Article Text

Abstract
A paediatric day assessment unit was opened in May 1995. An audit of the first year’s activity showed that, despite an increase in emergency admissions of 8.4%, the number of children admitted as an emergency overnight was reduced by 3% in paediatrics and 7.2% in surgery. In the first year, 1731 children were assessed as an emergency of whom 658 did not require admission to the inpatient ward. Midnight occupancy fell 17.7 % in paediatrics and 25.4% in surgery. The nurse staffing costs fell over £32 000 in the first year. No adverse events occurred during the first year of operation; this type of facility could lead to a more efficient use of resources in any children’s unit.
- day assessment unit
- ambulatory paediatrics
Statistics from Altmetric.com
The number of children referred for admission to paediatric units has increased substantially in the last decade.1 2The appropriateness of referral and admission of these children has been called into question.3 4 The use of short stay assessment facilities has been advocated and, in Australia, has been found to have a beneficial effect on patient management.5In this paper we describe our experience of starting a similar unit in the UK, and report an audit of the first year’s operation.
Background
York District Hospital is a district general hospital situated in North Yorkshire serving a childhood population of 45 000 with about 3200 deliveries per annum. It is a single district trust, combining both acute and community paediatric services. In 1994–5, the acute service consisted of two inpatient wards with a total of 44 beds and one short term intensive care bed. These wards were mixed paediatric/surgical wards where both elective and emergency patients were admitted. A small proportion of surgical patients was admitted directly to a separate dedicated day case surgical unit for elective day case surgery. In addition to these two wards, the department also comprised a 15 bedded neonatal unit and a purpose built outpatient department and child development centre where day case investigations took place.
The nurse staffing of the unit consisted of 41.25 whole time equivalents (wte) for the paediatric wards and outpatient department and 21.57 wte for the neonatal unit. The medical staffing for the acute paediatric service consisted of four consultant paediatricians, two middle grade doctors, and five senior house officers.
It was apparent at this time that there were large peaks and troughs in activity, which in part were exacerbated by uncoordinated admission procedures for elective surgical cases because over 20 different consultant surgeons in five different surgical specialties were admitting children electively for surgery. On rare occasions there might be only five or six children on the two inpatient wards while at other times elective admissions were being cancelled because of lack of beds. Further, the department was not meeting fully the Audit Commission’s recommendations that two registered sick children’s nurses (RSCNs) should be on duty at all times on the children’s wards.6
Therefore, a review of the configuration of the paediatric service was undertaken. One of our authors (RAS) had experience of a day assessment unit in Newcastle,7 and so in 1994 a working group was set up to determine the way forward. The objective of this group was to change the inpatient service from two paediatric inpatient wards and an outpatient department where day case investigations were undertaken to a single inpatient children’s ward, a day assessment unit with short stay facilities, and a separate outpatient department.
Planning of the day assessment unit
At the outset of the planning process it was felt important to include a member of the surgical team and a general practitioner to represent the primary health care team. We analysed in detail two time frames of historic paediatric activity; July to August 1993 (a quiet period) and January to March 1994 (a busy period). In particular we looked at case mix and diurnal variation of occupancy (fig 1). Several conditions were felt by the medical and nursing staff to be suitable for care on the assessment unit (table 1). From these data an estimate of the number of beds needed on the children’s inpatient ward and the assessment unit was made.

Variation in two hourly inpatient numbers for a busy period 24–30 January 1994 and a quiet period 9–15 August 1993 before the opening of the assessment unit in May 1995.
Medical conditions thought to be treatable on the day assessment unit
It was necessary to even out the peaks and troughs in elective surgical admissions and so a five bed bay was set aside on the children’s inpatient ward solely for the use of elective surgical admissions. Admission to this area was controlled by the waiting list department to ensure maximum usage of the facility. Day case surgery continued on the day case surgical unit.
Operational protocols were developed for admissions to both the inpatient ward and the day assessment unit (these are available from the authors on request) and a period of public consultation was undertaken with the community health council. The new configuration was piloted during a traditionally quieter period in May to August 1995. Towards the end of the pilot period, there was a positive response to the changes in the arrangements on the children’s wards and we opted to continue the pilot into the winter months of 1995–6. The only change made was to increase the number of beds on the inpatient ward from 27 to 30 by the addition of three extra cubicles. This change was made as our historic data suggested that we needed three more cubicles in winter than in summer. We were fortunate at this time to appoint a fifth consultant colleague (RJB) who had an interest in ambulatory paediatrics and he took operational responsibility for the new service. This appointment facilitated the restructuring of the consultants’ timetables so that the new service was consultant led. Finally we agreed with our consultant surgical colleagues that children with head injuries or burns would be cared for by the paediatric service and that any child admitted under the age of 3 years with a surgical problem would be supervised by a consultant paediatrician.
Assessment unit
The unit is open seven days a week from 9 am to 9 pm. It consists of a waiting room/play area for day case children, a bay for acutely ill children with six beds/cots, and three treatment areas. Two treatment areas are separated by folding doors to maintain privacy. Children requiring longer term treatment are transferred to the children’s inpatient ward, but many acute admissions are discharged home directly from the assessment unit itself. In addition there are two cubicles for infants, for potentially infectious patients, or for privacy. A parents’ sitting room is shared with the inpatient ward. Children who clearly need admission, at the time of referral, go directly to the inpatient ward.
Children seen on the assessment unit usually fall into one of the following categories:
-
Acutely ill children seen for assessment before admission, usually referred by their general practitioner or from the accident and emergency department.
-
Children electively admitted for day case investigations, for example investigation of failure to thrive.
-
Children seen on the surgical preadmission programme before elective day case surgery.
-
Children referred by parents who have direct access to the children’s wards, for example brittle asthma, epilepsy, haemophilia, or diabetes.
-
Urgent outpatient referrals that cannot otherwise be seen in the outpatient department.
-
Some ward follow ups who need to be seen before there is an outpatient appointment available.
-
Some nurse follow ups, for example burns’ dressings.
The unit is staffed by 4.5 wte nurses and adjoins the inpatient ward which is staffed by 36.75 wte nurses. Paediatric medical staffing is provided by a senior house officer and a covering middle grade doctor. The duty consultant for the day has no other clinical commitments on the day he is on call, apart from the assessment unit. In the early evening a senior member of the medical staff (usually the consultant on call) undertakes a ward round of all the patients seen so far that day and a decision is made about discharge or transfer to the inpatient children’s ward. Families discharged home are given a contact telephone number should there be further problems once the child has returned home.
Outcome of the first year’s audit
Between June 1994 and May 1995 (the year before the opening of the assessment unit) a total of 3440 children were admitted to the children’s wards (1911 paediatric and 1529 surgical patients). Of these 1650 were emergency paediatric admissions and 875 were emergency surgical admissions. The number of children needing overnight emergency admission were 1489 in paediatrics and 685 in surgery (table 2).
The number of children admitted to the children’s wards during the two study periods
In the subsequent year, June 1995 to May 1996, there were a total of 2072 paediatric admissions, of which 2016 were emergencies. In the same time period there were a total of 1204 surgical admissions, of which 721 were emergency admissions. The number of children requiring overnight emergency admission was 1443 in paediatrics (representing a fall of 46 patients (3%) from the previous year) and 636 in surgery (a fall of 49 (7.2%)).The fall in the emergency surgical admissions is partially accounted for by the fact that 111 children with head injuries were admitted under the care of the paediatricians when previously they would have been under the care of the trauma and orthopaedic surgeons. Overall the number of children admitted overnight as an emergency fell from 2174 in 1994–5 to 2079 in 1995–6 (4.4%) (table 2).
In the same time period the number of emergency admissions increased substantially. In 1994–5, there were 2525 emergency admissions compared with 2737 in 1995–6: an 8.4% rise. This increase in emergency admissions was exclusively in paediatrics where the rise was from 1650 in 1994–5 to 2016 in 1995–6, a 22% increase in referral rate. In part, but not wholly, this change is explained by the head injuries and burns being admitted under the paediatric specialty instead of a surgical specialty. Of those children admitted in 1995–6 as an emergency, 658 were not admitted overnight but discharged home the same day.
Midnight occupancy also showed a marked change for the two periods. In 1994–5 midnight occupancy for all patients was 5711, falling to 4498 in 1995–6, a fall of 21.2%. This change was seen in both paediatric (3115 in 1994–5 and 2563 in 1995–6, a fall of 17.7%) and surgical specialties (2596 in 1994–5 and 1935 in 1995–6, a fall of 25.4%). A month by month study of midnight occupancy shows that this change occurred as soon as the assessment unit was opened and continued throughout the year for all patients (fig 2A) and surgical patients (fig 2C) and for most of the year for paediatric patients (fig 2B).
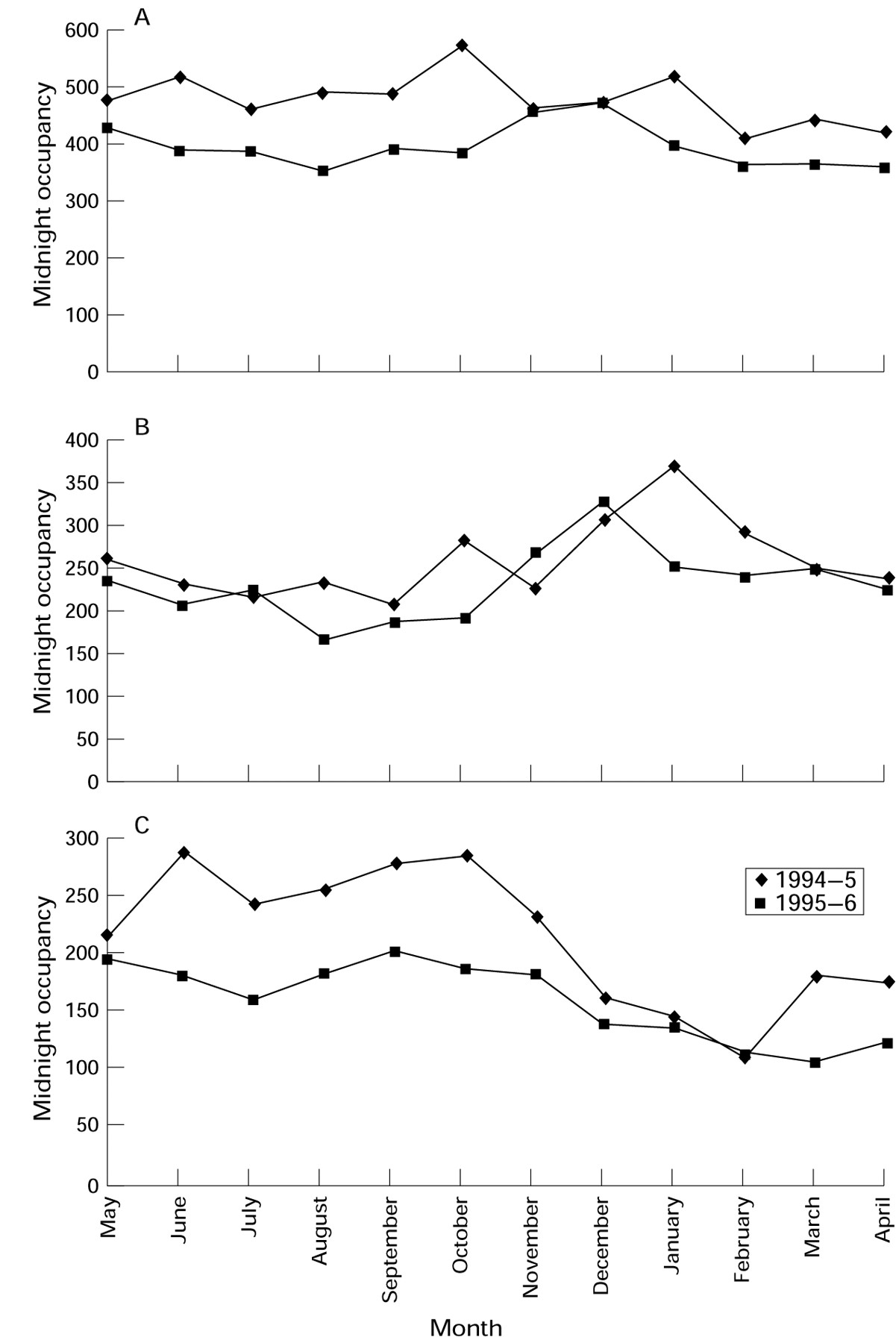
Midnight occupancy for 1994–5 and for 1995–6: for (A) all patients, (B) paediatric patients, and (C) surgical patients according to month of admission.
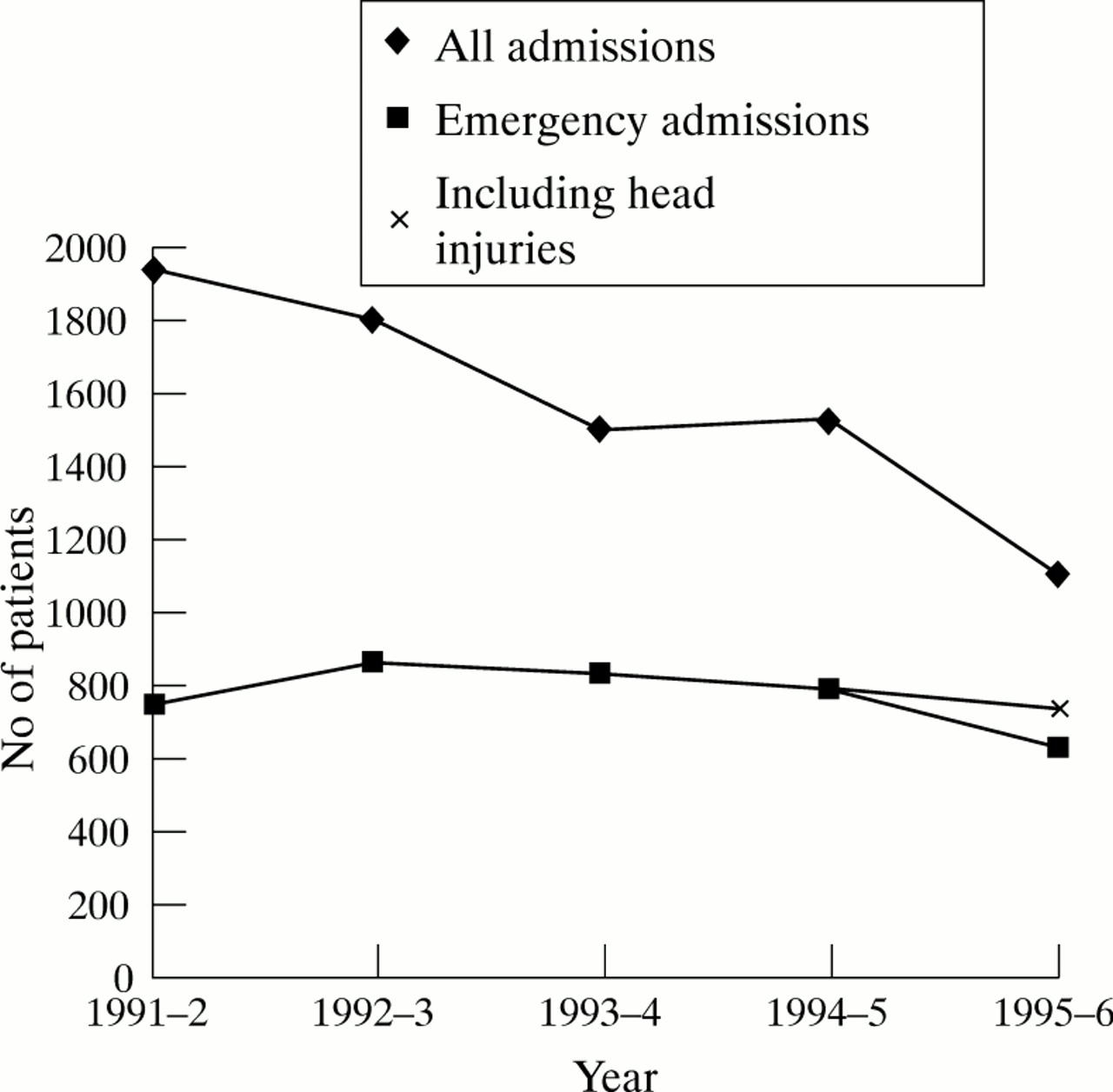
Analysis of the elective day case work reveals that in paediatrics this rose 8.4% from 756 in 1995–5 to 820 in 1995–6. In the surgical specialties the rise was even greater with 601 children seen in 1994–5 and 824 in 1995–6, a change of 37%. The change in surgical elective work is in part explained by better utilisation of the five bedded elective admission bay and also the use of the surgical preadmission programme for ear, nose, and throat and oral surgical patients. It is also explained by a general move towards elective day case surgery. For example, children with a fractured radius and ulna were previously admitted to the children’s ward overnight before manipulation under anaesthetic (MUA) the next day. Now they are treated with a back slab, appropriate analgesia, and discharged home to return the next day to the assessment unit for MUA as a day case. Figure 3 shows this secular trend in admissions since 1991–2 with a consistent fall in non-day case elective surgery while emergency surgical cases have remained constant apart from a fall in 1994–5 to 1995–6 when 111 head injuries were admitted under the paediatricians instead of the surgeons.

The number of non-day case surgical admissions from 1991–2 to 1995–6 for all admissions and for those patients admitted as an emergency.
Another way to look at the effectiveness of the day assessment unit is to analyse the data on those children with zero length of day stays (that is those patients who are admitted to and discharged from a bed on the same day). These data are shown in table 3. The number of surgical patients with zero length of day stay fell from 319 in 1994–5 to 265 in 1995–6 but rose in paediatrics from 498 in 1994–5 to 734 in 1995–6.
Number of patients with zero length of stay in 1994–5 and 1995–6 according to specialty
Not surprisingly, as a result of the changes in admission policy, the average length of stay on the inpatient wards has increased from 1.7 to 1.9 days in paediatrics and 1.5 to 1.7 days in surgery.
A measure of the efficiency of the ward changes can be gauged by their effect on the expenditure figures for the staffing costs of the children’s wards. These figures are expressed at September 1996 pay and price levels. In 1994–5 the staffing costs were £680 192. In the next year this fell to £648 063 (a saving of £32 028) and the projected costs for the current financial year 1996–7 are £642 062 (a further saving of £6001). These financial savings (£70 158 in the two years that the unit has been open) have been achieved despite an increase in the emergency admissions of 8.4%.
An alternative way of looking at the success of the assessment unit is to examine sickness rates of nursing staff, there being a close link between sickness rates of staff and staff morale. These have also fallen from 2.9% in 1994–5 to 2.4% in 1995–6, a reduction of 17%.
An analysis of the work undertaken during the first year of opening of the assessment unit is shown in table 4. There were 1731 emergency admissions of which 1073 were transferred to the inpatient ward for overnight care; the diagnosis at the time of transfer is shown. There were also 1289 elective admissions comprising 765 day cases, 236 children on the preadmission programme for surgery, 129 outpatients, and 159 ward attendees.
Emergency admissions to day assessment unit 1995–6 (for elective admissions see text)
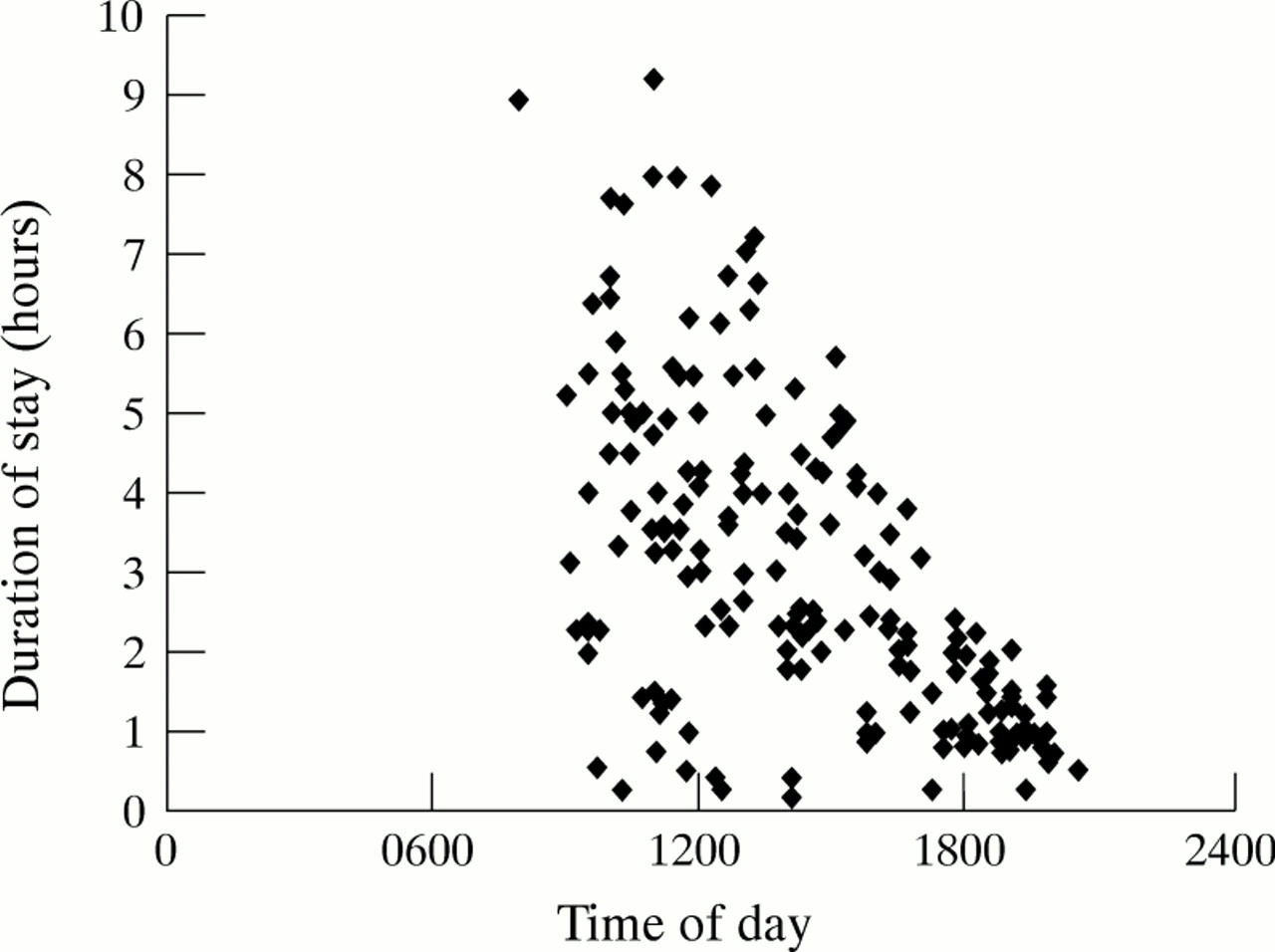
Figure 4 plots the duration of stay on the day assessment unit against the time of admission to the unit (for clarity only data on the first 200 emergency admissions are shown). As can be seen, those children seen earlier in the day had a longer duration of stay. The data are skewed towards the shorter length of stay and the median duration of stay for all the emergency admissions during the first year of operation was 2.5 hours.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
A scatter plot of the length of stay of emergency admissions plotted against time of admission to the assessment unit.
At the outset of the study, we were concerned that there might have been insufficient beds for the winter bronchiolitis season. However in the winter of 1995–6, no patient was refused admission because of the unavailability of paediatric beds and no elective surgical cases were cancelled as a result of medical paediatric patients occupying surgical beds.
Finally, the attendance and readmission rates were audited. All paediatric patients having a second or more visit to the assessment or inpatient ward within 28 days of their first attendance or discharge during the first six months of opening the assessment unit were identified. Elective reattendance, and those children with a diagnosis likely to result in unplanned readmission, for example haemophilia, were excluded. The case notes of the remaining 11 children reattending because of non-resolution of their problems were examined; of these seven did not require admission and their problem resolved, and four children required admission at a second or subsequent visit. These comprised two children with bronchiolitis initially seen early in the course of their illness, one child with a febrile convulsion who became febrile again after discharge from the assessment unit, and one child whose infective exacerbation of eczema was initially not recognised.
Discussion
The use of a short stay assessment unit is a relatively new concept in the care of children in the UK. Beattie and Moir described their experience of a short stay accident and emergency facility in 1993.8 However all their patients were over the age of 1 year and a large proportion of their cases were children with surgical trauma. In a study from West Yorkshire nearly 20% of admissions to an acute paediatric ward were deemed retrospectively to be ‘inappropriate’.3 This accords with the Canadian experience where 24% of patients seen were deemed to be inappropriate admissions.9 Our experience is similar in that 38% of children referred as an emergency were discharged without admission to the inpatient wards.
We have been able to show that in the first year of operation despite an overall increase in emergency admissions of 8.4%, 658 children were assessed and discharged home without an overnight stay. The benefits to these families are great in that home life is less disrupted, alternative child care arrangements are not necessary for siblings, less parental time is lost from work, and the emotional trauma to the child of being admitted is avoided. The fact that the readmission rate from the assessment unit was so low would suggest that the assessment was appropriate and that children were not discharged home incorrectly.
The benefits to the trust are such that we have been able to roster the nursing staff in a more efficient way. We now have on average 3.02 wte RSCNs on duty on the children’s inpatient ward and at least 1.0 wte RSCNs on the adjacent assessment unit whereas previously we had difficulty fulfilling the Audit Commission recommendations on nurse staffing. Night time staffing has also been easier as now only one ward is opened throughout the night as the day assessment unit closes at 9 pm. Sick leave on the unit among the nurses has fallen and is one of the lowest in the trust. As a result the use of bank nurses, with the concomitant costs, has fallen greatly. Crucial in the above has been the leadership of the nurse specialist children’s services manager (GMD) without whose vision and hard work the changes would not have been possible.
There have been difficulties which have been less easy to resolve: managing a 30 bed ward is difficult, and organising ward rounds on a ward where over 30 consultants have admission rights is not easy. At times, when the ward is very busy, it seems that the excellent quality of care has been in danger of being compromised because of the high throughput of patients; the introduction of team nursing has helped in this respect. Bedside teaching of students and junior doctors has also been more difficult as the needs of the inpatient wards require that children are seen and discharged as soon as the child is better. The final area of difficulty has been the elective surgical admission bay where firmness has been necessary to avoid abuse of written admission protocols.
Our experience of the assessment unit has been predominantly a positive one. The one year pilot project is complete and the new configuration of the children’s service will continue. We envisage further developments in our practice, particularly in the area of home care. As far as the assessment unit is concerned we would like to see the commencement of a same day outpatient service. Contracting issues with our purchasers need to be resolved if this new service is to evolve. Key to this is the type of patient who is sent as an emergency admission but who in reality is an urgent outpatient. To date the assessment unit has not altered our outpatient referral rate but we continue to monitor this closely to ensure that the mode/type of referral is correct for each patient.
Finally, one of the difficulties that we encountered in analysing our data was that the NHS data set does not have an adequate means of describing the emergency referrals to the assessment unit. The current definitions do not allow a differentiation between children who are referred as an emergency and discharged home on the same day and those who require an overnight stay. They are all emergency admissions, though the consequences for the child, the family, and the wards are completely different. For this reason we have tried to differentiate between those emergency admissions that required day time care only and those that need an overnight stay.
Similarly, looking at zero length of stay data does not adequately differentiate children seen during ‘normal working hours’ and those admitted at 00:10 am and discharged home the next morning after a stay of only 10 or 12 hours. Once again, the consequences for the family and child in the two scenarios are completely different. It is important when analysing data to understand the definition of a data set. We would recommend a new definition that adequately describes the emergency admission to an assessment unit that does not require an overnight stay. Without such a definition it is very difficult to capture correctly the workload of assessment units and record their activity. This problem of defining cases has made difficult the comparisons between retrospective data collected before May 1995 and prospective data collected subsequently. However, we are confident in our conclusions in that three different data sets (emergency admissions requiring overnight stay, midnight occupancy, and zero length of stay) have shown that an assessment unit allows children to be seen and discharged home appropriately without overnight admission to hospital.
Conclusions
We believe that the assessment unit has had a significantly beneficial impact on paediatric practice in York. In the first year of operation, despite an increases in the emergency referral rate, we have assessed and discharged home 658 children most of whom would previously have been admitted to the inpatient ward. We believe that this type of unit could be adapted with benefit to many hospitals.
References
Commentary
Children should be admitted to hospital only if the care they require cannot be as well provided at home, in a day clinic, or on a day basis in hospital.1-1 When an inpatient stay is essential it should be achieved easily and speedily and be as short as possible. Assessment of acutely ill children may require hospital facilities, especially in infants, though for some this may take only a couple of hours. However, conventional hospital arrangements often lead to an overnight stay. This paper reports experience of a short stay acute illness assessment facility. Overnight stays were reduced from 78% of paediatric admissions before the unit was established to 69% afterwards and significant numbers were discharged within two hours. The authors report a slight overall rise in paediatric admissions but this partly resulted from transfer of children with head injuries from surgical to paediatric care (a desirable change of policy). The proportion of emergency paediatric admissions rose from 86 to 97% while for surgery this was virtually unchanged at 57 to 59%. More opportunity exists for change to day case provision for surgical care but Beverley et al show that when services adapt to the requirements of children it is also possible to effect a change in paediatric emergency admissions.
Short stay assessment should be available for 24 hours a day. National data indicate that half of all paediatric emergencies are now discharged within one day,1-2 and thus the majority of paediatric units provide such a service, though in an unstructured way. Beverley et al emphasise the disadvantages arising from an overnight stay, such as disruption to home life and emotional trauma to the child. However, we also need to consider the advantages that might accrue for a family from an overnight stay. Mothers may find it reassuring, particularly in a small infant who appears ill to them (R MacFaul et al, unpublished), even though hospital involvement in an illness may create future dependency on this service.1-3 Emotional trauma resulting from a short hospital stay is likely to be minimal, even if it involves an overnight period, provided the child is accompanied throughout by a parent. Short admissions have never been shown to have long lasting effects, even in the days when they were longer and parental access limited.1-4 1-5 Much of the upset for infants and children results from the irritating, albeit necessary, restraints involved in investigations such as radiography or the discomfort (minimisable by local anaesthetic creams) of venepuncture or lumbar puncture. However, these interventions also occur during episodes without overnight stay. Close involvement of a parent or carer and a sensitive approach by nursing and medical staff is likely to ease substantially these acute stresses.
Meates and others have described similar arrangements that also include urgent outpatient appointments,1-6 the latter differing by virtue of the extent to which acute assessment needs ‘inpatient facilities’. Acute evaluation includes a period of observation by children’s nurses and senior paediatricians, often using monitoring, for example for oxygen saturation, and investigations with a requirement for rapid results (that is, within a couple of hours) from imaging or laboratory tests, and immediate availability of equipment and staff (anaesthetists) for advanced life support. An appraisal is made of history, examination, measurement, and overall health and caregiver support framework. Case notes with (expensive) height and weight charts will be used with clerical and records activity. All who work on children’s wards know how consuming of staff time the obtaining of urine or blood samples can be. Sometimes quite expensive investigations are carried out, for example lumbar puncture or computed tomography. Thus, while outpatient arrangements can be provided in community settings away from a hospital, urgent acute paediatric assessment cannot.
Meates does not show a reduction in admissions (partly because of difficulties in data analysis), though a smaller proportion of attendances were admitted.1-6 Carter commenting,1-7 reports a reduction in overnight stay in Leicester. Provision of this type of service must be based principally on quality grounds rather than cost containment, especially when teams of home care children’s nurses are established 24 hours a day as by described by Cramp.1-8
ADMISSION OR DAY CASE?
Beverley et al recommend a new NHS definition for the work they describe. This may be desirable but there are counter arguments. Rather, we should be content to show that paediatric admissions can be as short as a couple of hours if services are arranged as described. Such a service is intensive and likely to be quite costly in staff resources and there may be disadvantage in not recognising the episode as an admission (which can extend into the home) even if it appears that admissions continue to rise. Some units continue to classify these children as day cases, urgent outpatients, or ward attenders but in doing so run the risk that the work carried out is undervalued, and possibly under resourced. What is done, even over a period of a few hours, equates to the work and, therefore, the expense of an admission. It is incorrect to use the term ‘emergency day case’ as within the rules of NHS guidance, a day case must be elective. It is important that those interpreting paediatric data do not erroneously record as a day case a child admitted and discharged on the same date. The nature of staff interventions and resource use are not closely comparable with outpatient practice or costs. The same clinical problem presenting in the morning and discharged within a few hours becomes an overnight stay when seen in the late evening. We should not be too concerned to avoid a longer period of stay if there is any risk to the child or if parental anxieties can be allayed thereby.
Advantage should be taken of current data collections within the NHS to quantify the work correctly and so argue for resources such as community children’s nurses or easily accessible paediatric follow up clinics, to provide a service demanded by families and primary care teams. At the same time we should refine our criteria for specialist intervention in acute childhood illnesses and audit our performance to ensure that it is appropriate and consistent with our aspirations to minimise risk to children in the furtherance of their optimal health.