Article Text

Abstract
AIMS To determine the effectiveness of a selective hospital based hepatitis B immunisation programme and the barriers to be overcome in obtaining a successful outcome.
METHODS Retrospective case note review of 265 infants born over a five year period to hepatitis B carrier mothers at a university affiliated hospital in Hackney, London.
RESULTS A total of 242 infants (91%) were fully vaccinated; 217 (82%) had serology; 31 required booster doses. Percentages failing to reach second, third vaccinations, and serology on schedule rose exponentially (7%, 18%, 33% respectively). Mobility was high (25%) and significantly affected outcome. A total of 95% Hackney resident babies were fully vaccinated compared with 78% non-residents. Uptake of routine immunisations was higher in Hackney residents than non-residents and greater in those who were eligible for hepatitis B vaccine. Name changes occurred in 35%. Translation requirements were high (85% for Turkish, Vietnamese, and Asian families). Requirements for specific postnatal counselling of mothers and hepatology referral fell significantly during the course of the study. Only seven of 22 babies born in 1995 in Tower Hamlets compared with 53 of 58 Hackney babies received a full vaccination course in non-hospital based primary care.
CONCLUSION In inner city areas with high prevalence of hepatitis B carriage, mobility, and diverse ethnicity, a dedicated centralised immunisation service can be highly effective, provided that adequate support services (translation, counselling, and parental referral) are available.
Key messages
Key messages
Even in inner city areas over 90% of infants can receive full hepatitis B immunisation
Mobility (changes of address) and poor understanding impede uptake
Effective antenatal screening and counselling, availability of translation, and hepatology referral services may all improve uptake
Despite problems of accessibility and cost, a centralised service is technically efficient at immunising babies against hepatitis B in inner city areas with high prevalence rates
- hepatitis B
- immunisation
- inner city
- barriers to immunisation
Statistics from Altmetric.com
In the UK selective immunisation of all babies born to infected mothers is the recommended method of preventing vertical transmission of hepatitis B and the concomitant risk of chronic liver disease.1 ,2 The NHS Executive required health authorities to implement universal antenatal screening and appropriate immunisation of all babies born to infected mothers by April 2000.3 The Executive neither stipulated where or by whom the immunisation programmes were to be delivered nor what levels of uptake should be achieved. Published data suggest that levels of uptake in UK community and primary care based hepatitis B immunisation programmes4 ,5 are generally lower than in centrally organised programmes in the Netherlands.6 In the UK many hepatitis B carriers live in inner cities where uptake of routine immunisations, for example, DPT (diphtheria, pertussis, and tetanus) and MMR (measles, mumps, and rubella) tends to be poor.7 ,8
Both Hackney and Tower Hamlets are inner city areas which form part of the East London and City Health Authority (ELCHA). They have broadly similar demographic characteristics and similar high indices of social deprivation. The London Borough of Hackney has a total population of 200 000 and an under 14 population of 48 000. In 1992–93 babies born to ethnic minorities comprised 48% of live births; 31% were black African or Caribbean.
A hospital based hepatitis B immunisation programme was established in Hackney in 1991 following the introduction of universal antenatal screening. Here we evaluate the effectiveness of this programme over a five year period and analyse the barriers to be overcome in achieving a successful outcome.
Materials and methods
Hepatitis B infected mothers were identified at booking by universal antenatal screening at the Homerton Hospital, Hackney, London. All positive women were counselled as to their status, its implication for themselves, their partners, and their families, and the need for immunisation of the baby. One of us (VL) reviewed details of their status from the virology department and was responsible for coordinating the immunisation programme, including development of an in house vaccination protocol and the training of labour ward staff in its use.
Infants of hepatitis B surface antigen (HbsAg) positive, hepatitis B antibody positive mothers (low risk carriers) were scheduled to receive recombinant vaccine (10 μg) at birth, 1, and 6 months. Infants born to high risk mothers (hepatitis B e antigen positive, or HbsAg positive and hepatitis B e antibody negative, or acute hepatitis in pregnancy) received in addition 200 IU of hepatitis B specific immunoglobulin at birth. Serological responses to vaccination were tested at one year to establish the effectiveness of the immune response. Those having anti-HBs titres greater than 100 IU/l were regarded as immune, those with titres of 10–100 were recalled for a booster dose and retesting six weeks later, and those with titres less than 10 had a repeat course of vaccine.
In order to facilitate attendance, the immunisation clinic was held in the hospital at the same time as the neonatal follow up clinic, with nursing and reception staff from the special care baby unit (SCBU). Weekly clinics were held, but an opportunistic policy for vaccine administration was followed for late comers and those who inadvertently attended the SCBU.
A vigorous policy for tracing non-attenders was followed. All babies who failed to attend one of their vaccinations were notified to their general practitioner, health visitor, and community paediatrician and given the next available appointment. If they failed to attend a second time, hospital based liaison health visitors contacted the family's health visitor and attempted to contact the family themselves to reinforce the need for attendance.
Data from babies born during 1992–96 inclusive were recorded. These included maternal ethnicity, timing of vaccine administration, serology outcomes, and failures to attend.
As part of an attempt to evaluate the effectiveness of the programme in overcoming barriers to immunisation, the following additional data were recorded.
In 1992–93, need for translation facilities, postnatal education/counselling of families, and hepatology referral were documented.
In 1995 we evaluated the mobility of the population by recording changes of names and addresses. Details of changes of name and address were obtained from personal health records and cross checked with the regional interactive child health computer system (RICHS). We compared the uptake of routine immunisation given at 6 months (third DPT) and 1 year (MMR). We also recorded the need for postnatal counselling and hepatology referral as a comparison with 1992–93 to provide some measure of the effectiveness of an antenatal counselling service.
Comparative data for hepatitis B vaccine uptake were obtained for 1995 from a neighbouring London district (Tower Hamlets) where there is a primary care based vaccination programme, but where the number of babies born to hepatitis B carriers is less than in Hackney.
Results
ETHNICITY
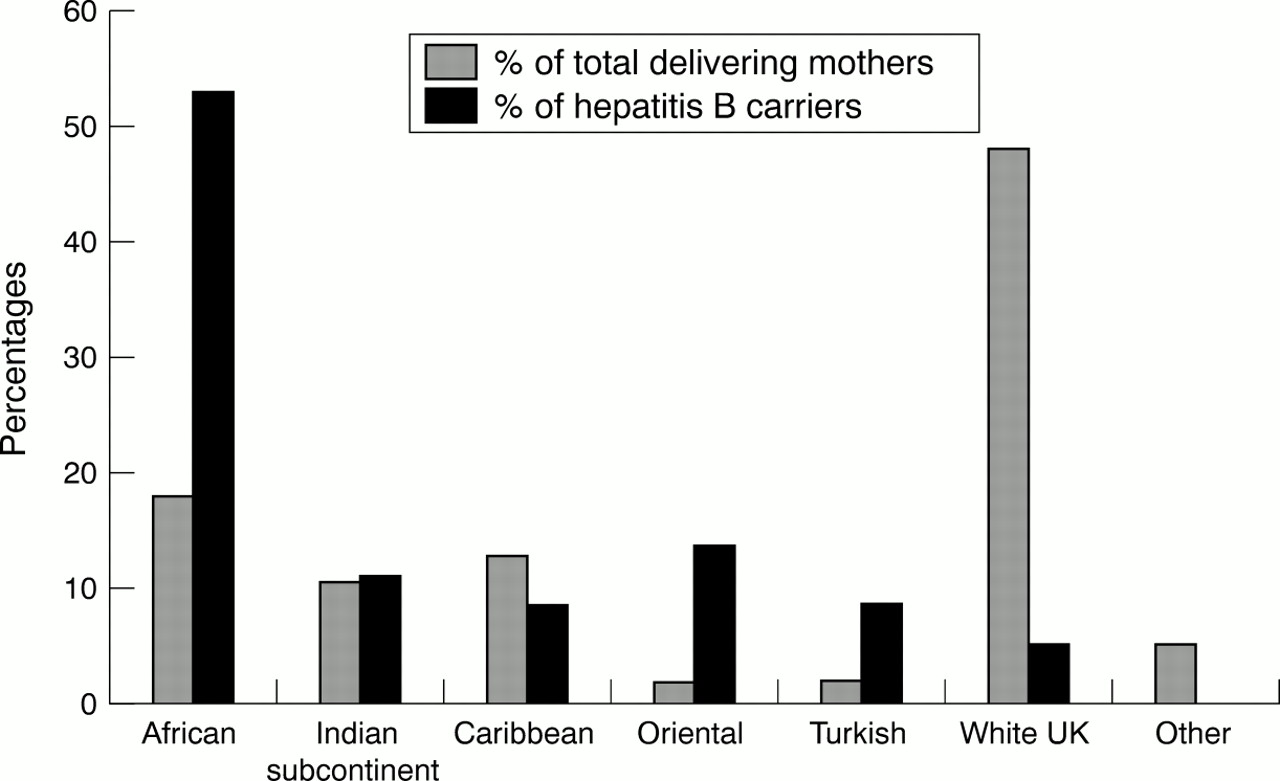
Figure 1 shows the ethnic distribution of hepatitis B carrier mothers in comparison with the ethnic distribution of the total population of delivering mothers. Hepatitis B carriers are seen to be over represented in all ethnic groups studied compared with white mothers, this effect being most notable in African, Oriental, and Turkish groups.

{kind=link}
Ethnicity of mothers.
VACCINE UPTAKE
During the study period there were 18 046 live births at the Homerton Hospital: 265 infants (1.45%) were born to HBsAg positive mothers of whom 46 (17%) were identified as high risk. Of the eligible infants, 242 (91%) received three doses of vaccine and 217 (82%) had serological responses measured. Three patients required revaccination, of whom two responded fully. Booster doses were required for 31 infants; 18 attended for post booster serology and all had satisfactory serological responses.
Two children born to high risk mothers became HBsAg positive. One had received no vaccine whatever; the mother had delivered elsewhere and had not disclosed her hepatitis status. The other child failed to complete her course of vaccine but was subsequently tested and identified as HBsAg positive at another hospital.
BABIES LOST TO FOLLOW UP
Twenty three (9%) infants were lost to follow up and presumed to have failed to complete a full course of vaccine. One had no vaccine (see above), seven had only one dose, and 15 two doses. A significant number of those lost to follow up lived outside Hackney (n = 14, χ2 = 17.4, p < 0.001). A significant proportion of babies were African (n = 18, χ2 = 6.6, p < 0.02); 12 were living in Africa and three outside London, but in the UK.
ADHERENCE TO IMMUNISATION SCHEDULES
Details of the time of administration of the first vaccine dose were available for 184 infants; 180 (98%) received this within 48 hours of birth and 164 within 24 hours. Only four infants had their first dose after seven days, of whom two subsequently tested negative for hepatitis B markers and were successfully immunised. Delays in attending for the 1 and 6 month doses of vaccine were cumulative, occurring in 16 and 40 respectively of the 217 infants whose serological responses were tested. Late attendance had no effect on serological responses. Testing serology was delayed in 72 infants (33%).
EFFECT OF RESIDENCE ON VACCINE UPTAKE
A high percentage of infants (66 of 265, 25%) moved out of Hackney. Of those who remained, a significantly higher proportion (190 of 199) received three doses of vaccine compared with non-residents (52 of 66). (χ2 = 17.41, p < 0.001). A similar trend was observed for serological responses. Data for non-residents were obtained from those who continued to attend for hepatitis vaccination or via health service records and RICHS.
ATTENDANCE FOR ROUTINE IMMUNISATION IN 1995
The uptake of routine immunisation (DPT × 3 and MMR) in those eligible for hepatitis B vaccine was compared with that in the non-eligible, in both Hackney residents (table 1) and non-residents (table 2). Uptake of routine immunisation was high in the hepatitis B vaccine eligible group of Hackney residents (table 1), but low in the non-resident babies. The hepatitis B eligible babies had a higher proportion of recorded mobility than others.
Hepatitis B immunisation versus routine immunisation in Hackney resident babies, 1995
Hepatitis B immunisation versus routine immunisation in non-Hackney resident babies, 1995
OTHER POTENTIAL BARRIERS TO HEPATITIS B IMMUNISATION
Name changes
Babies were initially registered in their mother's surname or second name. In 1995, 35% of infants were recorded as having name changes in the first year of life. The predominant populations affected were West African, Oriental, and Bengali babies; there were too few babies born to white hepatitis B carrying mothers to make meaningful comparisons.
Failure to understand the importance of vaccination
Requirement for translation
In 1992–93 translators or health advocacy services were required for 23 of 27 (85%) families of Indian, Bengali, Turkish, or Vietnamese origin. Overall almost 30% of hepatitis B carrying mothers required translation services.
Requirements for postnatal counselling/referral to hepatology—Comparison was made for the need for postnatal counselling and hepatology referral between the two periods of 1992–93 and 1995. The numbers of patients requiring postnatal counselling and hepatology referral fell significantly (see table3).
Requirement for postnatal maternal counselling and hepatology referral
COMPARISON WITH A NEIGHBOURING INNER CITY AREA—1995
A total of 53 of 58 (91%) Hackney infants compared with seven of 22 (32%) Tower Hamlets infants completed their course of vaccines (χ2 = 27, p < 0.01). None were lost to follow up, although one was living abroad. In contrast, nine of 22 (41%) Tower Hamlets infants had been lost to follow up.
COSTS
We have calculated the total cost (1999 information) of the immunisation programme including vaccines, staff (medical, nursing, secretarial), follow up serology, postage, etc to be circa £32 000. This represents a cost of immunisation of approximately £138 per successfully immunised baby and £126 if all babies are taken into account. Staff costs were 59% of the total cost.
These figures must be set against the long term cost of managing hepatitis B carriers produced by failure of immunisation.
Discussion
The effective delivery of a selective immunisation programme for babies depends on the accurate identification of all high risk pregnancies by universal screening. Efficient, timely communication of positive results, including mothers' e antigen/antibody status is essential. Those responsible for coordinating the programme and those who will administer the first dose of vaccine must be informed. Counselling of mothers is likely to improve their engagement in the immunisation programme. In our cases this was achieved by one of us receiving virology reports, and checking that labour ward staff were conversant with the vaccination policy. Active checking of maternal status was important because both late bookings and delivery elsewhere (acknowledged problems in inner city areas9) are potential obstacles to engagement in an immunisation programme. A high proportion of our infants received their first dose of vaccine with or without immunoglobulins within 48 hours.
Although delivery of the first dose of vaccine is important in minimising risk of vertical transmission, effective protection of the infant depends on the completion of a course of vaccine. The percentage of infants receiving a full course of vaccine consistently exceeded 90%, with over 80% having serological confirmation of their responses.
These coverage figures exceed those previously published for pre-1998 vaccination schedules in the UK, where 21–67% of babies from Manchester and the Midlands respectively were documented as having received three doses of vaccine.4 ,5 In an earlier study for the Public Health Laboratory, 89 of 102 babies from an original cohort of 155 received three doses of vaccine.7 In the Netherlands, where there is a centrally organised service with different vaccination schedules, uptake of three doses of vaccine rose from 80% to 94% between 1989 and 1991.6 Although an increasing number of our babies failed to receive their second or third doses on schedule, this did not seem to be a barrier to effective immunisation as judged by final outcome. Overall the percentage who did receive vaccine on schedule was higher than those in other series.4 ,6 Nonetheless 9% were lost to follow up before completing their course and some of these have probably become hepatitis B carriers.
This coverage was achieved in an inner city area where routine immunisation uptake, for example, DPT and MMR is traditionally poor7 ,8; uptake of third DPT was 91% and MMR 85% in Hackney in 1995. In contrast to other studies, uptake of hepatitis B immunisation was greater overall than that of routine immunisations.4 ,6 Uptake of DPT 3 and MMR were both higher in Hackney resident babies eligible for hepatitis B than those who were not, suggesting that mothers of these babies may have had an increased awareness of the overall value of immunisation. In non-residents uptake of hepatitis B was much higher than that of routine immunisations. One possible explanation of the latter is that the organisation and delivery of the hepatitis B immunisation programme overcame the barriers to effective immunisation, which exist in inner cities.7 These include a high prevalence of ethnic minority families, one parent families, young mothers, and mobility.
Ethnic minority families were disproportionately represented in this study, emphasing the relatively high prevalence of hepatitis B carriage.10 The main barrier to immunisation in ethnic minority families is said to be poor understanding of English.7 Immunisation requires valid consent,2 which must be adequately informed. Adequate understanding of information may be impossible without translation facilities, which were required by approximately 30% of all our families. Even if parental command of English is good, difficulties in comprehending the nature and significance of maternal hepatitis B carriage and its consequences for families may still prevent effective immunisation. This may be countered by pretest discussion and post-test counselling and referral of parents and families to hepatology services.3 The increasing effectiveness of antenatal counselling is one explanation for the decline for the need for postnatal counselling and hepatology referrals between 1992–93 and 1995 in the absence of a significant proportion of hepatitis B carriers having second or subsequent children in 1995.
Although a significant proportion of our babies were born to young, single mothers, this did not seem of itself to be a barrier to immunisation. Of greater practical difficulty in contacting non-attenders were name changes. We attempted to overcome this by amending the parent held records, cross checking with hospital and other records, liaising with family health visitors and clarifying the infants' name(s) via translators. We also encouraged parents to take responsibility for their own child's immunisation programme by active education, support, and demonstration of the importance of the parent held records.
The mobility of families is a further barrier to immunisation. Hepatitis B carriers were disproportionately more mobile when compared with other Hackney families. Changes of address did have an adverse effect on uptake in that a significant proportion of those lost to follow up lived out of borough and many lived abroad. Nevertheless we did achieve a high coverage in non-residents, which may have been an effect of enhanced parental understanding of the importance of completing a course of vaccine.
Hospital based immunisation services may have potential disadvantages in that they are of limited availability and accessibility. We overcame this by offering an open door opportunistic vaccination policy for those who did not attend clinic at specified times, using centralised and parent held records to register such vaccinations. A further means of overcoming such barriers is the use of community or primary care based services which would also have advantages in terms of costs. However, acknowledged difficulties exist in meeting targets for routine immunisation in inner city areas.7 ,8 ,11 Experience with hepatitis B immunisation in our neighbouring district and elsewhere suggests that compliance is still sub-optimal.12 The reason for this may be difficulties in central coordination of such a service, especially in areas where the prevalence of hepatitis B is low. Further, some ethnic minority families may have greater familiarity with or preference for a hospital based mode of delivery of health care.
Hospital based services are likely to be more expensive than those which are community based and our costs were relatively high. They do have to be set against the medical and social costs of poor coverage, which include those of chronic hepatitis B carriage and chronic liver disease. Assuming a similar coverage rate to our neighbouring health district in the absence of a hospital based service, we might expect our 265 infants to have produced approximately 50 new hepatitis B carriers, of whom 25% would develop chronic liver disease.
These results do not indicate where infants should attend for their hepatitis B immunisation. Rather they suggest that barriers to immunisation in an inner city area may be overcome by the provision of a centralised, dedicated service, which has definable features. These include antenatal pretest discussion, post-test counselling, and hepatology referral; effective communication between virology departments, central coordinators, and those responsible for an initial immunisation; tenacity and persistence in tracing defaulters; skilled translation services; and referral of other family members for testing, counselling, and treatment. Our model meets the requirements of the NHS Executive's recommendations.3
References
Commentary
The UK is one of the few western European countries which have chosen not to comply with the WHO recommendations for universal hepatitis B vaccination. The WHO recommended that countries such as the UK, with a low prevalence of carriage, should introduce universal adolescent and/or infant vaccination by 1997.1-1 The UK position therefore needs defending.
Most recognised new hepatitis B infections in the UK occur in young adults1-2; very few infections are acquired in childhood. If we estimate the number of UK infections that lead to chronic carriage, however, adult exposures are the major cause but perinatal infections form a substantial minority.1-2 The most immediate priorities for prevention, therefore, are to target those at greatest risk by improving uptake in those exposed by sexual activity or intravenous drug use, and in infants born to carrier mothers.1-3
Universal adolescent vaccination has potential to impact on adult infections in the medium term, but would have limited impact on perinatal infection as most pregnant carriers will have been infected during childhood in countries of high prevalence.1-4 If universal infant vaccination was adopted, for example using combination infant vaccines, it would take many years to have an impact on the peak incidence in young adults and, unless an additional dose of hepatitis B vaccine was given at birth, would not prevent perinatal infections. Even with a universal adolescent or infant vaccination policy, therefore, it is still necessary to identify babies born to carrier mothers so that they can be given the additional protection of vaccine at birth and, if the mother is high risk (HBeAg positive and anti-HBe negative), hepatitis B immunoglobulin.1-5 Universal antenatal screening, as recommended since April 2000, is essential so that the risk status of all babies is known by the date of delivery.1-6
One argument for switching to universal vaccination in infancy is that it would be easier to achieve high vaccine coverage in infants at highest risk. This argument was based on a number of audits which suggested that coverage for selective hepatitis B vaccination was low.1-7-1-9 Larcher et al show that achieving high hepatitis B vaccination coverage is possible—even in an inner city district with a highly mobile and ethnically diverse population. This and studies from overseas have shown that success depends on having a well focused, and actively managed programme with intensive attention to follow up.1-10-1-12
The prevalence of carriage in the UK antenatal population is very low—probably between 0.1% and 0.3%.1-4 1-13 1-14 As there are about 640 000 births per year in England and Wales, we estimate that around 2000 babies born each year are at risk of perinatal infection. As neonatal vaccination is 90% effective at preventing a risk of up to 25% that the child will become a hepatitis B carrier, only four children need to be vaccinated to prevent one carrier. We argue that resources should be targeted at selective infant vaccination and improving follow up of these 2000 infants at greatest risk (including testing for HBsAg). This is likely to have a more rapid impact on perinatal infections and subsequent population HBsAg carriage than vaccination of 638 000 infants who are at no risk at birth and at very low risk during childhood. To justify the UK policy of universal antenatal screening and selective vaccination, however, requires surveillance systems to be in place. Paediatricians have an important role in ensuring that the UK can show that implementation of selective infant vaccination is effective.
Commentary
Larcher et al show that, in certain instances, a selective approach to hepatitis B virus (HBV) vaccination can work. Accordingly, the UK Department of Health's recent instruction2-1 that all pregnant women should be offered and recommended a hepatitis B test is welcome; this new guidance stemmed from the recognition that large proportions of certain high risk groups were not being vaccinated despite long standing directives which indicated that they should be.
The World Health Organisation, in an attempt to eradicate HBV globally, asked all governments to implement universal HBV vaccination of children in their countries by 1997.2-2 The nearly 100 countries in which all children are now immunised against HBV includes most of Europe and North America.2-3 In the UK, however, a compelling case for the introduction of universal vaccination has been hindered by the equivocality of the results of cost effectiveness analyses2-4 2-5; these incorporated relatively scanty data on HbsAg carriage rates which are lower than those observed in countries which have adopted universal immunisation. Accordingly, the universal approach is still being resisted in favour of a targeted intervention. This “evidence based” stance would be applauded if it were not for the following factors.
In the context of a targeted programme, the vaccination of all those belonging to certain high risk groups, in particular injecting drug users, is problematic. Although the guidance to immunise injectors was launched in 1988,2-5 rates of vaccine uptake among this group are either unknown or low.2-6 In Glasgow, a city with the highest prevalence of injecting in the UK and an extensive network of harm reduction agencies, community wide surveys of injectors who had been injecting for, on average, six years, were conducted in 1993/94 and 1999; 81% (833/1024) and 79% (351/444), respectively, had never received a single dose of HBV vaccine (unpublished data, SCIEH). Occasional islands of high uptake have been observed in England,2-7 and the Department of Health has recently pumped considerable resources into improving vaccination rates.2-8Optimal rates can only be achieved if dedicated funding for vaccination is sufficient and sustained, and if drug treatment/needle and syringe exchange centres are numerous, accessible, and user friendly enough to attract high proportions of injecting populations.2-7 Even if favourable conditions existed throughout the UK, it would not be possible to offer vaccine to those who had recently commenced their injecting careers and had not yet gravitated to such agencies. Past and present experience informs us that vaccinating, for example, over 80% of UK injectors who had started to inject in the previous two years is unachievable.
In the late 1990s the incidence of acute HBV infection among injecting drug users, UK wide, increased dramatically.2-9 2-10 This observation highlights the pitfall of using HBV data that apply to current and past (injecting) behaviours to make a decision about the implementation of universal vaccination, the impact of which—in terms of the number of hepatitis B infections prevented—depends entirely on the future behaviour of the population; if, for example, the universal vaccination of UK adolescents had been implemented in 1990, a large proportion of the UK's recent HBV infections would have been avoided.
Perhaps the most unconvincing aspect of the current selective policy is that it is not particularly selective. To not merit vaccination one has to eschew—throughout one's lifetime—injecting drug use, having multiple sexual partners, being imprisoned, working in occupations in which one might come into contact with “sharps”, and spending lengthy periods in parts of the world where infection is endemic.2-11 Since millions of persons already qualify for vaccination, the case for continuing with a selective policy appears untenable.
If the above reasons for abandoning the present policy and embracing universal immunisation were still considered insufficient, the premise that the fight to rid this infection globally can only be won if every country, regardless of its current prevalence, is signed up to vaccinate its entire childhood population, should be decisive.