Article Text

Abstract
A case is described of a child of 2.6 years who developed total deafness after acute bacterial meningitis. Rapid obliteration of the cochleas due to osteoneogenesis led to limited cochlear implantation. The case is made for fast tracking these children to cochlear implant teams before neo-ossification becomes established.
- meningitis
- deafness
- cochlear implantation.
Statistics from Altmetric.com
Case report
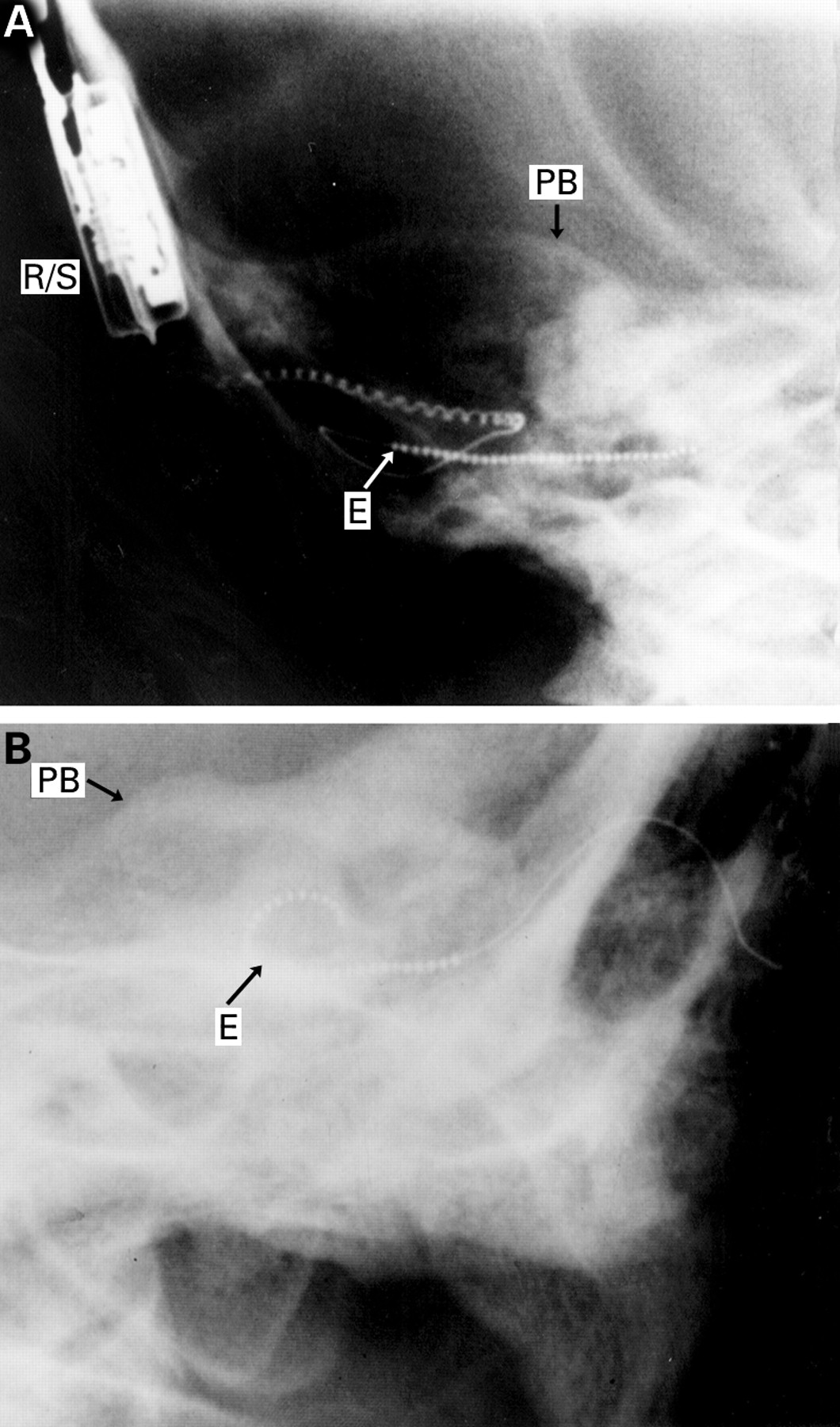
A child aged 2.6 years was referred for audiological assessment after Streptococcus pneumoniae meningitis. Neurological complications had included a right ptosis, left lower motor facial palsy, and pyramidal signs of the right arm and leg. Audiological assessment was carried out six weeks after discharge and indicated a profound hearing loss. This was confirmed by auditory brainstem response (ABR) assessment two weeks later. Referral to the cochlear implant team was made eight weeks after discharge. Hearing aids were fitted 11 weeks after discharge. Computed tomography was carried out and this showed almost complete obliteration of the left cochlear lumen by new bone formation with a marked but lesser degree of obliteration on the right side. Urgent cochlear implantation was recommended. Cochlear implantation, using a Nucleus 22 channel intracochlear device was carried out seven months after the onset of meningitis. Widespread ossification of the scala tympani was encountered and it proved possible to insert no more than eight out of the 22 electrodes (fig 1A and B). The next month the eight active channels were programmed and tuned to create a so called MAP. Initial results indicate that the child is responding across a wide frequency range.
{kind=link}
(A) Partial insertion of Nucleus 22 channel cochlear implant. (B) Full insertion of similar device showing position in basal and middle turns of cochlea (E = electrode; PB = upper surface petrous bone; R/S = receiver/stimulator).
Discussion
This case is important because it highlights a number of issues regarding the identification and treatment of profound deafness in children after meningitis.
Meningitis is the commonest identifiable cause of acquired profound deafness in both adults and children. Up to 10% of children who suffer acute bacterial meningitis will sustain some degree of permanent unilateral or bilateral deafness.1 2 The site is almost always cochlear with loss of the organ of Corti and not the auditory nerve as has previously been stated. The survival of the cochlear nerve therefore allows the possibility of cochlear implantation. Infection in the subarachnoid space reaches the cochlea by two possible routes. The cochlear aqueduct is one possible channel. This leads from the subarachnoid space of the posterior cranial fossa, just below the opening of the internal auditory meatus, through the petrous temporal bone, to the scala tympani of the basal turn of the cochlea adjacent to the round window membrane. It usually obliterates in early life but may remain patent into adult life. Alternatively infection may enter the cochlea through the lateral end of the internal auditory meatus either through canaliculi for the cochlear nerve fibres or through a direct dehiscence in the case of certain congenital anomalies. It is likely that if the infection is going to reach the cochlea it will do so early in the course of the meningitis. The infective process in the cochlea may produce a reaction in the endosteum of the cochlea with a resultant overgrowth of new bone, the process of cochlear osteoneogenesis. When confined to the region of the round window this may present little obstacle to the insertion of a cochlear implant. If osteoneogenesis is widespread implantation may be impossible or limited as in this case report.
In order to identify children with meningitis who become deaf it is recommended that all children at risk have a reliable assessment of their hearing by whatever means may be appropriate to their ages.3 Referral for a hearing assessment should be an essential part of the treatment protocol for all such children and should be performed 2–4 weeks after discharge to allow any middle ear deafness to resolve. The availability of authoritative audiological assessment by paediatric audiology teams trained in the evaluation of very young children and in the performance and interpretation of objective tests of hearing such as ABR is a prerequisite if the service is to be effective. Delay in referral to such specialist teams is often attributable to the practice of repeated testing over time because of uncertainty as to the reliability of results obtained. If profound deafness is present high quality, high definition computed tomography of the cochleas is mandatory and should be interpreted by a clinician accustomed to viewing such images. Computed tomography underestimates the extent of obliteration because early in its evolution the new bone is relatively radiolucent compared with the dense bone of the otic capsule. A partially obliterated lumen can thus appear to be patent. Magnetic resonance imaging with its ability to differentiate between bone and the normal cochlear fluids promises to resolve this problem. If there is a suggestion of new bone formation in the cochlear lumen, the child should be fast tracked to the nearest paediatric cochlear implant centre for early evaluation for implantation. It is the observation of the authors that paediatricians do not realise just how rapidly the process of neo-ossification may occur. Trials with hearing aids should be abandoned when it is obvious that this process is occurring as valuable time may be lost.