Article Text

Abstract
OBJECTIVE To investigate possible renal toxicity of long term gentamicin inhalation in patients with cystic fibrosis.
METHODS Urinary N-acetyl-β-d-glucosaminidase (NAG) activity was measured during routine respiratory clinic visits. Outpatient records were reviewed for data on long term gentamicin inhalation, and parents and patients were interviewed for compliance. Exclusion criteria were irregular gentamicin inhalation, urinary infection or other febrile illness, intravenous aminoglycoside treatment during the previous three months, and diabetes mellitus. Patients were assigned to three groups: group 1, current gentamicin inhalation; group 2, previous gentamicin inhalation that had been stopped at least three months ago; and group 3, never any gentamicin inhalation.
RESULTS 52 patients (34 girls, 18 boys), mean (SD) age 11.5 (5.7) years, entered the study. Patients currently on gentamicin inhalation (n = 20) were significantly younger and had higher urinary NAG activity (0.83 (0.57) U/mmol creatinine) than the 23 patients without gentamicin inhalation (0.26 (0.10) (p = 0.0001) and the nine patients with previous gentamicin inhalation (0.32 (0.15) (p = 0.0125). Twelve patients on current gentamicin inhalation had raised NAG values but all those in groups 2 and 3 had NAG values within the normal range. In patients currently on gentamicin inhalation, there was a positive correlation between urinary NAG activity and cumulative dose of nebulised gentamicin (r = 0.60, p = 0.0049).
CONCLUSIONS Long term gentamicin inhalation in patients with cystic fibrosis poses a risk of renal toxicity. It is not known whether further treatment might result in more severe renal damage.
- N-acetyl-β-d-glucosaminidase
- cystic fibrosis
- gentamicin
- kidney function
Statistics from Altmetric.com
Lung disease in cystic fibrosis is characterised by chronic bacterial infection of the airways and progressive tissue damage.1 Antimicrobial treatment is usually targeted toPseudomonas aeruginosa, and, as well as repeated courses of intravenous antibacterial treatment, inhaled antibiotics are increasingly used for long term home treatment.2 Several studies have explored the value of antipseudomonas treatment given by nebuliser in cystic fibrosis,3-11 and a recent meta-analysis clearly documented a clinical benefit.12However, concern arises over the potential side effects of aminoglycosides although no case of ototoxicity or nephrotoxicity in cystic fibrosis patients on long term aminoglycoside inhalation has been reported so far.2
N-acetyl-β-d-glucosaminidase (NAG) is a lysosomal enzyme present in high concentrations in the renal proximal tubular cells. Its molecular weight of 140 kDa does not permit glomerular filtration; thus increased urinary NAG activity is one of the most sensitive markers of renal disease.13 It predominantly reflects tubulointerstitial renal lesions including those caused by aminoglycosides and other drug toxicity.14
To investigate the possibility of subclinical renal toxicity, we measured urinary NAG activity in cystic fibrosis patients on and after long term gentamicin aerosol treatment.
Methods
Clean midstream urine was collected from all cystic fibrosis patients who visited the respiratory outpatient clinic during a period of three months. Cystic fibrosis had been diagnosed in all patients by typical clinical symptoms in combination with positive sweat tests.15
Outpatient records were reviewed for data on long term inhalation of gentamicin, the only aminoglycoside used for aerosol treatment in this centre. Gentamicin inhalation had been used because of repeated positive sputum samples for gentamicin sensitive strains of Ps aeruginosa in combination with clinical and lung function signs of respiratory deterioration. The single dose of nebulised gentamicin was 120 mg, diluted to 4 ml with saline, and inhaled from a jet nebuliser (Pari Master, Pari, Starnberg, Germany). Patients with more severe disease had inhaled this dose twice daily, and those with milder forms once daily, throughout the entire treatment period. Some patients had been changed from two to one gentamicin inhalations a day if a sustained clinical improvement was observed or if there were problems of compliance or practicability. Gentamicin inhalation had been stopped in some patients because of the emergence of gentamicin resistant bacterial strains in sputum samples.
Parents and patients were interviewed for long term compliance with gentamicin inhalation and patients who admitted to irregular inhalation were excluded from analysis. We also excluded patients with urinary or other infections or intravenous aminoglycoside treatment during the previous three months, and those with diabetes mellitus, as these factors can influence urinary NAG activity.16 17
The remaining patients were assigned to one of three groups: group 1, those with current gentamicin inhalation; group 2, those with previous gentamicin inhalation that had been stopped at least three months ago; and group 3, those without any past or current gentamicin inhalation. In groups 1 and 2 we calculated duration of treatment and cumulative dose of nebulised gentamicin.
Urinary NAG activity was measured using a commercially available kit (Boehringer Mannheim, Mannheim, Germany) with cresolsulphonphthalein-glucosaminide as substrate; values were normalised for urinary creatinine, as measured by the Jaffé reaction. In children over two years of age, the upper limit of the normal range for this method in our laboratory is 0.6 U/mmol creatinine.18 Routine urine analysis was also performed.
Informed consent for the study was obtained from parents and patients.
STATISTICS
Data are presented as means (SD). The Mann-Whitney non-parametric test and linear regression analysis by the least squares method were used for statistical analysis. A p value of 0.05 was considered as the limit of significance.
Results
Of 68 cystic fibrosis patients seen in the outpatient clinic, two were excluded because of poor compliance with gentamicin inhalation, five because of recent infection, three who had received intravenous aminoglycoside treatment within the past three months, and two because of diabetes mellitus. Four patients were unable to produce urine for testing.
The remaining 52 patients (34 girls and 18 boys) were aged 11.5 (5.7) years (range 3 to 25). Urine analysis was normal in all of these. The data for each group are shown in table 1 and significant differences are indicated. Group 1 patients were significantly younger and had higher urinary NAG activities than patients in groups 2 and 3. Twelve of the 20 patients in group 1 had urinary NAG values above the upper limit of the normal range. All patients in groups 2 and 3 had values within the normal range, and there was no significant difference between these two latter groups.
Data from 52 patients with cystic fibrosis currently on treatment with inhaled gentamicin (group 1), previously treated with gentamicin (group 2), or never treated (group 3)
For group 1 there was a positive correlation of urinary NAG activity with cumulated dose of inhaled gentamicin (r = 0.60, p = 0.0049). The correlation of urinary NAG activity with duration of treatment did not reach significance (r = 0.41, p = 0.071). Fourteen of the 20 patients had inhaled 120 mg twice daily throughout the entire treatment period, three had had their treatment frequency reduced to once daily after periods of three, 16, and 22 months, respectively, and three had always inhaled 120 mg once daily.
For the subgroup of 14 patients who had always inhaled twice daily, the correlation between cumulated dose of gentamicin (186 (122) g; range 54–498) and urinary NAG activity (0.95 (0.60) U/mmol creatinine; range 0.25–2.24) remained significant (r = 0.63, p = 0.015). As expected, the correlation between the duration of treatment (774 (510) days; range 224–2075) and urinary NAG activity reached the same significance.
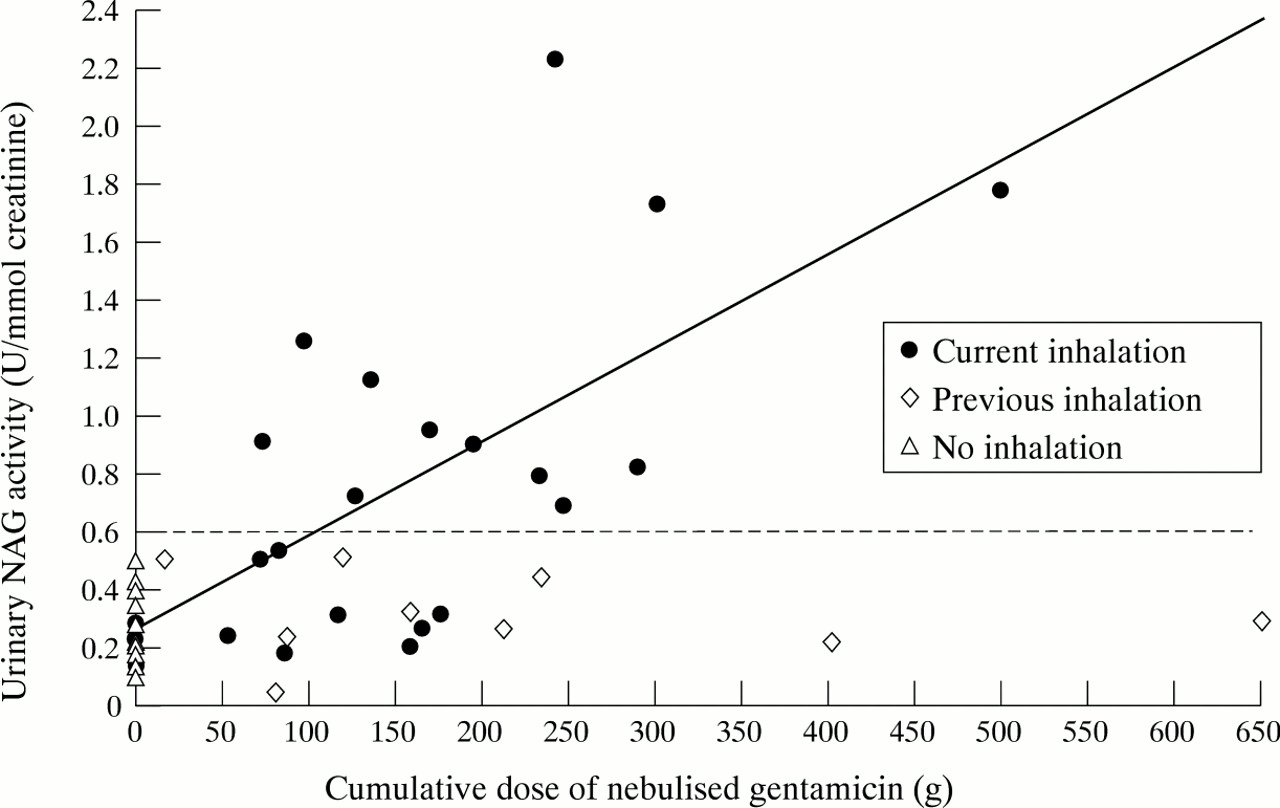
Figure 1 shows individual urinary NAG activities for all three groups and the correlation between NAG values and cumulative doses of nebulised gentamicin for the group with current gentamicin inhalation.

{kind=link}
Urinary NAG activity and cumulated dose of nebulised gentamicin for all 52 patients, and regression line for the group currently on gentamicin inhalation. The horizontal line indicates the upper limit of normal NAG values.
Discussion
We have shown significantly raised urinary NAG activity in cystic fibrosis patients currently inhaling gentamicin. Urinary NAG activity also correlated significantly with the cumulated dose of nebulised gentamicin, thus indicating a straightforward dose–response relation between inhaled gentamicin and renal damage. The normal urinary NAG activity in patients with previous gentamicin inhalation suggests that such renal damage from long term gentamicin inhalation is reversible.
The patients currently on gentamicin inhalation were significantly younger than those in the two other groups. The somewhat older age of patients who had previously stopped gentamicin inhalation because of emerging bacterial resistance against gentamicin is explained by the time taken for bacterial strains to lose sensitivity to aminoglycosides. The group that never received gentamicin inhalation included some older patients with milder forms of the disease and without bacterial colonisation. We considered whether this age difference could have influenced the difference in NAG activity but this is highly unlikely as there are no age related fluctuations in NAG reference values beyond infancy.13 19 Furthermore, the additional finding of a significant correlation between the cumulated dose of nebulised gentamicin and urinary NAG activity strongly argues for a cause–effect relation between long term aminoglycoside inhalation and raised urinary NAG activity.
We could calculate only the cumulated nebulised dose; the amount of drug actually inhaled by individual patients will have been much smaller. Others have shown that less than 10% of the antibiotic placed in the nebuliser is deposited in the lungs, while approximately half of the dose remains attached to the walls of the nebulising system.20 21 To cause renal toxicity, some of the inhaled drug must have been absorbed systemically from the respiratory or the gastrointestinal tract, or both. It has been shown that such systemic absorption of nebulised aminoglycosides can occur. One pilot study from this centre demonstrated measurable and dose dependent serum concentrations of gentamicin after inhaling doses from 120 to 600 mg.22 Others have also found measurable serum concentrations after inhalation of tobramycin.8 9 23With a few exceptions that have to be interpreted as analytical or sampling errors,24 these serum concentrations were low, indicating a relatively small degree of systemic absorption. Correspondingly, the 24 hour urine recovery of inhaled tobramycin was found to be no more than 0.008% to 1.4% of the nebulised dose.10
Three groups have investigated cystic fibrosis patients for renal toxicity after aminoglycoside inhalation and failed to detect any signs of renal damage.8-10 One of these studies used urinary NAG measurements.8 The investigators observed urinary NAG activities from 0.26 to 3.44 U/mmol creatinine after five to 25 months of tobramycin inhalation. Surprisingly, they interpreted these values as within the normal range for cystic fibrosis patients. In a previous study, the same group measured a urinary NAG activity of 0.65 (0.21) U/mmol creatinine in 23 cystic fibrosis patients and found these values no different from those of healthy controls.25 These investigators also observed reversible increases of urinary NAG values with intravenous tobramycin treatment.25 Some of our patients with current or previous gentamicin inhalation had also received one or more two-week inpatient treatment courses with intravenous aminoglycosides because of respiratory deterioration despite gentamicin inhalation. Theoretically, such systemic treatment could have contributed significantly to the observed renal damage, but the finding of normal NAG values after terminating intravenous treatment and our observed correlation between NAG activities and nebulised doses argue against such an interpretation of our results.
Our findings of increased urinary NAG activity with long term gentamicin inhalation and the correlation with the cumulated nebulised dose suggest a dose–response relation. They indicate subclinical renal damage, but the clinical implications remain unclear. The mechanisms of aminoglycoside induced renal damage are understood to be as follows26: initially, there is binding of the drug to tubular brush border membranes, and this is followed by endocytosis and transfer to tubular cell lysosomes; subsequently, these lysosomes start to leak and rupture. Advanced toxicity is characterised by tubular necrosis and eventually renal failure. These mechanisms explain why increased urinary activity of lysosomal enzymes like NAG is an early sign of renal toxicity. With a relatively low systemic absorption of inhaled aminoglycosides, the observed increase in NAG activity is most likely to be a function of both dose and duration of treatment. In fig1, the regression line crosses the upper limit of normal urinary NAG activity at a cumulated nebulised dose of 110 g gentamicin, thus approximately indicating the likely cumulative dose for first signs of renal toxicity. It remains possible, however, that long term aerosol treatment, exceeding the duration of treatment in our study, might cause more severe or even permanent renal damage. This concern could be of particular relevance given the recently suggested policy of high dose treatment with inhaled aminoglycosides, up to 1800 mg of tobramycin daily.11 One previous study that documented normal serum creatinine levels after a treatment period of 32 months9 cannot be extrapolated to guarantee the safety of substantially longer treatment periods.
A further question that cannot be answered by our results is whether these findings are specific for gentamicin or are also valid for other aminoglycosides. Previous work has suggested that tobramycin might have lower toxicity than other aminoglycosides.27 Consequently, increases in urinary NAG activity might be less pronounced with long term tobramycin inhalation, but this remains to be evaluated.
CONCLUSIONS
We found raised urinary NAG activity in cystic fibrosis patients on long term gentamicin inhalation and showed a correlation with the cumulated dose of nebulised drug. This evidence for subtle renal damage or tubular dysfunction raises the question whether longer term treatment might result in more severe renal toxicity. We recommend repeated assessments of urinary NAG activity in cystic fibrosis patients on long term aerosol treatment with aminoglycosides.