Article Text

Abstract
METHODS The clinical and epidemiological features of 102 children with extra-pulmonary tuberculosis, diagnosed between 1982 and 1998 at P & A Kyriakou Children's Hospital were reviewed.
RESULTS During the past decade, a 50% increase of admissions for extra-pulmonary tuberculosis was observed. The source of infection was disclosed in 48 patients. Diagnoses included superficial lymphadenitis (n = 48), pleural effusion (n = 27), meningitis (n = 16), skeletal tuberculosis (n = 5), miliary tuberculosis (n = 3), abdominal tuberculosis (n = 2), and pericarditis (n = 1). Miliary tuberculosis developed in infants, lymphadenitis and meningitis in preschool children, and pleural effusion and skeletal tuberculosis in older children. None of the patients with extra-pulmonary tuberculosis died; however, six patients with meningitis developed permanent neurological deficits. In these patients, antituberculous treatment was introduced at a median of six days following admission as compared with one day in patients with no complications. Poverty, immigration, and limited access to medical services were common among patients with meningitis.
- M tuberculosis
- extra-pulmonary tuberculosis
Statistics from Altmetric.com
Tuberculosis constitutes the main infectious cause of death worldwide. An estimated 1.3 million cases of tuberculosis and 450 000 associated deaths occur annually in children.1Extra-pulmonary tuberculosis accounts for up to one third of all cases.2 ,3 Children show a higher predisposition to the development of extra-pulmonary tuberculosis.4 ,5 The impact of extra-pulmonary tuberculosis is greatest among infants and young children who tend to develop more severe extra-pulmonary disease, especially meningitis and miliary tuberculosis.4 ,5
A significant increase in the number of children with tuberculosis has been noticed in Greece recently, which is mainly attributed to the immigration shift from Eastern Europe during the past decade. In particular, the annual incidence of childhood tuberculosis in the area of Athens has increased from 7.8 cases per 100 000 children during the 1987–1990 period to 14 cases per 100 000 children during the 1995–1998 period, of which 4.5% (1987–1990) and 31% (1995–1998) occurred in children of immigrants.6 In 1999, the incidence in the general population in Greece was 22 cases per 100 000, of which 43% were immigrants (Infectious Diseases Confirmation and Intervention Center, Ministry of Health, Athens, Greece; personal communication).
In the current study we present our 17 years' experience with extra-pulmonary tuberculosis in children, with emphasis on epidemiological and clinical features, and outcome.
Patients and methods
P & A Kyriakou Children's Hospital is a 510 bed university tertiary care hospital in Athens, Greece. It provides medical services to approximately 800 000 paediatric residents, in association with the only other 800 bed paediatric hospital in this area. Medical services are provided to all children irrespective of country of origin, status of insurance, or other socioeconomic parameters. All children 0 to 14 years old who were admitted with tuberculosis between January 1982 and December 1998 were identified through a computerised database system. Only patients with an extra-pulmonary site of infection were included in the study.
Extra-pulmonary tuberculosis was defined as identification ofMycobacterium tuberculosis through Ziehl–Neelsen acid fast stain and culture in Loewenstein–Jensen or BACTEC media in a tissue or specimen from a site other than lung parenchyma, in association with clinical and/or imaging findings compatible with infection locally. In case of negative cultures, extra-pulmonary tuberculosis was defined as clinical, laboratory, imaging, and/or histopathological evidence of mycobacterial infection in a site other than hilar lymph nodes or lung parenchyma, in association with a positive tuberculin skin test reaction and/or history of exposure to tuberculosis, and exclusion of other diseases. Tuberculin skin test was interpreted at 48–72 hours following intracutaneous injection of 5 tuberculin units of purified protein derivative, and was considered positive or negative when the local induration was at least 10 mm or less than 10 mm, respectively, regardless of erythema. The RT23-SSI and the 5780A Pasteur–Merieux tuberculin lots were used before and after 1995, respectively.
Access to medical services was determined by the completeness of the routine vaccination schedule (diphtheria and tetanus toxoids, pertussis vaccine, and poliovirus vaccine) according to the patient's age. BCG vaccine is administered to all children at the time of school entry (6 years of age) or at any age in children at high risk for tuberculous infection, following a negative tuberculin skin test.
Differences between continuous variables with non-normal distribution were estimated with the Mann–Whitney test. All statistical analyses were two tailed.
Results
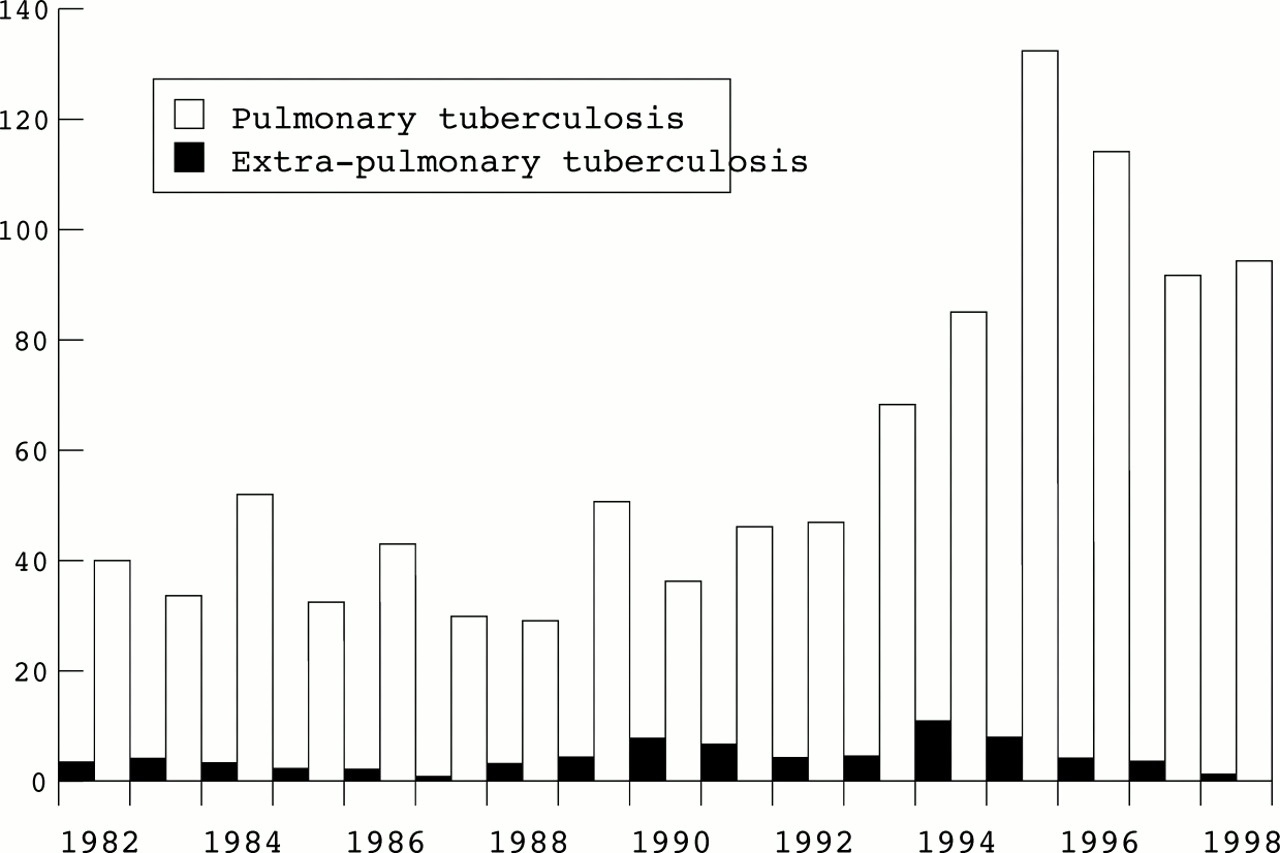
During the study period, 102 children were admitted with extra-pulmonary tuberculosis in our hospital. Between the 1980s and the 1990s, a 50% increase of admissions for extra-pulmonary tuberculosis was noted. The corresponding increase of admissions for pulmonary tuberculosis was 106% (fig 1). Overall, extra-pulmonary tuberculosis accounted for 9% of the total 1161 cases of tuberculosis admitted in our hospital during the study period. Table 1 lists the characteristics of patients with extra-pulmonary tuberculosis. Table 2 shows the site of infection and the corresponding ages of the children. Forty per cent of the cases of extra-pulmonary tuberculosis were culture confirmed (table 3). One multiple drug resistant M tuberculosis strain was detected among the cases studied; all other isolates were susceptible to antituberculous agents.
{kind=link}
Distribution of patients with pulmonary tuberculosis and extra-pulmonary tuberculosis according to year of admission.
Characteristics of 102 children with extra-pulmonary tuberculosis (%)
Distribution of 102 children with extra-pulmonary tuberculosis with reference to site of infection and age
Culture confirmed cases of extra-pulmonary tuberculosis (%)
LYMPHADENITIS
A total of 48 patients were admitted with tuberculous lymphadenitis. Lymph node enlargement was the only sign of infection in 47 of them, preceding their admission by a median of 35 days (range: two days to one year). The remaining patient was admitted with high grade fever; he developed lymph node enlargement three days post-admission. The submandibular and anterior cervical lymph nodes were the most frequently involved nodes.
Twenty four of the 48 patients had a concurrent site of infection, including hilar lymphadenitis (23 patients) and adenoid tonsils and nasal tubercle (one patient). Chest radiographs disclosed a primary focus of infection and enlarged hilar lymph nodes in 21 patients, and calcified nodules in two others; the remaining 25 patients had normal chest radiographs. Tuberculin skin test in 47 patients had a median induration of 15 mm (range 10–30 mm). One patient noted a 5 mm induration.
Treatment consisted of a nine month course of isoniazid and rifampicin (35 patients) or a six month course of isoniazid and rifampicin in association with pyrazinamide during the first two months (13 patients). Thirty three of the 48 patients underwent surgery for diagnostic and/or therapeutic reasons at a median of 60 days (range: two days to one year) following the onset of lymphadenitis, including total excision (27 patients), incision and drainage (five patients), and wide debridement (one patient). Lymph node examination in 29 patients revealed histopathological features compatible with tuberculosis in all and M tuberculosisdetection in 11. In addition, histopathology and cultures revealed tuberculosis in the excised nasal granuloma and adenoid tonsils. Two patients had a second operation; one because of the development of axillary tuberculous lymphadenitis 75 days following total removal of collateral epitrochlear lymphadenitis, and another for aesthetic reasons. Gastric fluid cultures were performed in 15 patients and were positive in eight. Overall, 19 cases of tuberculous lymphadenitis were culture confirmed. In the remaining 29 cases, distinction from non-tuberculous mycobacterial lymphadenitis was based on a positive tuberculin skin test reaction, in association with chest radiographic findings compatible with tuberculosis and/or a history of exposure to tuberculosis.
PLEURAL EFFUSION
Of the 27 patients with tuberculous pleural effusion, 24 had symptoms including fever (22 patients), cough (10 patients), chest pain (seven patients), weakness (five patients), weight loss (four patients), and respiratory distress (two patients). Fever persisted for a median of 10 days (range 1–30 days). In the remaining three asymptomatic patients, pleural effusion was detected through contact investigation of a family member recently diagnosed with tuberculosis. The median tuberculin skin test induration for 26 patients was 20 mm (range 10–30 mm); one patient had no reaction. In addition to pleural effusion, chest radiographs showed enlarged hilar lymph nodes and nodular infiltrates in nine patients, interstitial markings in two, and atelectases in another. Seventeen patients had gastric fluid cultures, nine of which were positive. Fifteen patients received isoniazid plus rifampicin for nine months, and 12 received isoniazid and rifampicin for six months in association with pyrazinamide during the first two months. Adjunctive steroid treatment was administered for six weeks in 13 patients. All 27 patients noted clinical and radiographic response; however, three of them had recurrence of pleural effusion within one month of steroid discontinuation. Residual lesions (parenchymal or lymph node calcifications, or small pleural adhesions) were present at treatment completion in six patients; all others noted complete radiographic resolution.
MENINGITIS
Of the 16 patients with tuberculous meningitis, six were completely unvaccinated, very low income immigrants. Overall, patients with meningitis accounted for 46% of very low income patients, 42% of immigrants, and 25% of completely unvaccinated patients with extra-pulmonary tuberculosis.
All patients with meningitis presented with high grade fever preceding their admission by a median of seven days (range 0–17 days). Fever persisted for a median of 19 days (range 5–50 days). Additional signs and symptoms included nuchal rigidity (12 patients), vomiting (11 patients), headache (nine patients), drowsiness (seven patients), refusal to feed (four patients), weakness (three patients), status epilepticus (one patient), and irritability (one patient). Overall, tuberculous meningitis cases were classified as grades I and II with eight patients in each group.
The median tuberculin skin test induration in 14 patients was 15 mm (range 10–22 mm); two patients had no reaction. Chest radiographs showed nodular infiltrates and enlarged hilar lymph nodes in seven patients and calcified nodules in two. Seven patients had normal radiographs. Computed tomography and/or magnetic resonance examinations were performed in 11 patients and were abnormal in six. Findings included hydrocephalus in all six patients in association with basal ganglia vascular infarcts in one patient, tubercle located at hypophysis in another, and spinal leptomeninges involvement in a third. Microbiological confirmation was established in eight patients. Overall, cerebrospinal fluid (CSF) cultures were performed in 16 patients and were positive in six; gastric fluid cultures were attempted in 11 patients and were positive in four.
Patients with meningitis remained hospitalised for a median of 33 days (range 16–125 days). Antituberculous treatment was instituted in all patients at a median of two days (range 0–8 days) following admission. From 1982 to 1988, treatment for tuberculous meningitis consisted of isoniazid and rifampicin for 12 months in association with streptomycin during the first two months. Beginning in 1989, pyrazinamide for two months was added to the aforementioned regimen. Adjunctive steroid treatment was administered to all patients for a four week period followed by gradual dosage tapering. Five patients developed generalised seizures followed by apnoea, including two who required mechanical ventilation; two underwent shunt surgery for CSF flow relief; two had 7th cranial nerve palsy; and one developed transient diabetes insipidus. None of the patients died. However, two patients noted recurrence of meningitis as a result of non-compliance with treatment. Close supervision of treatment administration ensured their compliance. Regarding long term complications, six of the 16 patients developed permanent neurological deficits including balance impairment and urinary incontinence (two patients), blindness (one patient), quadriplegia, severe mental retardation, and seizures (one patient), fine movements impairment (one patient), and learning disabilities (one patient). Both patients with meningitis recurrence had neurological deficits. The median interval from admission to treatment introduction was six days (range 3–8 days) for patients with long term complications, and one day (range 0–3 days) for patients with no long term complications (p = 0.21). A further comparison between patients with and without long term complications showed that the former patients were younger (median age 3 v 5 years; p = 0.97), had smaller skin test reactions (median induration 7 v 15 mm; p = 0.45) and more pronounced CSF abnormalities (table 4). In particular, increased white blood and neutrophil counts were associated with the development of complications (p ⩽ 0.10). No difference was observed regarding the median interval from the onset of symptoms to time of admission and the addition of pyrazinamide to treatment.
CSF findings in 16 children with tuberculous meningitis
SKELETAL TUBERCULOSIS
Five patients developed skeletal tuberculosis. The following sites were affected: hip–femoral joint (two patients), knee joint (two), and thoracic spine (one). Findings included localised inflammation (four patients), fever (three patients), limping as a result of pain (three patients), and restricted movements (two patients). Isotope scanning showed increased radionuclide uptake from the involved sites. Patients had a median tuberculin skin test induration of 20 mm (range 14–20 mm). Enlarged hilar lymph nodes were shown in three patients; the other two had normal chest radiographs. Surgery was performed in both patients with hip–femoral joint tuberculosis and revealed granulomatous tissue; however, bone cultures were negative. Synovial fluid cultures were performed in one patient with knee tuberculosis and were negative. Treatment consisted of isoniazid, rifampicin, pyrazinamide, and streptomycin for two months, followed by isoniazid and rifampicin for a total of 12 months. Complete clinical and imaging restoration was achieved in all patients within five months of treatment introduction. However, one patient developed chronic painless otorrhoea three months following treatment introduction. Computed tomography showed mastoiditis, and otomicroscopy disclosed white caseous material and granulomatous tissue in the inner ear. Cultures grew a multiple drug resistant M tuberculosis strain. Moderate unilateral high frequency sensorineural hearing loss was manifested. Ethambutol and cycloserin were added to treatment for a total of six months with complete clinical response.
MILIARY TUBERCULOSIS
Three patients developed miliary tuberculosis. The following symptoms were present: fever (three patients), cough (two patients), failure to thrive (two patients), tachypnoea, expiratory wheezing, and prolonged expiration (one patient), and night sweats (one patient). Chest radiographs showed bilateral, diffuse micronodules and lobular consodilation (three patients), atelectases (two patient), and enlarged hilar lymph nodes (one patient). The median tuberculin skin test induration was 10 mm (range 10–15 mm). All patients had positive gastric fluid cultures. Bronchiolitis was initially diagnosed in one infant; steroids were administered followed by clinical deterioration. At that time, the patient's positive tuberculin skin test reaction and its family history of tuberculosis became known and the diagnosis was established. All three patients were successfully treated with a nine month course of isoniazid plus rifampicin, in association with pyrazinamide and streptomycin during the first two months. Steroids were also administered for six weeks. No complications or relapse occurred among the three infants with miliary tuberculosis.
ABDOMINAL TUBERCULOSIS
Two patients developed abdominal tuberculosis; both presented with abdominal distension and fever for two weeks. One patient reported anorexia, fatigue, and low grade fever during the past three months, whereas constipation and dilated superficial abdominal veins were encountered in the other. Both patients had anaemia, positive skin test reactions (16 and 11 mm), and normal chest radiographs. Abdominal imaging revealed enlarged mesenteric lymph nodes and a large amount of peritoneal fluid in both patients, and an enteric–peritoneal fistula in one. No signs of intestinal obstruction were present. Patients received a 12 month course of isoniazid plus rifampicin in association with pyrazinamid for two months. Excellent response was noted. Both patients are free of active infection approximately 10 years following diagnosis.
PERICARDITIS
One child was admitted with fever, chest pain, and respiratory distress of three days duration. Weight loss was noted during the last month. Tuberculin skin test reaction was 20 mm. Chest imaging findings included miliary tuberculosis, accumulation of pericardial fluid, and adhesions within the pericardial space. Paracentesis yielded 300 ml of fluid. Pericardial and gastric fluid cultures grewM tuberculosis. The patient was successfully treated with isoniazid and rifampicin for 12 months in association with streptomycin, pyrazinamide, and steroids during the first two months. No complications or relapse of tuberculosis occurred.
Discussion
Before the availability of agents with activity againstM tuberculosis, the development of tuberculosis was associated with a progressive course and fatal outcome in up to 50% of patients.1 The introduction of antituberculous agents has become the cornerstone of management of such infections. In the current study all children with extra-pulmonary tuberculosis were successfully treated. No deaths occurred.
Tuberculous meningitis remains the most serious form of extra-pulmonary tuberculosis. In the present study, long term complications only occurred in patients with meningitis, permanent neurological deficits developing in more than one third. Younger age and delay in the introduction of appropriate therapeutic agents rendered these children vulnerable targets for the development of serious complications. Similar findings have been reported from other studies.4 ,5 ,7-9 In addition, in the present study, patients with neurological complications tended to manifest smaller tuberculin skin test reactions and more pronounced CSF abnormalities compared to patients without neurological complications. However, with the small number of cases, these observations did not reach statistical significance.
In the present series, tuberculous meningitis manifested as a febrile illness with a median duration of seven days prior to admission in association with a variety of signs and symptoms. A more indolent course has been observed in other series and may postpone the establishment of clinical suspicion for tuberculosis.8 ,9Considering the resurgence of tuberculosis in children, tuberculous meningitis should not be forgotten in the differential diagnosis of meningitis. In such patients, individual risk factors, abnormal chest radiographs, and positive tuberculin skin test reactions may contribute to the diagnosis.10
As expected, superficial lymphadenitis constituted the predominant manifestation of extra-pulmonary tuberculosis among the patients studied.2 However, infants are more susceptible to severe forms of tuberculosis,5 ,11 and in the present study, miliary tuberculosis predominated in infants, superficial lymphadenitis and meningitis in preschool children, and pleural effusion and skeletal tuberculosis in older children, confirming age dependent changes in host–pathogen interactions, described by others.2 ,4 ,11
Increases in the numbers of children admitted with both pulmonary and extra-pulmonary tuberculosis were observed in our hospital during the past decade. These emerging trends reflect the worldwide increasing incidence of paediatric tuberculosis.1 ,4 However, the number of children admitted with extra-pulmonary tuberculosis fell from 1996 to 1998. Beginning in 1993, yearly tuberculin skin test screening of all children up to 6 years of age and then every two years up to 14 years of age was introduced nationwide. The recent fall of admissions for extra-pulmonary tuberculosis may be a result of the early detection of asymptomatic tuberculous infection in Greece.
Several factors have been implicated in the current resurgence of tuberculosis, including the acquired immunodeficiency syndrome (AIDS) epidemic, the emergence of multiple drug resistantM tuberculosis strains, poverty, immigration, homelessness, and inadequate tuberculosis control programmes.1 ,4 ,12 The significance of these factors is further intensified during early childhood, not only because of the immature immune responses of infants and young children, but also as a result of the economic and social dependence of this group of patients. However, in the current study, there were no cases of AIDS, only one multiple drug resistant M tuberculosisstrain was detected, and there were excellent clinical responses to the standard antituberculous regimens observed in all other patients. Despite this, drug resistant tuberculosis is emerging in Greece. In 1998, 9.7% of M tuberculosis isolates from adult patients were resistant to isoniazid, 3.9% to rifampicin, and 4.1% to both agents; 55% of these strains came from immigrants (National Reference Center for Mycobacteria, Hospital for Thoracic Diseases, Athens, Greece; personal communication). In the light of a rise in incidence of resistant strains, treatment with only two agents is no longer recommended as conventional sensitivity testing is not available for several weeks.
Immigrants accounted for only 12% of the study population. The current study extended over a 17 year period. The fact that immigration from Eastern Europe to Greece was greatly intensified during 1992–1997 and that the usual practice of new immigrants is either to immigrate alone or only with their older children may explain this small proportion. Overall, immigration, poverty, unemployment, and restricted access to medical services as indicated by a deficient routine vaccination status, were associated with up to 25% of the cases of extra-pulmonary tuberculosis. However, the source of infection remained unidentified in up to 50% of our patients, so that the relative contribution of each parameter remains uncertain. Of note, approximately 50% of cases in immigrant, very low income, or unemployed families were patients with tuberculous meningitis. Delays in identification and contact tracing of infected adults are common in such groups and render young children at increased risk of developing tuberculosis.4
Childhood tuberculosis reflects the inadequacy of the public health system in controlling transmission of infection in the community.4 ,7 Prompt and efficient identification of the source of transmission and application of effective environmental measures are intimately linked to the control of childhood tuberculosis.