Article Text

Abstract
BACKGROUND Growth hormone insufficiency (GHI) is diagnosed conventionally by short stature and slow growth, and is confirmed by diminished peak GH response to a provocation test. Insulin-like growth factor I (IGF-I) and IGF binding protein 3 (IGFBP-3) have previously been considered individually
OBJECTIVE To test the hypothesis that the combined analysis of IGF-I and IGFBP-3 could act as a surrogate marker for the diagnosis of GHI.
DESIGN Reference ranges for IGF-I and IGFBP-3 were calculated using 521 normal individuals. A retrospective analysis was performed on 318 children referred for investigation of short stature.
RESULTS No significant difference was found between either the IGF-I or IGFBP-3 standard deviation scores (SDSs) in children with and without GHI. If the requirement were for both tests to be positive (< −2 SDS) for a diagnosis of GHI, then 99% of children without GHI would be correctly identified; however, the sensitivity of the test was only 15%.
CONCLUSIONS Neither IGF-I nor IGFBP-3 alone is a marker for GHI. In addition, they cannot be used as an effective screening test in combination.
- insulin-like growth factor I
- insulin-like growth factor binding protein 3
- growth hormone insufficiency
Statistics from Altmetric.com
- insulin-like growth factor I
- insulin-like growth factor binding protein 3
- growth hormone insufficiency
Short stature is a common problem in paediatric practice and although idiopathic growth hormone insufficiency (GHI) is relatively rare (prevalence, 1/3000),1 it deserves consideration because effective therapeutic intervention is available. GHI is a heterogeneous condition. Its diagnosis is suggested by short stature and impaired height velocity but to establish the diagnosis GH secretion must be shown to be abnormal.
Human GH secretion is pulsatile. To make a diagnosis of GHI, GH secretion can be measured by means of a 24 hour profile. This is time consuming and expensive to perform and hence the diagnosis is based conventionally upon the peak GH response to provocation tests, which are not themselves without danger.2
Insulin-like growth factor I (IGF-I) is a well characterised peptide, the product of the interaction between GH and its receptor. It binds avidly to specific binding proteins (IGFBPs) with only about 1% of the circulating IGF-I present in its free form.3 Nutritional status,4 5 and thyroid hormones also influence the levels of circulating IGF-I.6
When a specific radioimmunoassay was first developed for IGF-I,7 early results suggested that IGF-I might be used in screening for GHI.8 However subsequent researchers have found it to be a poor diagnostic marker.9
IGFBP-3 was proposed as an alternative surrogate marker for GHI because its serum concentration is also closely related to GH secretory status.10 11 IGFBP-3 binds to IGF-I and associates with an acid labile subunit to form a high molecular weight ternary complex.12 However, IGFBP-3 alone has a poor sensitivity in detecting patients with GHI and offers no diagnostic advantage over IGF-I.13
We aimed to test the hypothesis that the combined analysis of serum measurements of IGF-I and IGFBP-3 could act as a surrogate marker for the diagnosis of GHI.
Materials and methods
DATA COLLECTION
We measured concentrations of IGF-I and IGFBP-3 on the serum samples of 281 normal male subjects (aged 0.05 to 69.9 years) and 240 female subjects (aged 0.01 to 74.2 years). They had been recruited as normal controls in other research studies and their heights were between the third and 97th centiles on the Tanner and Whitehouse growth charts.
We took blood for the measurement of serum IGF-I and IGFBP-3 from 318 children and young adults (184 boys, aged 1.7 to 25.4 years: 134 girls, aged 0.9 to 19.9 years). They were referred consecutively for GH provocation tests to the London centre for paediatric endocrinology based at Great Ormond Street Hospital (glucagon tests 10 μg/kg) and the Middlesex Hospital (insulin tolerance tests, 0.1–0.15 IU/kg). We also performed auxological measurements on these patients.
ASSAYS
We measured serum IGF-I using an in-house radioimmunoassay (RIA) with acid/ethanol extraction. The sensitivity of the assay was 13 ng/ml. The intra-assay coefficients of variation (CVs) were 9.0%, 5%, and 4.7% at concentrations of 45, 243, and 698 ng/ml, respectively. The interassay CVs were 10.5%, 10.1%, and 5.1% at concentrations of 75, 196, and 698 ng/ml, respectively.
We measured serum IGFBP-3 using an immunoradiometric assay (IRMA; DSL Webster, Texas, USA). The sensitivity of the assay was 0.5 ng/ml. The intra-assay CVs were 3.8%, 3.2%, and 1.8% at concentrations of 7.35, 27.53, and 82.72 ng/ml, respectively. The interassay CVs were 0.6%, 0.5%, and 1.9% at concentrations of 8.03, 21.51, and 76.9 ng/ml, respectively.
GH was measured by the NETRIA and HYBRITRECH immunoassays at Great Ormond Street and the Middlesex Hospitals, respectively. The NETRIA assay is a solid phase IRMA based on reagents from the North East Thames region immunoassay service and has a lower limit of detection of 0.1 mU/l. The intra-assay CVs were 5.1%, 2.4%, and 2.6% at concentrations of 0.8, 4.5, and 86.5 mU/l, respectively. The interassay CVs were 3.3%, 5.2%, and 5.5% at concentrations of 7.7, 21.7, and 45.8 mU/l respectively. The HYBRITECH assay (Hybritech Europe, Liege, Belgium) is also a solid phase IRMA, which is specific for the 22 kDa GH fragment and has a lower limit of detection of 0.5 mU/l. The intra-assay CVs were 10.6%, 5.2%, and 4.9% at concentrations of 1.4, 3.5, and 14.4 mU/l, respectively. The interassay CVs were 10.5%, 7.2%, and 5.4% at concentrations of 6.0, 13.2, and 33.3 mU/l, respectively.14
STATISTICAL ANALYSIS
Using the data obtained on the normal subjects, we were able to plot centiles for IGF-I and IGFBP-3 in boys/men and girls/women. We used exponentially damped polynomials to describe changes in the median, spread, and skewness. We used maximum likelihood estimation to determine the most appropriate models and to test for any significant sex effect. Hence, we expressed centiles parametrically and this allowed relatively simple estimation of age and sex adjusted standard deviation scores (SDSs).15 16
Initially, we considered the short children by dividing them into two groups based upon their peak GH response to a provocation test.
- Group
- I: growth hormone insufficient (GHI: boys, 92; girls, 56).
- Group
- II: non-growth hormone insufficient (non-GHI: boys, 85; girls, 73).
The groups were defined in our study using previously determined GH cut off values specific to the assay in use. In patients undergoing an insulin tolerance test, a cut off value of 13.5 mU/l had been determined for the peak GH response measured by the HYBRITECH assay, below which a diagnosis of GHI could be made.17 Using a similar critical appraisal of the performance characteristics of the NETRIA assay, the cut off value for a peak GH response to a glucagon test was determined at 35 mU/l.18 Other investigators using different GH assays and provocation tests have arrived at other values for the cut off points. In our study, the large differences between the values in the NETRIA and HYBRITECH assays might be related to the designs of the immunoassays. The NETRIA assay uses polyclonal/monoclonal antibodies compared with the HYBRITECH assay, which uses a monoclonal antibody with high specificity to the 22 kDa GH isoform. When these two assays have been compared, the NETRIA assay has been shown to give higher readings for a specific quantity of GH.14
It is well recognised that GH provocation tests, rather than being the ideal “gold standard”, have a high rate of false positives. For this reason, we also considered the prepubertal children according to another parameter suggestive of GHI, namely annualised height velocity standard deviation scores (HVSDSs), to determine whether a similar relation to IGF-I and IGFBP-3 would be seen.
Therefore, we divided prepubertal children into two groups.
- Group
- III: short normals with HVSDS > −0.8 (boys, 33; girls, 28).
- Group
- IV: short, slowly growing with HVSDS < −0.8 (boys, 99; girls, 51).
We used the SPSS statistical package to perform the data analyses. Correlations were calculated using the Spearman test for non-parametric data.
Results
NORMAL RANGES
Normal ranges for IGF-I (fig 1A and B) and IGFBP-3 (fig 1C and D) were constructed from the values obtained for the 521 normal subjects (boys/men, 281; girls/women, 240) aged from 0.01 to 74.2 years. In these individuals the IGF-I and IGFBP-3 values were both age and sex dependent. Peak values occurred at puberty and were followed subsequently by a decline, although the decline was less noticeable in IGFBP-3 than in IGF-I.

Insulin-like growth factor I (IGF-I) concentrations were plotted according to age, from birth to the 7th decade of life, in normal boys/men (A) and girls/women (B). IGF binding protein 3 (IGFBP-3) concentrations were plotted according to age, from birth to the 7th decade of life, in boys/men (C) and girls/women (D). Centile lines (C10 (10th centile), median, and C90 (90th centile)) were calculated from these data and superimposed on the real values.
RELATION OF GH SECRETION AND HEIGHT VELOCITIES TO IGF-I AND IGFBP-3
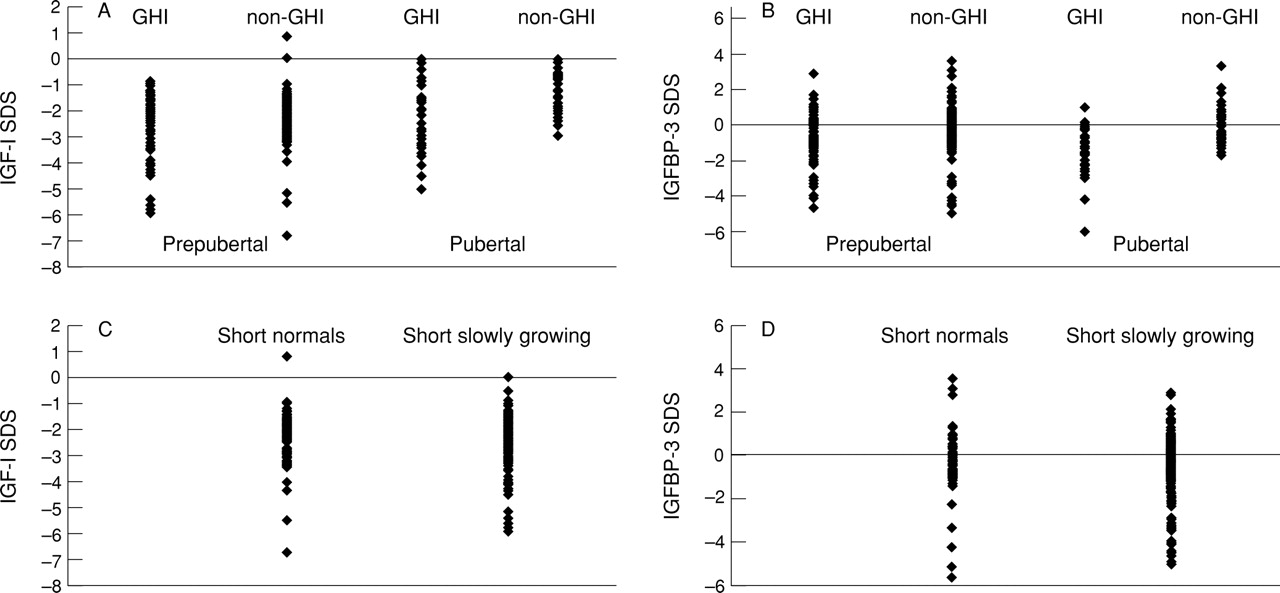
Using these age related normal ranges for IGF-I and IGFBP-3, we converted the values for IGF-I and IGFBP-3 obtained from the children under investigation for short stature to SDS values. Figure 2A shows a plot of the IGF-I SDS values obtained from GHI and non-GHI group. The prepubertal and pubertal children were analysed separately. The IGF-I concentrations were low in all short children (IGF-I SDS < 0) and, although there was a tendency for lower values to occur in the pubertal children with GHI, we could not distinguish between individuals with and without GHI in either the prepubertal or pubertal age range.
{kind=link}
{kind=link}
Serum insulin-like growth factor I (IGF-I) and IGF binding protein 3 (IGFBP-3) measurements obtained for the children investigated for short stature were converted to standard deviation scores (SDSs) using the age related normal ranges. The children were divided initially into two groups according to their pubertal status. For both the prepubertal and pubertal groups IGF-1 SDS (A) and IGFBP-3 SDS values (B) were compared in the growth hormone insufficient (GHI) and non-GHI groups, defined according to the previously described cut off values. In the prepubertal children, the IGF-I SDS (C) and IGFBP-3 SDS values (D) were also compared according to the children’s annualised height velocity (HVSDS): short normals HVSDS > −0.8; short slowly growing HVSDS < −0.8.
Figure 2B shows the results for IGFBP-3. The IGFBP-3 SDS values show a more even distribution around the mean, but again we could not distinguish between children with and without GHI.
In the prepubertal children, we also analysed the IGF-I and IGFBP-3 SDS values based on their annualised height velocity SDS. Figure 2C and D shows the IGF-I and IGFBP-3 SDS values, respectively, in children with HVSDS > −0.8 (short normals) and HVSDS < −0.8 (short slowly growing). Again, we found no significant differences between the two groups, showing that similar results occur regardless of whether height velocity or peak GH values are used to discriminate between the children.
EVALUATION OF IGF-I AND IGFBP-3 “CUT OFFS” FOR THE DIAGNOSIS OF GHI
Using the GH peaks in response to provocation tests as the gold standard method for the diagnosis of GHI, we assessed various cut off points for the IGF-I SDS and IGFBP-3 SDS in terms of their efficiency, sensitivity, and specificity as a single test measurement19 20 (table 1). When considering IGF-I SDS, the sensitivity of the test reached a figure of 62% at best, with an efficacy of 55% at a cut off value of −2 SDS. However, the specificity of the test was only 47%, so using a −2 SDS cut off, a large proportion of children with normal GH values on provocation would be misdiagnosed as being GH insufficient. Similarly with IGFBP-3, the best compromise was a cut off point of −0.5 SDS, with a sensitivity of 61%, a specificity of 68%, and an efficiency of 65%.
Comparison of the sensitivities, specificities, and efficiencies of insulin-like growth factor I (IGF-I) and IGF binding protein 3 (IGFBP-3) measurements at different cut off SDS values
EVALUATION OF A COMBINATION OF IGF-I AND IGFBP-3 TESTS
Both tests required to be negative to identify non-GHI children
The IGF-1 and IGFBP-3 data were analysed according to the approach used by Sackett et al.21 The first hypothesis used was the requirement for both tests to be negative (normal) to identify the non-GHI children (table 2). A negative test was defined as one in which the IGF-I or IGFBP-3 SDS values were > −2 SDS from the mean. However, the sensitivity of this combined test is only 54% and the specificity 64%. Hence, 46% of the normal children would be misdiagnosed as children with GHI.
Both tests required to be negative to identify children without growth hormone insufficiency (GHI)
Both tests required to be positive to diagnose GHI
The second hypothesis used was the requirement for both tests to be positive (abnormal) to make the diagnosis of GHI (table 3). A positive test was defined as an IGF-I or IGFBP-3 SDS of < −2 SDS below the mean. Thus, 99% of children without GHI would be correctly identified. However, with a sensitivity of only 15%, 85% of children who are currently diagnosed as GHI on provocation testing would be missed. We note that if both tests were abnormal a child is highly likely to have GHI.
Both tests required to be positive to diagnose growth hormone insufficiency (GHI)
Discussion
Our data collected on the serum IGF-I and IGFBP-3 measurements in the control subjects of normal height (third to 97th centile) agreed with those reported by others.13 22-24 We found both IGF-I and IGFBP-3 to be highly age dependent. We were interested to note that, although both IGF-I and IGFBP-3 are GH dependent, there is much less of a decline in IGFBP-3 than IGF-I after puberty. This might reflect the influence of other factors present in the circulation causing an uncoupling of IGFBP-3 from its direct relation to the GH response. We found IGF-I concentrations to be below the mean in all short children, although there was a tendency for IGF-I concentrations to be lower in the GHI group. However, there was considerable overlap between the children with GHI and those diagnosed as having idiopathic short stature, making it impossible to discriminate between the two groups. This agrees with other published data.6 Similar patterns of results were obtained regardless of whether the growth failure was defined according to clinical parameters, such as growth velocity, or the gold standard GH concentrations after provocation testing. Others have concluded that IGF-I is a poor discriminator in young children.23 However, in our study population the IGF-I concentrations were low in all short children irrespective of age.
IGF-I is related to GH secretion but the question remains as to why this association is weak when short children are considered on an individual basis. This is probably because of factors other than GH that influence the IGF-I concentration. Some of these are well recognised—namely, nutrition—but other influences are not so clearly defined.
Similarly the IGFBP-3 measurements did not discriminate between the children with GHI and those with a diagnosis of idiopathic short stature, as had been demonstrated previously.13 However, in contrast to IGF-I, IGFBP-3 concentrations were not low in all short children and little is known at present about factors that may influence the uncoupling of this protein from the GH response.
Others have considered the diagnostic roles of the IGFs as molar ratios in serum and concluded that the best measurement for differentiating GHI was the IGF-I: IGF-II ratio.25 Furthermore, the diagnostic roles of urinary IGF-I and IGFBP-3 concentrations have been considered. However, near complete overlap was seen between children with GHI and short normal children.26
We conclude that, at present, there is no easily measured and well defined serum marker for diagnosing GHI. Neither IGF-I nor IGFBP-3 alone is a surrogate marker for GHI and even when analysed in combination they cannot be used as an effective screening test.
Perhaps in the future we will focus more on the components of GH in the circulation. GH is present as a number of differently sized isoforms and current assay techniques primarily measure the presence of the 22 kDa fragment. With the development of assays specific for other isoforms, we can attempt to analyse the relative importance of these to growth in vivo. In addition, we need to consider a spectrum of partial end organ resistance to GH or variation in the biological activity of GH itself.
Acknowledgments
H Mitchell is a Smith and Nephew Medical Research Fellow. We thank Dr AM Wade, Institute of Child Health, London, for performing the statistical analysis of the normal data and creating the IGF-I and IGFBP-3 centiles; Mrs J Jones, Kings College Hospital for performing the IGF-I/IGFBP-3 assays; Ms J Pringle and Mrs B Leonard, Cobbold Laboratories, The Middlesex Hospital for performing the Hybritech GH assays; and Dr A Winrow, Kingston Hospital for providing the normal adolescent control samples.