonin, is a recognised marker of bacterial sepsis, and high concentrations correlate with the severity of sepsis. PCT has been proposed as an earlier and better diagnostic marker than C reactive protein (CRP) and white cell count (WCC). This comparison has never been reported in the differentiation of meningococcal disease (MCD) in children presenting with a fever and rash.
Aim: To determine if PCT might be a useful marker of MCD in children presenting with fever and rash.
Methods: PCT, CRP, and WCC were measured on admission in 108 children. Patients were classified into two groups: group I, children with a microbiologically confirmed clinical diagnosis of MCD (n = 64); group II, children with a self limiting illness (n = 44). Median ages were 3.57 (0.07–15.9) versus 1.75 (0.19–14.22) years respectively. Severity of disease in patients with MCD was assessed using the Glasgow Meningococcal Septicaemia Prognostic Score (GMSPS).
Results: PCT and CRP values were significantly higher in group I than in group II (median 38.85 v 0.27 ng/ml and 68.35 v 9.25 mg/l; p < 0.0005), but there was no difference in WCC between groups. Sensitivity, specificity, and positive and negative predictive values were higher for PCT than CRP and WCC. In group I, procalcitonin was significantly higher in those with severe disease (GMSPS ≥8).
Conclusions: PCT is a more sensitive and specific predictor of MCD than CRP and WCC in children presenting with fever and a rash.
- procalcitonin
- meningococcal disease
- white cell count
- C reactive protein
- AUC, area under curve
- CRP, C reactive protein
- GMSPS, Glasgow Meningococcal Septicaemia Prognostic Score
- IL, interleukin
- MCD, meningococcal disease
- PCT, procalcitonin
- ROC, receiver operator characteristic
- TNFα, tumour necrosis factor α
- WCC, white cell count
Statistics from Altmetric.com
- AUC, area under curve
- CRP, C reactive protein
- GMSPS, Glasgow Meningococcal Septicaemia Prognostic Score
- IL, interleukin
- MCD, meningococcal disease
- PCT, procalcitonin
- ROC, receiver operator characteristic
- TNFα, tumour necrosis factor α
- WCC, white cell count
Despite introduction of the new meningococcal C conjugate vaccine, meningococcal disease (MCD) remains an important cause of morbidity and mortality in childhood. There is now good evidence that mortality from this disease is falling,1 but a high index of suspicion, prompt diagnosis, and aggressive management are essential if mortality and morbidity are to be reduced further.
The ill child who presents with fever and a rash will almost always be managed as MCD with intravenous antibiotics, aggressive fluid resuscitation, inotrope support, and ventilation if necessary. In contrast, the relatively well child with fever and a rash may present a diagnostic dilemma for the clinician. Most clinicians would err on the side of caution and admit such children. They might also be started on intravenous antibiotics pending the results of blood culture and polymerase chain reaction assay to detect meningococcal DNA. A significant proportion of such children may have a viral illness,2,3 therefore managing them as cases of meningococcal septicaemia would be subjecting them to unnecessary antibiotics and hospital admission.
Procalcitonin (PCT) is a 116 amino acid protein with a molecular mass of 13 kDa, which is a precursor of calcitonin. In neuroendocrine cells (C cells of the thyroid, pulmonary, and pancreatic tissues), it undergoes successive cleavages to form three molecules: calcitonin (32 amino acids), katacalcin (21 amino acids), and an N-terminal fragment (57 amino acids). Raised concentrations of a substance immunologically identical to PCT in sepsis were first described by Assicot and colleagues,4 and were found to correlate with the severity of microbial invasion.
The exact sites of PCT production are unknown, but the liver is thought to be the major site of production. Human hepatocytes have been shown to produce large amounts of PCT following stimulation with tumour necrosis factor α (TNFα) and interleukin 6 (IL-6).5 In health, circulating concentrations are generally very low, usually below 0.01 ng/ml, and in viral infection and inflammation concentrations are slightly increased, but rarely above 1 ng/ml.6 In contrast, in severe bacterial infection concentrations may reach 500 ng/ml or more. This makes it an ideal marker for differentiating bacterial from viral infection. PCT concentrations start to rise from about four hours after an endotoxin challenge, peak at about six hours, and remain increased for over 24 hours. In contrast, C reactive protein (CRP) concentrations begin to rise between six and 12 hours.7,8
CRP as a single variable was shown to facilitate evaluation of the seriousness of infectious purpura with shock. CRP <100 mg/ml on admission was associated with a high fatality rate.9 In a study of 124 children with MCD, eight had CRP values on admission that were less than 20 mg/l, of which five had symptoms for 12 hours or less.10 In that study, CRP was found to have a role in supporting the diagnosis of MCD, and monitoring the response to treatment, but was not found to be of prognostic value. It concluded that in pyrexial children, where the diagnosis was doubtful, CRP may aid clinical management. A more recent study of 55 children presenting to a paediatric assessment unit with fever and a petechial rash proposed the “ILL” criteria (irritability, lethargy, and low capillary refill), white cell count (WCC) outside the range 5–15 × 109/l, and CRP >5 mg/l as risk factors for significant bacterial sepsis.11
This study aimed to determine whether PCT might be a useful marker of MCD in children presenting with fever and a rash, and to compare this with CRP and WCC. Additionally, we aimed to determine if there was any correlation between PCT and the proinflammatory cytokines TNFα, IL-6, and IL-8.
METHODS
A total of 108 children were studied. Children were included in the study if they were referred to the meningococcal research fellow at the Royal Liverpool Children's Hospital NHS Trust, Alder Hey with a presumptive diagnosis of MCD, from two prospective studies (September 1992 to April 199412 and November 1997 to March 199913). PCT, WCC, and CRP were measured on samples which had been taken on admission and stored at −70°C. Ethical approval for collection and analysis of samples for this study was obtained from the local research ethics committee.
In 64 children (group I), a clinical diagnosis of MCD was made in an ill child with fever and a petechial or purpuric rash (probable cases),14 in all of whom the diagnosis was confirmed microbiologically. These children were all managed as cases of MCD, and were notified to the consultant in communicable disease control. In 44 children (group II), all microbiological tests were negative for MCD, and the supervising clinician made an alternative diagnosis (see table 1). These children were all initially thought to have MCD, not just fever and petechiae.
Diagnoses in children presenting with fever and a rash but without MCD
In children with a clinical diagnosis of MCD, severity of disease was assessed using the Glasgow Meningococcal Septicaemia Prognostic Score (GMSPS).15,16 Severe disease was defined as a GMSPS of ≥8. Concentrations of TNFα, IL-6, and IL-8 were also determined on plasma samples taken on admission. The plasma samples were stored at −70°C until assayed using an enzyme amplified sensitivity immunoassay (Medgenix, Fleurus, Belgium).
Measurement of plasma PCT was performed using a coated tube immunoluminometric assay as supplied by Brahms Diagnostica GmbH, Berlin, which is a “sandwich immunoassay” with one of the monoclonal antibodies being luminescence labelled. Using a luminometer, the intensity of the luminescence signal was measured which was directly proportional to the concentration of PCT present in the sample. The within and between batch precision were less than 10% for PCT control concentrations of 1.3 and 38.5 ng/ml respectively. Functional assay sensitivity was 0.3 ng/ml.
CRP was measured by rate nephelometry using the Beckman image immunochemistry system with reagents supplied by the manufacturer. This routinely used method has sensitivity down to 4 mg/l. The within and between batch precision were less than 5% across a concentration range of 12–45 mg/l.
Statistical analysis was performed using SPSS for Windows, version 9.0, and receiver operator characteristic (ROC) plots were performed using StatsDirect software. Cut off values of 2 ng/ml for PCT and 30 mg/l for CRP were used, as these gave the best sensitivity/specificity values. The data when plotted did not follow a normal distribution, and therefore the Mann–Whitney test was used to compare distributions, and Spearman's correlation coefficient for correlations.
RESULTS
The age range of the children studied was 0.07–15.9 years. There was a significant difference in median age, PCT, and CRP between the two groups, but not in WCC (fig 1, table 2). Figure 2 shows the ROC plot of the relative accuracies of CRP and PCT in differentiating MCD from other illnesses in children presenting with fever and a rash. The areas under the curve (AUC) for CRP and PCT, at the given thresholds, were 0.90 (95% CI 0.83 to 0.97) and 0.96 (95% CI 0.90 to 1.00) respectively. The proportion difference between these AUCs is not statistically different from zero (95% CI −0.012 to 0.14, p = 0.11). Table 3 shows the sensitivity, specificity, and positive and negative predictive values for WCC, CRP, and PCT and both CRP >30 mg/l and PCT >2 ng/ml. Figure 3 shows a scatter plot of PCT versus CRP values within the two groups.
Median (interquartile range) age, PCT, and CRP concentrations in groups I and II
Performance characteristics of WCC, CRP, and PCT
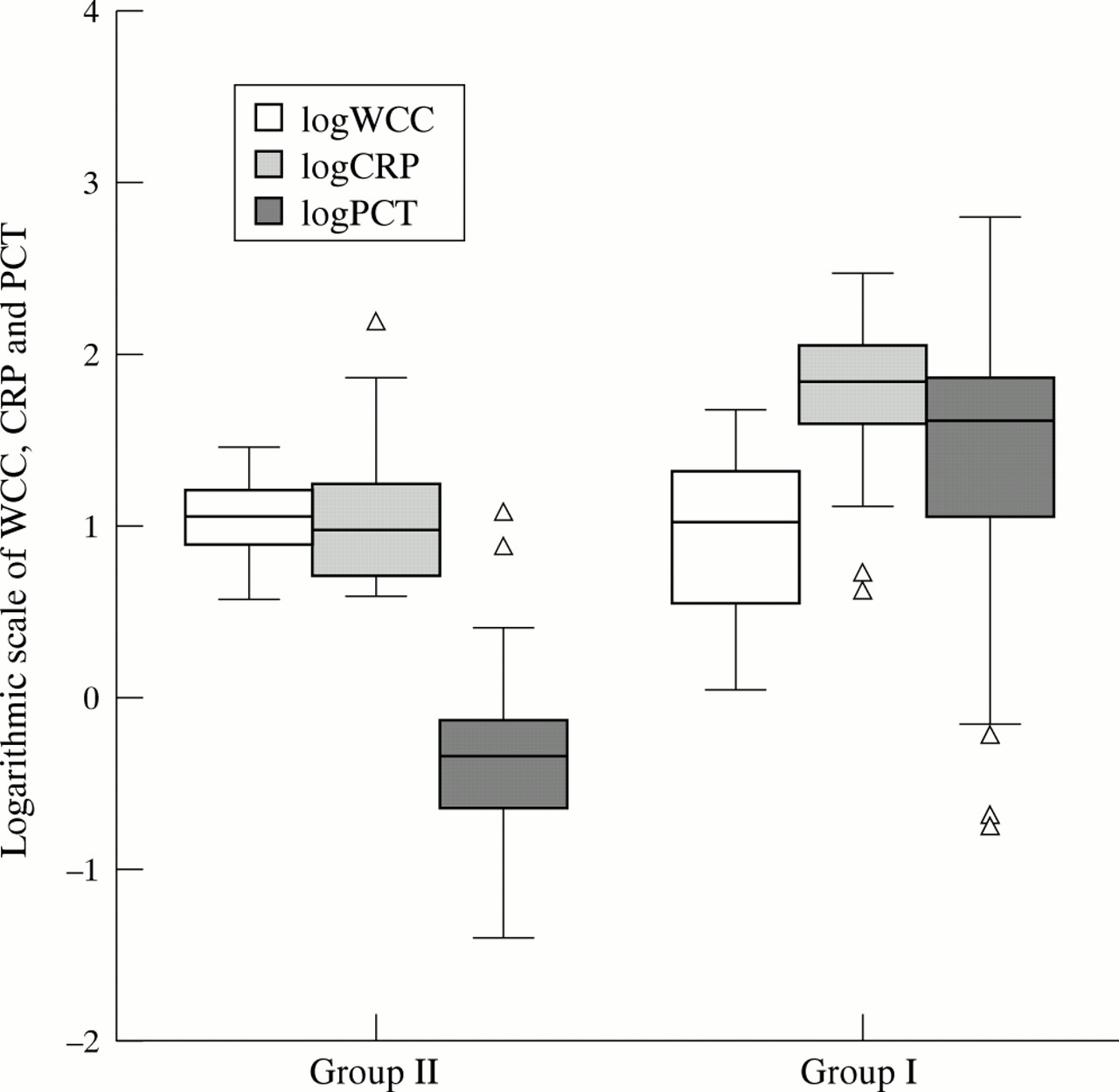
Box and whisker plot showing median, quartiles, and extreme values (log10) for WCC, CRP, and PCT. Box represents the interquartile range, and the whiskers extend from the lowest to the highest values, excluding outliers. Outliers are shown as Δ.

ROC plot comparing CRP and PCT as diagnostic markers of MCD in children presenting with fever and a rash.

{kind=link}
{kind=link}
{kind=link}
Scatter plot of CRP versus PCT values. Axis taken back to −100 to allow better demonstration of spread of points around zero.
There was no significant difference in duration of symptoms between the two groups. There was no significant correlation between PCT and CRP and duration of symptoms. There was a significant negative correlation between admission calcium and PCT (r = −0.597, p < 0.0005), but a positive correlation with CRP (r = 0.393, p = 0.015). There was a significant positive correlation between PCT and TNFα (r = 0.473, p < 0.0005) and IL-8 (r = 0.575, p < 0.0005) but not IL-6 (r = 0.222, p = 0.078). There was a negative correlation between CRP and TNFα (r = −0.415, p = 0.001) and IL-8 (r = −0.314, p = 0.012), but no correlation with IL-6 (r = −0.177, p = 0.163).
In group I, 37 children (57.8%) had severe disease, and five (7.8%) died. PCT was significantly higher in those with severe disease (p = 0.001); it was higher in those who died, but this difference was not significant (p = 0.299).
DISCUSSION
This is the first study to examine the role of PCT as a diagnostic marker of MCD in children presenting with fever and a rash. PCT appears to be a more specific and sensitive marker of MCD than either WCC or CRP.
PCT has been compared with CRP, IL-6, and interferon α in differentiating bacterial from viral infections.17 In that study, a PCT value of ≥1 ng/ml had better sensitivity, specificity, and predictive value than CRP, IL-6, and interferon α. Additionally, PCT values were higher in invasive compared to localised bacterial infections, with a cut off value of 1 ng/ml differentiating between localised and severe bacterial infection.
The role of PCT has also been extensively studied in the intensive care setting; here it is important that an accurate distinction is made between inflammatory states and viral and bacterial infection.18–20 PCT concentrations have been shown to be more sensitive than specific markers of sepsis compared with CRP and IL-6 in adult intensive care patients,20 and than CRP and WCC in critically ill children.19 A cut off of 2 ng/ml was useful in differentiating severe bacterial disease in children. These findings have been confirmed in our study of children initially thought to have MCD, which was subsequently confirmed microbiologically.
The median age of children in the two groups was significantly different. This is because all the children in group I were from the second prospective study period, and the majority of those in group II were from the first study period. There was a significant increase in median age between these two study periods, as a result of the changing epidemiology of MCD on Merseyside, thereby explaining this difference.21
PCT and CRP were significantly higher in children with MCD compared with controls, but WCC was not significantly different. PCT was also higher in those with severe disease compared with those without. There was a significant positive correlation between PCT and the proinflammatory cytokines, whereas with CRP there was a negative correlation. This can be explained by the differential kinetics of PCT and CRP following endotoxin release. PCT rises rapidly and early, shortly following TNFα, IL-6, and IL-8, whereas CRP begins to rise slowly several hours later when TNFα, IL-6, and IL-8 are beginning to fall. The kinetics of CRP also explain the finding of higher CRP concentrations in those with a longer duration of symptoms, which has been reported previously.10
The finding of an inverse correlation between PCT and admission calcium is an interesting one. PCT concentrations are increased in sepsis without an increase in calcitonin.4 Hypocalcaemia is known to occur in septic shock, and has recently been shown to correlate with severity of disease in MCD.22 The exact mechanism for this hypocalcaemia is unclear, as it is not the result of increased urinary excretion of calcium or of attenuated bone resorption. In most septic patients hypocalcaemia was associated with an increased parathyroid hormone concentration, although in a small subgroup with a pronounced inflammatory response, hypocalcaemia was associated with low parathyroid hormone concentrations.23 This finding was also confirmed in a recent study of hypocalcaemia in MCD.22 TNFα has been shown to correlate with the degree of hypocalcaemia and hypomagnesaemia.24 Exactly how the inflammatory response induces hypocalcaemia is unknown, and the question as to whether PCT may have a role to play in this process is one that deserves further study.
One weakness of this study is that children in group II (self limiting illness) did not undergo thorough virological screening (throat swab and stool for virus culture) to exclude aetiologies such as enterovirus. At the time the children were studied, newer techniques such as enterovirus and adenovirus PCR were not available for increased virological confirmation.
The question must be asked whether PCT could be reliably used in the ambulatory or accident and emergency setting to distinguish between children with fever and rash who might have invasive MCD and those without. In 7% of children in this study, a low PCT value would have falsely reassured clinicians, therefore this test cannot be presented as a gold standard. However, it performs better than tests currently used (WCC and CRP), and may be a useful adjunct in diagnosis.
At present widespread use of PCT is prohibited by cost: approximately £6 (sterling) per test (in a research setting), compared to £1 (sterling) for CRP in routine use. It takes three to four hours to perform, but with automation both cost and time to perform the assay should decrease, thereby allowing its more widespread use.
Conclusions
This study has confirmed previous studies that high PCT concentrations are predictive of severe bacterial infection. PCT is a more sensitive and specific marker of bacterial infection than CRP and predicts MCD in children presenting with fever and rash. It correlates significantly with other inflammatory mediators known to be important in the pathophysiology of MCD. In conclusion, PCT is a promising marker of severe bacterial sepsis and is a more sensitive and specific predictor of MCD than CRP and WCC in children presenting with fever and a rash.