Article Text

Abstract
AIMS To assess compliance with Department of Health guidelines on weaning practice in a representative sample of 127 infants from Glasgow, and to identify factors influencing timing of weaning.
METHODS Questionnaires on feeding and weaning were completed during home visits. Ninety eight mothers completed a further questionnaire on attitudes to weaning
RESULTS Median age at introduction of solid food was 11 weeks (range 4–35 weeks); only 7% of infants had not been weaned before age 4 months. There was no difference in timing of weaning between boys and girls. Younger mothers (< 20 years old), those of lower socioeconomic status, and those who formula fed their infants tended to introduce solids earlier. Infants who were heaviest before weaning were weaned earlier. Seventy three of 98 mothers reported that they weaned their babies because they felt that they required more food. Sources of information influencing time of weaning were previous experience (53/98), books and leaflets (43/98), advice from the health visitor (31/98), and family and friends (15/98). Sixty five of 98 mothers reported receiving formal information on weaning, in most cases (54) this was from the health visitor. Mothers who received formal information tended to wean their infants later. Two per cent of infants had been given cow’s milk as a main drink by age 6 months, 17% by 9 months, and 45% by the end of the first year.
CONCLUSION Compliance with recommendations on timing of weaning (not before 4 months), weaning foods, and cow’s milk consumption in Glasgow is poor, although no poorer than in many other areas of the UK as found by Office of Population, Censuses and Surveys. Public health messages in relation to weaning may not be reaching their target audience.
-
Non-compliance with recommendations on weaning practice is common
-
Compliance is sensitive to education and the input of health professionals
-
To improve compliance families with lower educational attainment and of lower social class should be targeted
- weaning
- anthropometry
- nutritional status
- cows’ milk
Statistics from Altmetric.com
Clear recommendations exist for weaning practice in the UK1: “The majority of infants should not be given solid food before four months”; “cow’s milk should not be used as a main drink before one year”; “semi-skimmed milk is not suitable as a main drink before two years of age” and “first weaning foods should be non-wheat cereals and pureed fruit and vegetables”. There is increasing evidence of non-compliance with these recommendations,2 and there is debate as to the seriousness of non-compliance with some of them.3 4 In addition, maternal attitudes to weaning are often inappropriate and misinformed5; in some cases this can lead to unsuitable weaning diets.6
This study aimed to assess compliance with weaning recommendations in a representative sample of infants from Glasgow, a city characterised by poor compliance with recommendations in other aspects of infant feeding7 (low breastfeeding rates), to identify the factors that influenced weaning practice, and to assess the contribution of formal advice to weaning practice.
Methods
The sample of healthy, term (37–42 weeks’ gestation) singletons was selected, in 1992 and 1993, using a stratified random sampling frame based on postal code sector. Standard anthropometric measurements (weight, recumbent length, head circumference, and triceps and subscapular skinfolds) were made for the Glasgow longitudinal infant growth study during home visits made monthly until 6 months old then at 9, 12, 18, and 24 months. During the home visits, infant feeding and weaning practice (defined here as introduction of semisolid or solid foods) was described and measured by completion of the Office of Population, Censuses and Surveys (OPCS) questionnaire used in the UK surveys of infant feeding practice.2 An additional questionnaire was used to assess (by self report) maternal attitudes to weaning, factors influencing timing of weaning, and sources and nature of information used by mothers when deciding when to wean.
Group mean comparisons were made by t test; χ2 tests were used to test the significance of differences in the proportions of infants between categories.
Results
SAMPLE CHARACTERISTICS
The sample was similar to the postal code areas from which it was drawn, and similar to the Greater Glasgow Health Board area, in terms of social class (table 1) and infant feeding practice (45% breastfeeding at the end of the first week v43% from the postal codes sampled). The breastfeeding rate observed was similar to that found for Scotland in the 1990 OPCS infant feeding survey (fig 1).2
Social class distribution (%) of subjects and of local and regional geographical area

Breastfeeding rates compared with the OPCS 1990 infant feeding report.2 Blank, Glasgow longitudinal infant growth study; Shaded, OPCS data for Scotland 1990; Filled, OPCS data for the UK 1990.
TIMING OF WEANING
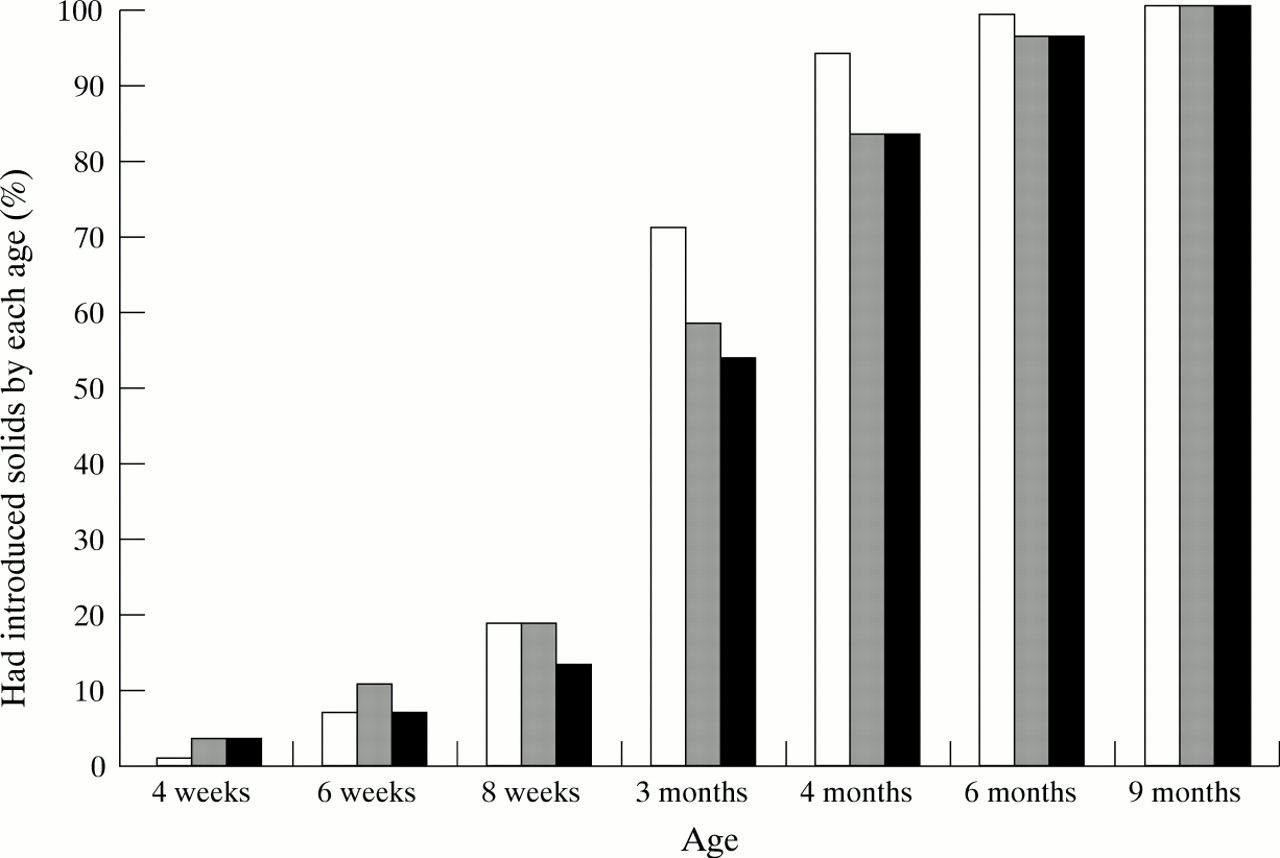
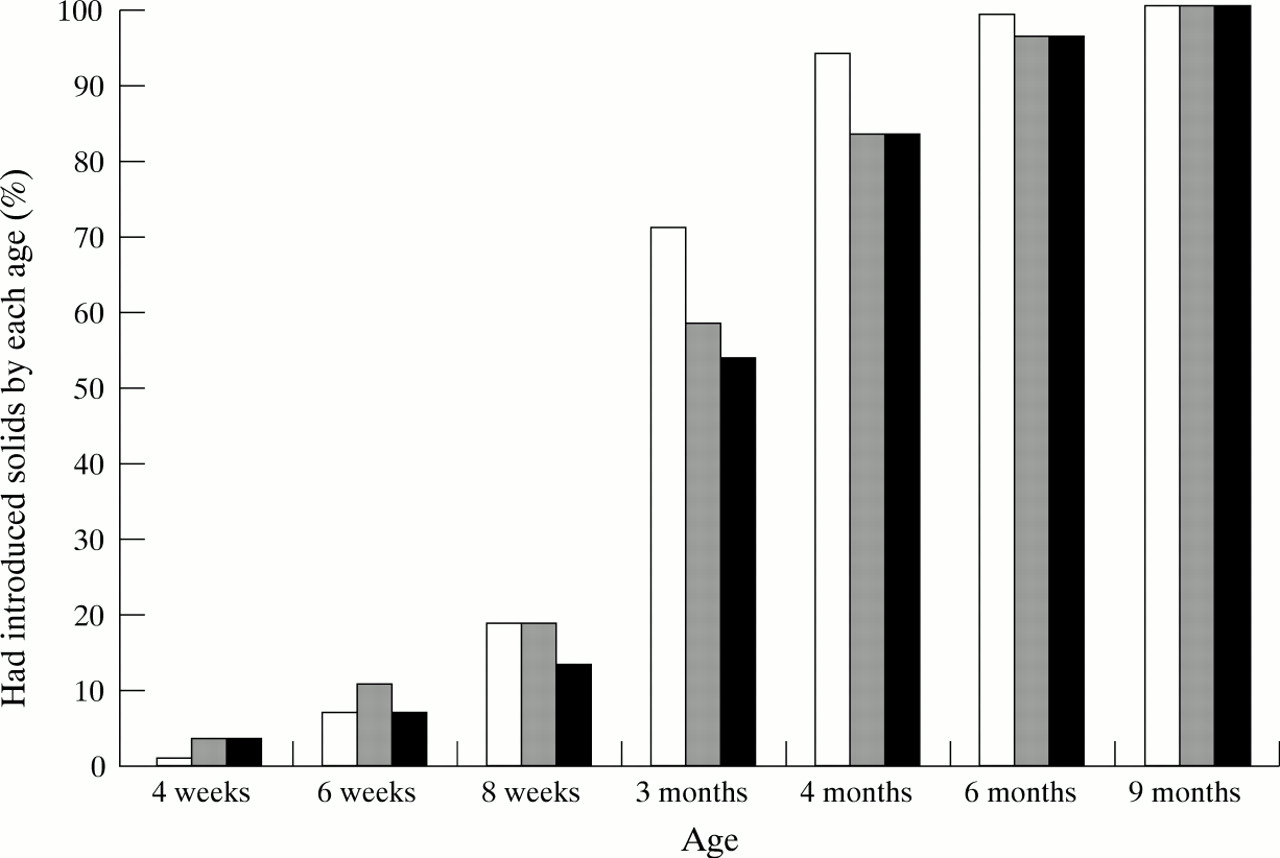
Median age of introduction of solid food was 11 weeks (range 4–35 weeks). Only 7% of the sample had not introduced solids by 4 months old (the recommended time of weaning). This was similar to that reported for Scotland and the UK2 in the 1990 OPCS infant feeding survey (fig 2).
{kind=link}
{kind=link}
Percentage of mothers who had introduced solid food by age of infant compared with OPCS 1990 infant feeding report.2 Blank, Glasgow longitudinal infant growth study; Shaded, OPCS data for Scotland 1990; Filled, OPCS data for the UK 1990.
There was no significant difference in timing of weaning between boys and girls. Younger mothers tended to introduce solids earlier (table2). Weaning was later in those of higher socioeconomic status (χ2 test for proportion weaned before 10 weeks and on or after 10 weeks, p < 0.01) and in mothers who had higher or further education (Mann-Whitney test, p < 0.05). Nine per cent of mothers in social class I and II, and 31% in social class III and below had introduced solids by 10 weeks. Breast fed infants were weaned later than formula fed infants (median 12 v 11 weeks, Mann-Whitney test p < 0.001). Eight per cent of mothers who breast fed weaned by 10 weeks compared with 33% of mothers who formula fed. The infant’s weight at 1 month was also related to timing of weaning: heavier infants were weaned earlier. Weight at 1 month was negatively correlated with age at introduction of solids (multiple regression; p < 0.05).
Median age of weaning and percentage of sample weaned by age of mother
Of the 127 mothers in the sample, 98 completed an additional questionnaire on attitudes to and information on weaning. There was evidence of an association between the provision of formal advice and timing of weaning. Of 65 mothers who sought or received formal advice, only nine introduced solids before 10 weeks compared with 12 of 33 mothers who had not received formal advice.
FIRST WEANING FOODS
Commercially prepared cereals were the most commonly used first weaning foods, used by 102/127 mothers (82%). This consisted of baby rice (66%), baby cereal (9%), and rusks (5%). Only six infants (5%) were given fruit or vegetable purees as their first weaning food. The remaining 14% were introduced to solid food with other commercial baby foods.
USE OF COW’S MILK AND REDUCED FAT MILK AS A MAIN DRINK
By 6 months of age, two infants (2%) were given cow’s milk as their main drink. This increased to 22 (17%) at 9 months, and 55 (45%) by the end of the first year. These proportions were smaller than those found by the OPCS infant feeding survey2 where 36% had used cow’s milk as a main drink by 9 months. Semiskimmed or skimmed milk was used as a main drink in five (4%) of the Glasgow sample by 1 year.
ATTITUDES TO WEANING AND SOURCES OF INFORMATION
Ninety eight mothers were asked for their attitudes to weaning and on sources of information; they could give more than one answer to each question.
The two reasons most often reported as to why mothers weaned their child were (1) the perception that the infant was “not satisfied with milk feeds and was hungry” (73 of 98 mothers), (2) “because the baby was not sleeping through the night” (20 mothers).
Knowledge as to when to wean and what foods to use were obtained by 53 of the 98 mothers from previous experience, 43 from books and leaflets, 31 acted on advice from the health visitor or doctor, and 15 obtained advice from family or friends. When asked if any formal advice was received from health professionals, 65 of 98 mothers reported having some type of formal information. In most cases (54 of 65) this was from the health visitor or doctor and in 21 of 65 this was from books or leaflets.
Mothers were asked which factor had the greatest influence on their decision to introduce solids and their choice of solid foods; advice from the health visitor or doctor was not the main influence reported. Only 28 of 98 mothers reported that the health visitor or doctor had the greatest influence on when to wean their baby and, as noted above, the perception that weaning was necessary to “satisfy” the infant was dominant.
Discussion
The results confirm widespread non-compliance with current UK recommendations1 in relation to timing of weaning, use of cow’s milk as a main drink, use of reduced fat milk as main drinks, and first weaning foods.
Breastfeeding rates in Glasgow are low.8 Timing of weaning was earlier than recommended1 but similar to UK data on infant weaning practice.2 Compliance with recommendations in relation to cow’s milk was marginally better than UK data.2 In summary, these results suggest that low levels of compliance with UK recommendations were not the result of factors specific to the sample, or to Glasgow.
The public health implications of non-compliance on such a scale remain unclear.3 4 The most serious discrepancy between actual practice and recommendations is in timing of weaning. Early introduction of solids has been discouraged because it is believed to encourage excessive weight gain, increase the risk of infection, and increase the risk of allergic disease.1 There is a consensus that early weaning is hazardous and should be avoided.1 However, Forsyth et al showed that early introduction of solids might be less harmful than was previously thought, and they suggested a more flexible approach to recommendations on weaning practice.4
Around two thirds of mothers received formal advice about weaning practice, but most reported that other factors influenced their decision on weaning. In particular, 74% reported a perception that infants were hungry, and 20% reported infant sleep disturbance. Previous studies have reported that infant body size influences timing of weaning, independent of other factors,2 4 implying that timing of weaning is matched to the physiological needs of the infant, at least in part. Other factors that influenced timing of weaning in the present study were those already described2: mothers who used formula feeding, those who were younger, and those in lower social classes, tended to wean their infants earlier. The observations that mothers who did not receive formal information on weaning, who formula fed, and those of lower social class and educational attainment tended to wean their infants earlier, suggests that weaning practice can be influenced by education.
The importance of non-compliance with current recommendations in relation to cow’s milk feeding, use of reduced fat milks, and first weaning foods is difficult to assess, and such an assessment is beyond the scope of this study. Recommendations on the use of cow’s milk in infancy are based on concerns related to iron deficiency1and recommendations related to reduced fat milks are based on concerns that low energy intake might compromise growth and nutritional status.3
The importance of maternal attitudes to breastfeeding has long been recognised as an important element in achieving compliance with UK recommendations.9 Parental attitudes to weaning practice have received less attention but would appear to be often misinformed,5 with adverse consequences for some infants.6 Further research on the importance of parental attitudes and beliefs would help elucidate the underlying causes of non-compliance with Department of Health recommendations on weaning,2 and further research on the public health implications of non-compliance is recommended.
In view of the potential hazards,1 public health strategy should continue to focus on avoidance of early weaning. There may be a case for relaxing the recommendations4 on weaning practice, but as these represent a critical review of the available evidence, any modification of current advice must be approached with care. Recommendations are generally cautious, seek to avoid risks to public health, and should not be modified without a further review of the evidence.
The extent of non-compliance shown by this study could lead to the conclusion that current guidelines are failing to reach their target audience. Our evidence that weaning practice was sensitive to education, social class, and the input of health professionals, implies that there is some scope for improvement in this area. Such an improvement might be practical if educational messages can be focused on the appropriate groups—that is, on families of lower social class and educational attainment.
Acknowledgments
The authors thank all parents and children involved in the study. The study was supported by Milupa Ltd. We are also grateful to the Greater Glasgow Health Board Information Unit (Gerry Smith; Dr John Womersley) for advice on the sampling frame and access to census data.