Article Text

Abstract
AIM To measure drug adherence in children with mild asthma receiving long term prophylactic treatment.
METHODS Double blind randomised placebo controlled trial. Patients received inhaled budesonide 100 μg or 200 μg daily, or placebo for 27 months. All participants were asked to inhale medication or placebo from two different Turbuhalers (morning and evening) during the study. A total of 122 children (80 boys, 42 girls) aged 7–16 years with mild asthma (mean FEV1 103.7% of predicted) were included in the trial. Drug adherence was assessed by counting the number of remaining doses in the inhaler when study medication was returned at six month intervals.
RESULTS A statistically significant and continuing decrease in measured drug adherence was found from three to nine months and then to 27 months, reaching mean values of 40.6% and 46.9% for inhaled morning and evening medication respectively. Drug adherence declined more rapidly in the placebo group (compared to active treatment); this difference became significant after two years of treatment. Children aged 9 years or less had better drug adherence during the entire study period, but the difference was only significant for the first three months of the study. Measured drug adherence was significantly higher for evening medication compared to morning medication for all study intervals after nine months.
CONCLUSION Measured drug adherence diminishes significantly when treating children with mild asthma in a long term trial. This emphasises the importance of monitoring compliance in clinical trials.
- drug adherence
- patient compliance
- inhaled corticosteroids
- childhood asthma
Statistics from Altmetric.com
Glucocorticoids are the most effective anti-inflammatory drugs in the treatment of asthma and international treatment recommendations currently suggest treating mild persistent childhood asthma with a low dose of inhaled steroids, cromolyn sodium, or nedocromil sodium.1 The fact that airway inflammation has been shown to occur in mild intermittent asthma,2 may possibly result in prophylactic treatment of a milder form of disease. In the authors' opinion this will inevitably lead to increased attention on drug adherence in this group of patients.
Drug adherence can be determined directly by repeated measurement of serum concentrations of the drug (or a metabolite) in question, when methods are available (serum theophylline measurements). Treatment adherence can also be indirectly measured objectively by assessing the use or intake of prescribed medication. This has been assessed electronically in a clinical trial concerning the use of inhaled steroids for 13 weeks in childhood asthma and was reported to be 58%.3 Few studies have however reported objectively measured drug adherence in a long term trial involving children with asthma. Prescribing prophylactic long term therapy in children with mild asthma in order to treat inflammation in the airways and obtaining symptom control may possibly result in a decline in treatment adherence.
Patients and methods
STUDY DESIGN
The study was a double blind, placebo controlled single centre extension trial. The study was a direct continuation of a previous 12 week trial (n = 163), which has been reported and described in detail elsewhere.4 At baseline patients were randomised into four different treatment groups, and each patient received two Turbuhalers, one for morning medication or placebo and the other for evening medication or placebo. Group I patients were given budesonide 100 μg once daily in the morning and placebo in the evening. Group II received budesonide 200 μg once daily in the morning and placebo in the evening. Group III received budesonide 100 μg twice daily. Group IV received placebo twice daily. Clinical assessments were performed at three month intervals during the first year and at six month intervals during the second year.
PATIENTS
A total of 122 children with mild asthma were included in the present study, 80 boys and 42 girls, aged 7–16 years. All were selected from the outpatient clinic at the Section of Allergy and Pulmonology, Department of Paediatrics, Ullevål University Hospital in Oslo. All subjects participated in a two year extension study on the effect of low dose inhaled budesonide on mild asthma, mild being defined as low grade symptoms that did not interfere with sleep and lifestyle, or episodes of cough and wheeze occurring less than once per month.5 Table 1 gives demographic details of participants.
Patient characteristics at baseline
METHODS
Patient drug adherence was assessed by counting the remaining doses in the inhaler device which initially contained 200 doses. This was done at six monthly intervals or when the inhalers were returned. This method has been described in detail elsewhere.4 If inhalers were lost during the study period, patients were provided with new inhalers for the rest of that six month period, but these patients were excluded from the measurement period.
Drug adherence was calculated as:

Patients were not informed of compliance measurements and the results of these were unknown to the study investigator until the study was completed. The study was approved by the regional medical ethics committee.
STATISTICAL EVALUATION
Means were used for the index of location and confidence interval as the index of dispersion. Unpaired t tests were used to compare drug adherence between different groups, and paired t tests were used to compare the difference between morning and evening compliance. Probability values of 0.05 and less were considered to be significant.
Results
PATIENTS
Thirty three patients withdrew during the study period: 19 because of disease deterioration, 14 because of non-compliance, and one because of change of residence. After three months of treatment all inhalers (n = 244) were recovered for measurement from included study subjects. From 9 to 21 months, 94–98% of inhalers of included patients were recovered for measurements, whereas 69% of inhalers (123 of 178) were included in the measurement at the last visit of the study.
DRUG ADHERENCE ASSESSMENT
Mean measured adherence for morning medication dropped significantly (p < 0.05) for twice daily medication: from 76.7% after three months of treatment to 51.7% six months later for morning medication, and respectively from 77.7% to 58.8% for evening medication in the same period. As table 2 shows, mean adherence for twice daily medication continued to diminish throughout the study period. Patients receiving placebo had higher (but not significantly) drug adherence during the first nine months of the study, and thereafter consistently lower adherence when compared to active treatment to the end of the period. This difference was statistically significant during the last six months of the study as shown in table2, which presents the mean adherence values per patient for joined morning and evening medication, with the lowest adherence value for the placebo group at the end of the study (32.1%) compared to 48.7% for budesonide treatment. Figure 1 shows similar trends for the comparison of adherence to morning medication only.
Comparing measured compliance when treating mild childhood asthma with twice daily inhaled budesonide or placebo for 27 months

Measured drug adherence for use of Turbuhaler in the morning, treating mild childhood asthma with inhaled budesonide or placebo for 27 months.
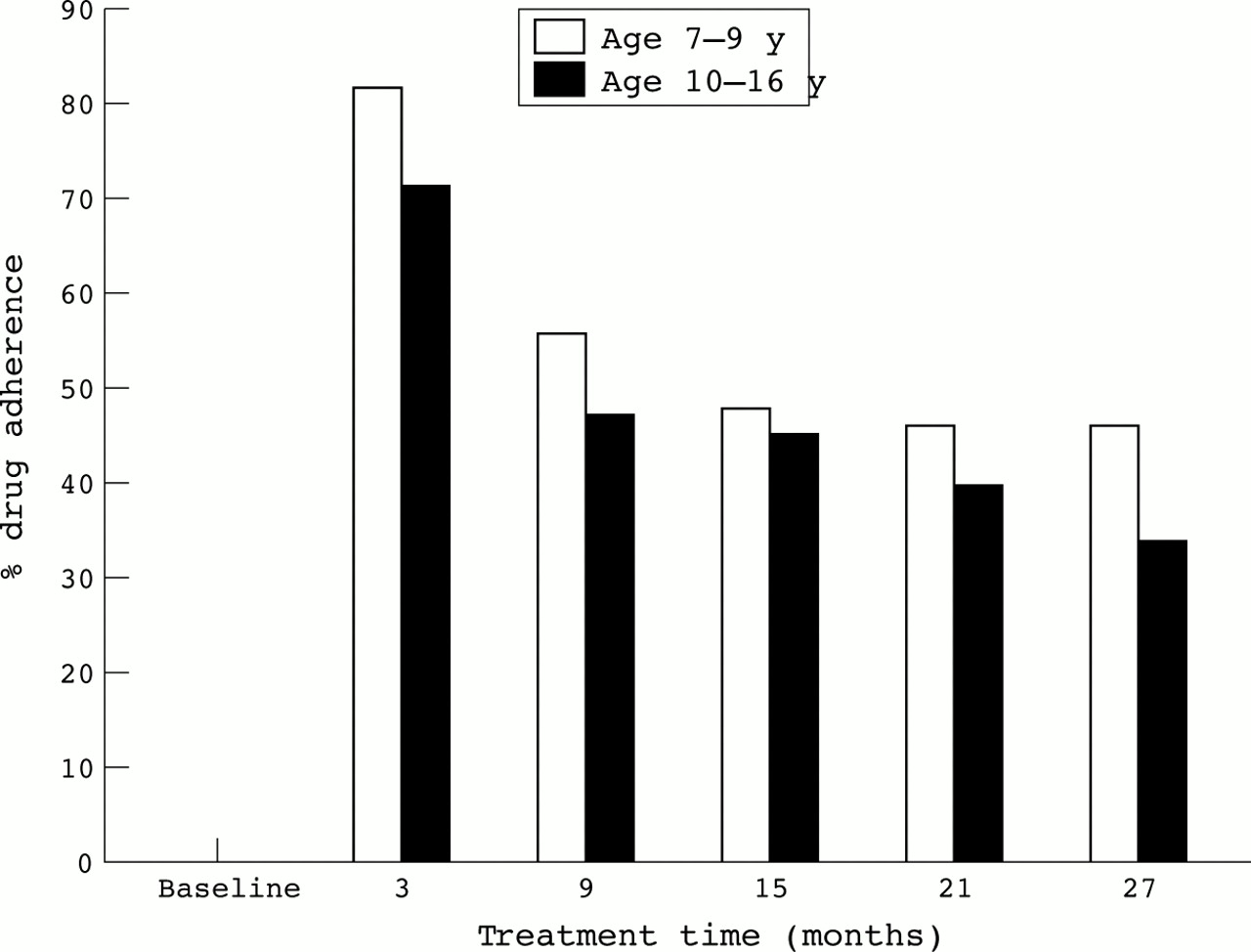
Adherence in two different age groups (7–9 years versus 10–16 years at baseline) was on all occasions higher in the younger age group. This difference was however only significant for the first three months of treatment as presented in table 3 for evening medication and in fig 2for morning medication.
Comparing measured drug adherence for evening medication between two age groups of children with mild asthma treated with inhaled budesonide or placebo for 27 months

{kind=link}
{kind=link}
Comparing measured drug adherence in the morning between two age groups of children with mild asthma treated with inhaled budesonide or placebo for 27 months.
Measured adherence was always higher for evening medication; this difference was statistically significant on all visits after three months of treatment as shown in table 4.
Comparing measured drug adherence between morning and evening doses, when treating mild childhood asthma with inhaled budesonide or placebo for 27 months
Discussion
The present study shows that measured drug adherence in a clinical trial involving children with mild asthma, diminishes significantly with time in a long term study. After nine months of treatment, drug adherence was found to be constantly better in the group of patients that inhaled a low dose of budesonide compared to placebo with significant difference the last six months of the study. Adherence was also found to be significantly better for evening medication at nine months and towards the end of the study. Younger children (7–9 years) had a significantly higher adherence to the inhalation therapy during the first three months of the study, possibly as a result of parental motivation, but this difference seems to be reduced as the adherence decreases.
This study emphasises the importance of monitoring compliance in a clinical trial. This is important with regard to the assessment of a possible dose–response effect of a given treatment; it can also influence the general conclusion to be drawn from a trial, as has been pointed out by others.6 To the authors' knowledge, a long term clinical trial, where drug adherence to asthma medication has been objectively measured for more than two years, has not been reported previously.
As with all other indirect measurements of compliance—counting unused blisters or pills, or using an electronic inhaler timer device (Nebulizer Chronolog Forefront Technologies Inc., Lakewood, Colorado, USA)—the method used in the present study will only reveal the “theoretical best” compliance, as it is not possible to rule out that the patient might have clicked the inhaler without inhaling (“test clicking”), as has been described by others,7in which case the real compliance would be even lower than measured.
Some short term studies on drug adherence have reported overuse of medication,4 ,8 but it cannot be ruled out that this overuse is in some part at least caused by “test clicking” the inhaler. In the present study overuse of medication was not detected at all after the first three months, possibly suggesting that this effect wears off in a long term study as could be expected when adherence gradually diminishes with time, as in the present study.
Fourteen patients with “known” non-compliance were excluded from the study during the 27 month period. Some of these did not return their inhalers back to the clinic and consequently could not be included in the study for the last three or six months prior to their last visit in the study. The exclusion of these patients from the ongoing study can possibly have resulted in somewhat higher adherence results at the end of the study, than would be expected if they had not been excluded. It can therefore be concluded that drug adherence is likely to be underestimated in the present study.
Children participating in the present study all suffered from mild asthma. Our finding that drug adherence became significantly better in the treatment group when compared to placebo is an important observation, possibly suggesting that this low dose of an inhaled steroid was effective in controlling asthma symptoms, hence possibly resulting in a better adherence. Other studies have shown that failure to comply with asthma treatment results in increasing symptoms,3 but in the present study the main objective was to measure changing trend in concordance with prescribed inhalation therapy in mild asthma, rather than the efficacy of the treatment given.
It has been shown that participating in a clinical trial can increase the patient's motivation and compliance,9 and this conclusion is supported by the relatively high measured adherence at the beginning of the present study; nevertheless it shows clearly that patient adherence with the intake of inhaled steroids diminishes rather rapidly as time goes by, even in a clinical trial. We therefore conclude that it seems to be important to monitor patient compliance in order to understand how low it really can be, and find ways to improve it.
Acknowledgments
The authors thank A Sødal for her help in collecting the data. The study was supported by a grant from Astra Draco, Lund, Sweden, who delivered budesonide, terbutaline, and placebo Turbuhalers.