Article Text

Abstract
AIMS To determine whether tuberculosis is increasing in frequency and to explore the association between deprivation, ethnicity, and tuberculosis in the city of Leeds.
METHODS Descriptive epidemiology and ecological analysis of a register of children and young people (0–18 years) diagnosed with tuberculosis from 1982 to 1997 in Leeds Health Authority.
RESULTS A total of 107 children were identified, 61 through contact tracing, to give an age and sex standardised incidence rate of 3.9 per 100 000 per year. Rates decreased over the 16 year study period by an estimated 6.6% per year. The disease was more common in girls (56%) and most frequent in 5–9 year olds, with respiratory disease accounting for the largest proportion (82%). Children of south Asian origin (35%) had a crude incidence rate of 25.7 per 100 000 per year. The female:male ratios differed notably between south Asian (1.9:1) and non-south Asian children (1.02:1). For all subjects, univariate analyses showed significant positive associations between incidence and deprivation, population density, and ethnicity. There were no significant associations between deprivation, population density, and ethnicity and incidence of tuberculosis in south Asian children. For non-south Asian, mainly white children, only deprivation was significant. The proportion of non-south Asian children in the population was the overriding factor influencing incidence of tuberculosis.
CONCLUSIONS Tuberculosis remains an uncommon disease in Leeds children. An unexpected finding was a relatively higher incidence in Asian girls compared to boys. Overall, ethnicity explains a high proportion of disease independently of deprivation and population density but for non-south Asian Leeds children the strongest risk factor is deprivation.
- tuberculosis
- ethnicity
- deprivation
Statistics from Altmetric.com
Tuberculosis in children has been considered to be a disappearing disease.1 In England and Wales the notification rate of tuberculosis has declined steadily from 1913 to 1987.2 The 1983 survey of tuberculosis notifications in England and Wales showed a 35% decline over five years.3On the assumption that this trend would continue, the Joint Committee on Vaccination and Immunisation recommended stopping the school BCG programme by 1990 provided that the next survey showed a continuing downward trend.4 Unfortunately the national figures have shown no further decrease in notification rates.5
Tuberculosis has always been associated with poor living conditions and there is a recognised association between tuberculosis and poverty.6 ,7 Consistent patterns have emerged in national3 ,5 ,8 studies of tuberculosis showing higher rates in those from minority ethnic populations.9 For example, rates of tuberculosis of children of Bangladeshi origin are 25 times higher than those in the white population.5
The 1991 census showed Leeds to be the second largest metropolitan district in the UK, covering an area of 217 square miles with a total population of 720 000. The area is divided into 33 electoral wards; the 12 most deprived wards constitute an inner city area with a total population of 235 000. This densely populated part of the city contains 60% of those claiming supplementary benefit, 60% of the unemployed, 75% of the minority ethnic populations, 50% of single parent families, but only 28% of the population.10
The city has the benefit of a central chest clinic with carefully maintained records of all cases of tuberculosis. An earlier retrospective study6 had used relatively crude measures of poverty (residence within a defined “urban priority area”). The present study used more appropriate epidemiological methods over a 16 year period.
Methods
Cases were ascertained using the tuberculosis notification register at Leeds Chest Clinic, clinical records for those treated at the chest clinic, and cross checked with the health visitors' register held at the clinic. Children included in the study were aged 0–18 years, and diagnosed by a specialist physician at the chest clinic as having tuberculosis; their names were included on the tuberculosis register for the study period 1982–1997. Clinical assessment, tuberculin sensitivity, sputum microscopy and culture (when possible), and radiological assessment were used and the diagnosis made on the basis of all available information. Children were excluded if they were receiving antituberculous chemoprophylaxis, were infected with atypical mycobacteria, or when the diagnosis was changed by a chest physician on review. A standard proforma was used to abstract data from hospital case notes including full name, full address, and demographic details. Postcodes were validated using QuickAddress11; they were assigned to a 1991 census electoral ward via the Central Postcode Directory using the PC2ED facility at Manchester Information and Associated Services.
Each individual child was initially classified as being south Asian or not, using the Asian name analysis software Nam Pehchan.12This was cross checked, where possible, with specialist tuberculosis health visitors who knew the children concerned.
Age sex standardised rates were calculated by ward for all cases of tuberculosis in 0–18 year olds using the 1991 census (The 1991 census, ESRC purchase, Crown Copyright) to provide population denominators. For south Asians, a crude rate was calculated as denominator populations were not available by suitable age–sex strata. Three year moving averages of crude incidence were calculated for south Asian and non-south Asian populations for comparison. The average annual incidence rate was calculated for non-south Asians by regressing the log rate on year and expressing the exponential of the resulting coefficient − 1 as a percentage.
For each ward in Leeds Health Authority, a deprivation score (the Carstairs Index13) and “ethnicity” (the proportion of non-white children under 19 years) were calculated using data from the 1991 census. Population weighted population densities were calculated by ward as this measure was considered to reflect more accurately the density at which the average person lives compared to area based population densities.14
Negative binomial regression modelling examined the association between ethnicity, deprivation, and population density on incidence of tuberculosis in the south Asian and non-Asian populations (Poisson models showed an unacceptable degree of over dispersion, especially when only considering south Asians whose numbers were very low). Each of these variables were divided into five groups having approximately equal populations; they were analysed in relation to all 0–18 year olds (for which the age–sex stratified denominator population data were available), south Asians (for whom only denominator population totals were available), and non-south Asians (also using unstratified population data for ease of comparison). These groups are based on values calculated for each of the 33 wards, hence the discontinuous range values. For all 0–18 year olds, deprivation and population density were each modelled with ethnicity (the proportion of non-white individuals in the population).
Results
DESCRIPTIVE EPIDEMIOLOGY
In the entire study cohort (n = 107), 42 (39.3%) were index cases while 61 (57%) were found by contact tracing. Three cases were diagnosed following screening of new immigrants and one case was found during the school Heaf testing programme prior to BCG immunisation.
Table 1 describes the characteristics of the patient population by age and sex, showing the majority of children in the age group 5–9 years. Thirty eight (35.5%) children in the study were of south Asian subcontinent origin, of whom 25 were girls and 13 were boys, giving a female to male ratio of 1.9:1. The female to male ratio in white children was 1.02:1.
Frequency, proportion, and incidence of children diagnosed with tuberculosis by age group and by sex
Respiratory tuberculosis accounted for 88 (82%) of the cases (57 non-south Asian, 31 south Asian) while 17 (16%) had non-respiratory tuberculosis (11 non-south Asian, six south Asian), predominately tuberculous lymphadenitis (11 cases; 65% of non-respiratory tuberculosis).
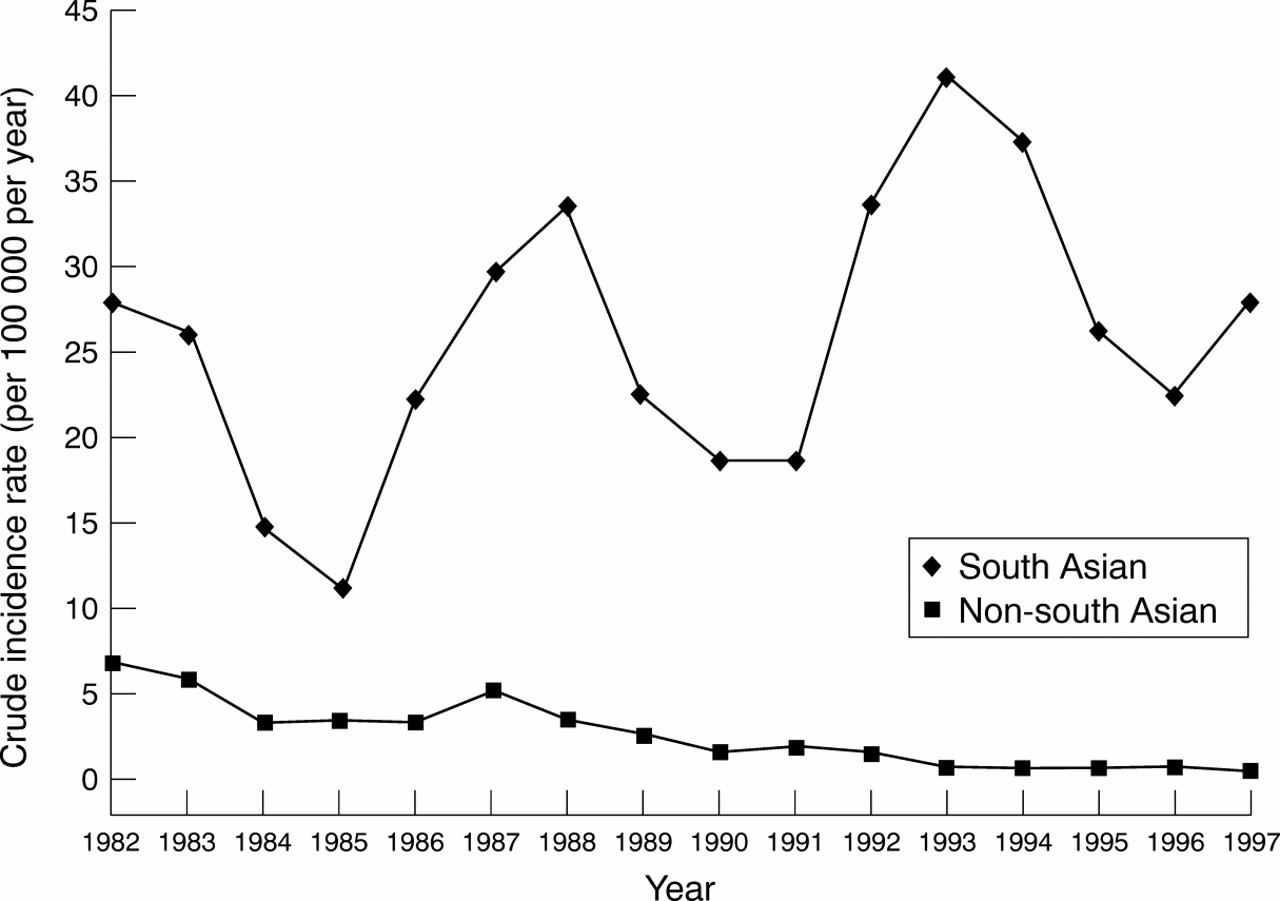
Overall age–sex standardised incidence rate over the period 1982–1997 was 3.9 per 100 000 per year (95% confidence intervals 3.2 to 4.7 per 100 000 per year). Crude incidence rates for 0–18 year-olds of south Asian origin were 25.7 per 100 000 per year (95% confidence intervals 17.4 to 33.9 per 100 000 per year), and 2.7 per 100 000 per year (95% confidence intervals 2.1 to 3.3 per 100 000 per year) for the non-south Asian population. Figure 1 shows three year moving averages for these crude rates by year. There is a significant 13.3% average annual decrease in incidence for the non-south Asian population determined by linear regression (coefficient of log rate = −0.142, p = 0.002). The overall average annual percentage decrease was 6.5% but was not significant (coefficient of log rate = −0.0678, p = 0.067).
{kind=link}
Incidence of tuberculosis in Leeds District Health Authority 1982–1997; three year moving average for south Asian and non-south Asian 0–18 year olds.
ECOLOGICAL ANALYSIS
For the entire study population univariate analysis of each demographic factor by negative binomial regression modelling showed significant positive associations between incidence and ethnicity, deprivation, and population density (see table 2). When analysed separately there were no significant associations for south Asians; for non-south Asians a significant positive association was seen with deprivation but not population density.
Univariate analysis of association between deprivation, population density, and ethnicity, and incidence of tuberculosis in 0–18 year olds in Leeds Health Authority, 1982–1997
In order to investigate further the relation between ethnicity and deprivation and ethnicity and population density, multivariate modelling was performed. Table 3 shows that ethnicity is independently and significantly associated with incidence of tuberculosis when modelled either with deprivation or population density, suggesting that the link with ethnicity is not explained either by deprivation or population density.
Ecological regression analysis of deprivation and population density in relation to ethnicity and incidence of tuberculosis in 0–18 year olds in Leeds District Health Authority, 1982–1997
Discussion
Childhood tuberculosis is often regarded as unimportant in the epidemiology of tuberculosis, as more than 95% of children with tuberculosis are smear negative15 and therefore do not contribute to the immediate spread of the disease. However, childhood tuberculosis is necessarily a result of recent infection and therefore the presence of tuberculosis in children, particularly the younger age groups, reflects continuing transmission in the community. Infected children represent a pool from which a larger proportion of future cases of adult tuberculosis will arise.15 The World Health Organisation estimated that there were 7.96 million new cases and 1.87 million deaths in all age groups as a result of tuberculosis in 1997.16
Under notification of tuberculosis in Britain is well recognised, but its extent is unknown.17 Leeds Health Authority has excellent cross checking systems to ensure accurate notification. The Consultant in Communicable Disease Control receives notifications of all positive cultures from the microbiology laboratories, histopathology laboratories, and the chest clinic. Local pharmacists inform the Consultant of all patients being prescribed combinations of antituberculous drugs. These mechanisms ensure continuous updating of the central tuberculosis register kept at the chest clinic and repeated local surveys have not detected any cases which were not already known to the chest clinic. It is therefore very unlikely that under notification is a significant problem in Leeds.
Our data showed that despite the fact that the total (adult and child) annual number of notified cases has been increasing in Leeds in the last three years of the study (J Watson, personal communication), the annual notifications for children alone have not shown a concomitant rise. The recent increase in adult notifications is likely to be caused by a combination of factors, for example an increase in homelessness, continued immigration, and increased reinfection of people visiting the Indian subcontinent.
Respiratory tuberculosis (82.2%) was much more common than non-respiratory disease (15.9%). There was an unexpected finding of a relatively higher number of south Asian girls with tuberculosis (male to female ratio 1.9:1 in south Asian and 1.02:1 in white children). Gender refers not only to physiological differences between the sexes, but also to the wide variety of behaviour, expectations, and roles attributed by culture to males and females. While much has been written about the influence of socioeconomic and cultural factors related to tuberculosis incidence, such studies have rarely analysed data by sex.18 There are some biological factors which may predispose females to tuberculosis infection. Animal studies suggest that the balance between the endogenous adrenal steroids cortisol and dehydroepiandrostenedione influences the balance of Th1 to Th2 cytokines which is thought to affect the immune response to tuberculosis.19 This would not explain the differential findings between south Asian and white girls in our study. Another recent study20 suggests that 25-hydroxycholecalciferol deficiency may contribute to the high occurrence of tuberculosis in Asians in west London. It is interesting to speculate about whether cultural factors, such as a tendency of Asian girls to spend more time at home, differentially affect vitamin D status, exposure to tuberculosis, or both. Prospective studies may help to explain the gender differential.
This study showed that the most affected age groups were children aged 0–4 years (24.3%) and 5–9 years (39%). These figures are of particular significance as children have been the target of a number of primary preventive measures against tuberculosis infection, including selective BCG immunisation of infants at higher risk. The neonatal BCG programme has been reported to provide between approximately 64%21 and at least 75%22 protection against childhood tuberculosis, with an overall rate of protection estimated at 65% against respiratory disease but almost complete protection against disseminated disease.23 Although the BCG status of our cohort was not fully documented, a previous study from Leeds6 found that none of the active cases received neonatal BCG.
The finding from the ecological analysis that the overall risk of tuberculosis is linked to deprivation, population density, and ethnicity is not new. It is of interest, however, that the risk for ethnicity in the multivariate analysis was independent of both population density and deprivation and therefore not explained by these factors.
The study population was considered to be as complete as possible, but the sources of cases were not independent so the ascertainment could not be formally tested. The numbers included were relatively small and caution in interpretation of the results is therefore important; however, the publication of similar findings from an independent study of tuberculosis9 lends weight to our results.
For the descriptive epidemiology, individuals were flagged as south Asian based on their name, a procedure which may be open to misclassification. However, the Nam Pehchan program,24which identifies part name (stem) or complete matches from a data dictionary of Asian names is used by the City of Bradford Metropolitan Council and Bradford Health Authorities in West Yorkshire and is particularly appropriate for the population in this study. Further checks were made with health care professionals dealing with the Asian families, along with visual inspection of the names; we therefore consider it unlikely that any major misclassification will have occurred.
The ecological analyses used census based variables to measure ethnicity, that is, the proportion of non-white children in the population; it should be noted that measuring summary characteristics of a population residing in an area, however restricted in size, does not necessarily represent the condition of any single individual.25 Despite this, a number of area based studies in the UK,26 ,27 although not all,28 ,29 have shown that census based investigations are a reasonable method of investigating the risk of disease in relation to population characteristics.
Examining our childhood populations of south Asians and non-south Asians (mainly white) separately, we found no links between deprivation or population density for south Asian children, reflecting a similar pattern shown in the combined childhood and adult population in Birmingham.9 For non-south Asian children there was an association with deprivation but not population density. These findings from the ecological analysis, in conjunction with the differential time trends, suggest that disease aetiology and the risk profile may be different for south Asian compared to other children. Our observations make it important for future analyses of overall trends and incidence rates to take account of ethnicity. Failure to do so will lead to misunderstanding of the dynamics of tuberculosis infection in the population.
Acknowledgments
Thanks to Dr John Watson and staff at the Leeds Chest Clinic for access to the data and to Dr Martin Schweiger, Consultant in Communicable Disease Control, Leeds Health Authority for advice.
References
2nd World Congress of the Pediatric Thoracic Disciplines April 26–8, 2000; Izmir, Turkey
Further details: Prof Dr Oktay Mutaf, Ege University Faculty of Medicine, Pediatric Surgery Department. Fax: +90 232 3751288; email:omutaf{at}med.rgr.rdu.tr