Article Text

Abstract
Objectives To establish the incidence of childhood coeliac disease (CD) in Scotland between 1 September 2009 and 31 August 2010, to determine clinical features at presentation and reasons for diagnosis, and to identify any differences in incidence and practice between regions.
Design Prospective data collection through the Scottish Paediatric Surveillance Unit (SPSU). Strategic contacts in each tertiary gastrointestinal region (East, West and North) were emailed monthly to report new cases of CD (<16 years). A clinical questionnaire was completed for each case. Additionally, regional laboratories were asked to report the number of diagnostic antibody tests for CD performed over the year.
Setting This national study looked at the total cases within Scotland. Scotland has a population of 5.2 million, with the mid-year estimate in 2009 of 912 144 children under the age of 16.
Results 91 new cases were reported, giving an overall adjusted incidence of 10.0/100 000/year. Incidence in the East was 16.3/100 000/year, West 8.1/100 000/year and North 7.7/100 000/year. Cases diagnosed due to active screening in the East (4.6/100 000/year) were more than twice the number observed in the West (2.0/100 000/year) and North (1.3/100 000/year), as was the incidence of classic cases. The most frequent symptoms reported were abdominal pain (50/91; 54.9%), failure to thrive (29/91; 31.9%), fatigue (29/91; 31.9%), diarrhoea (27/91; 29.7%) and bloating (19/91; 20.9%). Twenty-two children (24.2%) were diagnosed due to active screening, of which 14 had associated type 1 diabetes mellitus, one Down syndrome and seven had family history. Fifty-five per cent (12/22) of the patients diagnosed through active screening were asymptomatic. Significantly more CD diagnostic antibody tests were performed per head of population in the East compared with the West (OR 1.65, 95% CI 1.57 to 1.73) and North (OR 1.81, 95% CI 1.70 to 1.92).
Conclusions Approximately double the incidence of paediatric CD was observed in the East of Scotland. Evidence of more actively screened cases diagnosed and more antibody tests performed in the region suggests a lower threshold to test. An environmental influence cannot be dismissed since more classic cases were also captured. Further research is needed to highlight the role of any exogenous factors.
- Epidemiology
- Gastroenterology
- Paediatric Practice
- Data Collection
Statistics from Altmetric.com
What is already known on this topic
-
Just two countries to date have national data on ‘real world’ incidence rates of paediatric coeliac disease, but UK data are unavailable.
-
Sweden has demonstrated regional variation in case ascertainment nationally, although similar variation was not observed in the Netherlands.
-
Increased detection of coeliac disease in recent years is assumed to be due to improved education, awareness and active screening of ‘at risk’ groups.
What this study adds
-
The yearly incidence of paediatric coeliac disease in Scotland is higher than that previously recorded in smaller Scottish retrospective studies.
-
Significant geographical differences exist, even within a genetically stable population, and may relate to the threshold to test—a proxy for awareness?
-
Additional exogenous factors may partly explain the variation observed, highlighting the need for a national longitudinal prospective study from birth.
Introduction
Background and rationale
To date, only Sweden and the Netherlands have observed the incidence of paediatric coeliac disease (CD) at a national level. Researchers in the Netherlands have collected data prospectively since 1993 through the Dutch Paediatric Surveillance Unit (DPSU).1 ,2 Incidence rates per 1000 live births (<14 years) ranged from 0.55 in 1993 to 1.10 in 2001. The incidence within each Dutch province was similar and stable throughout the period 1993–1994. Sweden detected higher incidence rates of paediatric CD (<15 years) in the West and in Smaland and Islands compared with North, Middle Sweden and Stockholm between 1998 and 2003.3 This difference could not be explained by differences in gender, age or calendar year. The authors proposed that it did not reflect variation in case ascertainment or reporting as data from a corresponding screening study also reported North to South discrepancy.4 They concluded that geographical disparity was likely to lie in genetic distinction as well as environmental factors, including dietary patterns.
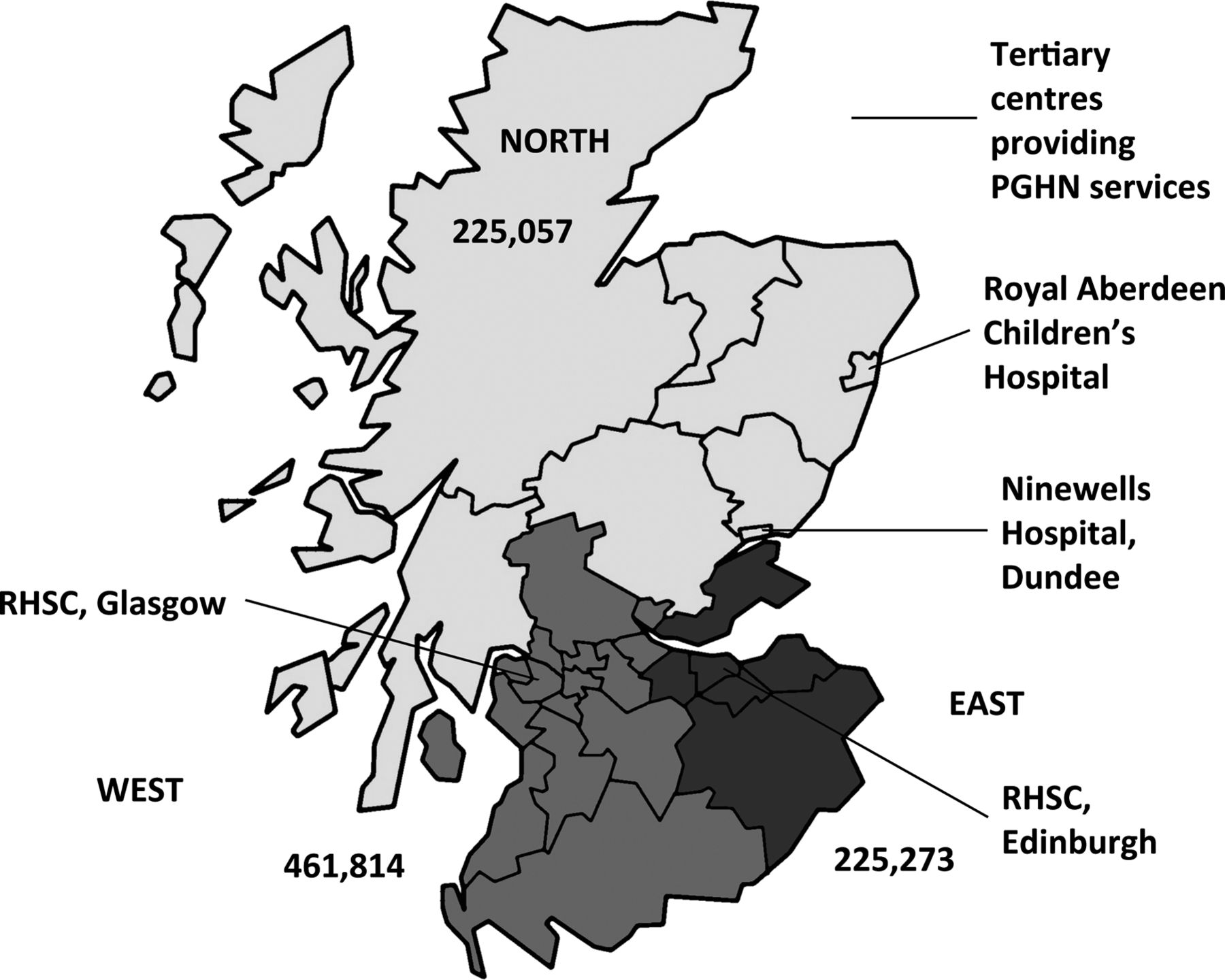
Results of a serological screening study in Southwest England suggests ∼1% of children in the UK are positive for CD.5 The pan-Scottish incidence of childhood CD has never been established; however regional studies suggest countrywide differences in incidence may be evident. The under 16 population in the West region was 461 814, East 225 273 and North 225 057 from the General Register Office for Scotland 2001 census data, which we used for statistical analyses in this study.6 One hundred and twelve new cases of CD (<16 years) were diagnosed in a tertiary care centre (TCC) in the West of Scotland between 1995 and 2008,7 whereas 141 children (<16 years) were diagnosed in a TCC covering the East of Scotland from 1990 to 2004.8 Although an extra year was observed in the East, and slightly different time periods were studied, the TCC in the West covers an area approximately double the population density (figure 1), implying regional variation in incidence and a consistently greater diagnostic rate in the East region per head of population. Previous data from the East demonstrated an average yearly incidence rate of 6.27/100 000/year between 2000 and 2004 compared with 2.38/100 000/year recorded in the West between 2002 and 2008.7 ,8
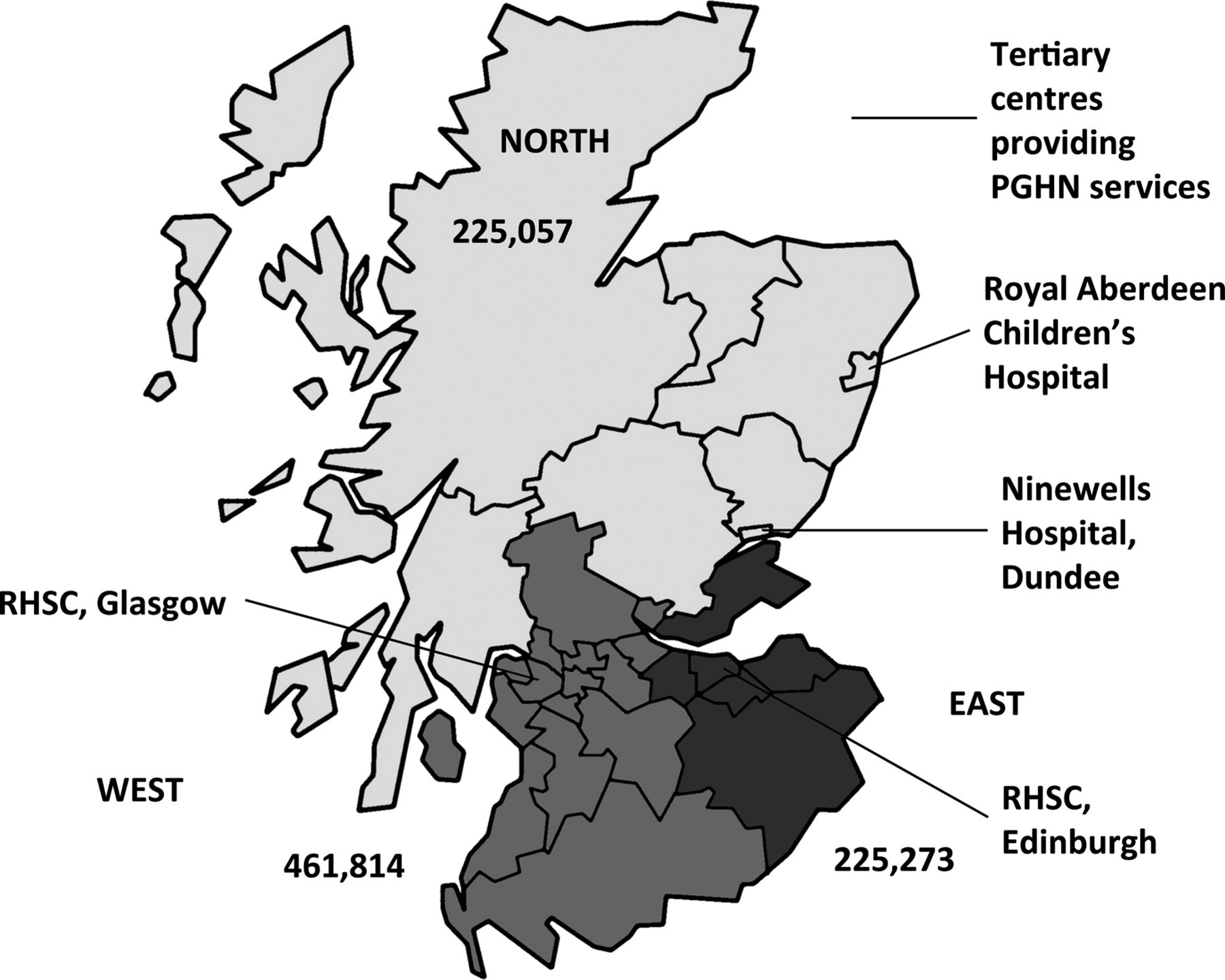
Tertiary centres for paediatric gastroenterology, hepatology and nutrition (PGHN) in Scotland. The Royal Aberdeen Children's Hospital and Ninewells Hospital in Dundee provide services in the North, The Royal Hospital for Sick Children (RHSC), Edinburgh provides services in the Southeast, and RHSC, Glasgow provides services in the West. The numbers within each area represent the total paediatric population under 16 years within the region (2009 mid-year estimates).
Establishing a prospective national incidence register in Scotland is timely. A new guideline (National Institute for Health and Clinical Excellence (NICE) Clinical Guideline 86) on the recognition and assessment of CD was accessible to clinicians practicing in primary and secondary care in Scotland from 2009,9 prompting us to look at current incidence, presentation and who was testing (primary or secondary care), and to see whether differences in CD case ascertainment or practice exist.
Objective
The aims were to determine the current diagnosed incidence of childhood CD in Scotland, to identify case presentation and reasons for diagnosis, and to identify any differences in case ascertainment and practice between regional networks.
Methods
Scottish paediatric gastroenterology services are divided between three regional networks (East, West and North) and are managed through a regional TCC (figure 1). Key Scottish Paediatric Society (SPS) members were identified within each TCC and surrounding regional outreach centres. These strategic contacts were added to a Scottish Paediatric Surveillance Unit (SPSU) emailing database.
A questionnaire was developed in consultation with SPS members to gather routine clinical data on newly diagnosed children. Information collected included demographic characteristics, age, presenting symptoms, other medical conditions, family history of CD, whether the child had been actively screened (due to presentation of an associated condition or family history of CD in a first-degree relative), investigations at presentation (including tissue transglutaminase (tTG) and endomysial antibody (EmA)) and endoscopic confirmation.
Data collection was achieved through an e-reporting system set up by the SPSU, and replicates similar methods used by the DPSU in capturing incidence of CD in the Netherlands.2 From 1 September 2009 an automated monthly email was sent to SPS members in the SPSU database which asked whether they had diagnosed any children <16 years with CD in the preceding month. If after 2 weeks a reply was not received, a reminder e-mail was sent to prompt a response. A positive response from SPS members generated an email to the Principal Investigator and the questionnaire was automatically forwarded to them for completion. Contacts were given a month to familiarise themselves with the process before the start of data collection.
Results were cross-checked with SPS members after a full year of data collection to make certain all new coeliac cases had been forwarded to the SPSU database. Furthermore, regional laboratories were asked to provide information on the number of paediatric CD tests requested from primary and secondary care to identify any differences in serological testing.
NHS Ethics approved the study as a service evaluation audit and no patient identifiable information was collected.
Population
All new childhood cases of CD (<16 years) diagnosed in Scotland between 1 September 2009 and 31 August 2010 were included in the study. Patients were excluded if they did not have a biopsy to confirm diagnosis to meet the prevailing 1990 European Society for Paediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN) criteria.10
Statistical analysis
To control for variation in age and sex ratios between regions, yearly incidence rates were standardised to the 2001 Scottish Census population using the direct method in the epitools package in R V.2.9.2 (R Foundation for Statistical Computing, Vienna, Austria).6 ,11 Children were split into three age groups: pre-school (0–5 years), primary school (6–10 years) and secondary school (11–15 years) to enable standardisation. Rates are presented per 100 000 of the childhood population at-risk (<16 years). χ2 and Kruskal–Wallis tests were performed using SPSS V.17.0 to identify any differences in nominal and continuous variables between tertiary networks.
Results
The SPSU had an 85% response rate (personal communication, Professor Neil McIntosh, SPSU administrator). A total of 110 cases were reported over the year. Fifteen duplicate cases were excluded through identification of sex, age and first part of postcode data. Four cases were excluded as confirmatory biopsies were not performed (1 East; 2 West; 1 North). This left a total of 91 new cases (37 East: 37 West: 17 North). The national age–sex standardised incidence rate was 10.0/100 000/year (95% CI 8.1 to 12.3). The rate was 16.3/100 000/year (95% CI 11.5 to 22.6) in the East, 8.1/100 000/year (95% CI 5.7 to 11.1) in the West and 7.7/100 000/year (95% CI 4.5 to 12.4) in the North (figure 2).

{kind=link}
{kind=link}
Annual age–sex adjusted incidence and 95% CIs of newly diagnosed coeliac disease in children aged under 16 years in each Scottish tertiary gastrointestinal (GI) network (East, West and North) between 1 September 2009 and 31 August 2010.
Gender ratio and age
The overall male to female ratio was 1 : 2 and the median age at presentation was 90 months (IQR 50–129 months); 7.7% (7/91) of all cases were under 2 years of age. There was no significant difference between the three regions with regard to proportion of under 2 year olds diagnosed, age at diagnosis or gender ratio.
Presentation
The most frequent symptoms reported were abdominal pain (50/91; 54.9%), failure to thrive (29/91; 31.9%), fatigue (29/91; 31.9%), diarrhoea (27/91; 29.7%) and bloating (19/91; 20.9%). Cases were categorised into three groups according to primary reason for diagnosis: actively screened (diagnosed due to an ‘at risk’ condition or family history of CD in a first-degree relative); ‘classic’ (presenting with ≥2 gastrointestinal (GI) symptoms); and ‘non-classic’ (presenting with one isolated GI symptom and/or extra-intestinal indicators). Twenty-two children (24.2%) were diagnosed due to active screening, of which 14 had associated type 1 diabetes mellitus (T1DM), one Down syndrome and seven had family history. Fifty-five per cent (12/22) of the patients diagnosed through active screening were asymptomatic. The adjusted rate of actively screened cases was 2.5/100 000/year (95% CI 1.5 to 3.7). Incidence of ‘non-classic’ cases (excluding actively screened cases) was 2.2/100 000/year (95% CI 1.3 to 3.4) and incidence of ‘classic’ CD was 5.4/100 000/year (95% CI 4.0 to 7.2). The incidence of ‘classic’ and actively screened cases was approximately twice as high in the East compared with the West and North (table 1). Excluding actively screened cases, a significantly greater proportion of older children (≥6 years) presented with non-classic symptoms (p=0.02) in contrast to children aged <6 years (table 2).
Annual age-sex adjusted incidence rates (per100 000) of newly diagnosed CD in children aged under 16 years in each Scottish tertiary gastrointestinal network (East, West and North) by primary reason for diagnosis
Differences in the primary reason for CD diagnosis between younger (<6 years) and older (≥6 years) children
Serological testing and biopsy practices
All children either had tTG or EmA serology. Two children (2.2%) were scoped by an adult gastroenterologist; all other children were scoped by either a paediatric gastroenterologist (n=85; 93.4%) or a paediatric surgeon (n=4; 4.4%).
Significantly more CD diagnostic serological tests were performed per head of population in the East (13.19/1000) compared with the West (8.04/1000) (p<0.0001) and North (7.34/1000) (p<0.001) over the year, and in contrast to the North significantly more were performed per head of population in the West (p=0.002) (table 3). Although the proportion of coeliac serological investigations requested from primary and secondary care clinicians in the North could not be confirmed, significantly more tests were requested by general practitioners (GPs) in the East (728/2972) compared with the West (293/3712) (OR 3.79; 95% CI 3.26 to 4.39; p<0.0001).
Differences in the proportion of CD serological tests (tTG/EmA) performed in each tertiary gastrointestinal network (East, West and North) per head of population (<16 years)
Discussion
This first Scottish national study demonstrates an overall childhood incidence of 10.0/100 000/year, with regional figures suggesting a rise in diagnoses. The incidence in the East between 2009 and 2010 was 16.3/100 000/year, whereas previous data collected in the East demonstrated an average yearly incidence rate of 6.27/100 000/year between 2000 and 2004.8 Additionally, compared with the 37 cases of paediatric CD identified in the West in this study, an average of 11 cases per year was recorded between 2002 and 2008 in a retrospective review in that region.7 The Scottish incidence rate cannot be compared to the Netherlands as studies calculated incidence per 1000 live births,1 ,2 however a much higher childhood (<16 years) incidence of 44/100 000/year was reported in Sweden in 2003.12 This elevated rate was attributed partly to unfavourable infant feeding practices between 1986 and 1996, increasing CD susceptibility,4 although additional differences in gene–environment interactions may exist between Scotland and Sweden, and thresholds to test.
Highly sensitive and specific serological screening tests (anti-EmA and tTG)10 will likely have contributed to increased case ascertainment. Both have enabled large population studies in which atypical and asymptomatic presentations have been identified.13 ,14 Recently published NICE Clinical Guideline 86 on recognition and assessment of CD highlights the spectrum of symptoms, associated conditions and family history associated with CD,9 implying clinical suspicion of CD in practice should be at its highest. However, the frequency of childhood cases in Scotland is considerably lower than the 1 in 100 expected prevalence,5 ,15 and suggests we are still failing to diagnose the majority.16 Population screening could uncover cases who may be at increased risk of poor bone health, fertility difficulties and reduced quality of life,17 but the cost effectiveness and its ethical justification is debatable.18
The majority of children were diagnosed endoscopically in a paediatric setting. The male to female ratio in the current study was 1 : 2, in line with most studies.19 Median age at diagnosis (90 months; IQR 50–129) and the percentage of under 2 year olds diagnosed (7.7%) was in keeping with findings of many recent single-centre studies in the UK and abroad.20–24 This is in contrast to an earlier report of paediatric CD (≤15 years) in the Lothian region of Scotland, in which most children diagnosed between 1960 and 1974 were under 2 years of age (∼65%, n=79).25 Many longitudinal studies have shown a steady rise in age at presentation over the last 20 years and with less typical symptoms.2 ,12 ,23 ,26–30 Our work supports these findings, since significantly more older children (≥6 years) were diagnosed with non-classic presentations compared with younger children (<6 years).
Nearly a quarter of cases were diagnosed after active screening (23.1%). In recent years, studies have documented actively screened cases ranging from 6.8% to 33% in paediatric populations.20 ,21 ,23 ,24 ,31 Our results are similar to those of the Welsh study of 1999–2004, in which 22% (n=86) of cases were due to targeting screening and smaller studies in Scotland which have witnessed increased numbers with associated conditions such as T1DM.7 ,8 ,23
We revealed striking differences between Scottish regions. Double the number of cases per head of population were diagnosed in the East (16.3/100 000/year) compared with the West (8.1/100 000/year) and North (7.7/100 000/year). This may be due to under-reporting; however an effective capture/recapture technique was employed to highlight cases that had not initially been forwarded to the register. Importantly, biopsy-proven cases in the East in the years either side of the study (2008–2009, 2010–2011) were similar (n=33 and n=40, respectively) (Royal Hospital for Sick Children, Edinburgh, 2012).
Despite variation in the number of cases, we observed uniformity between regions with regard to age and gender ratios. Interestingly, the incidence of classic cases and those diagnosed through active screening was just over twice as high in the East compared with the West and North. These results indicate that practitioner awareness of at-risk groups in the East may play a role in the greater incidence observed, but does not fully explain the difference in case ascertainment. Prior studies propose differences in genetics or infant feeding may lead to variation in CD prevalence between populations.1 ,12 ,26–28 Although this study does not specifically address these factors, Scotland is genetically very stable; only 1% of the Scottish population have foreign origins.6 Furthermore, a meta-analysis could not determine whether longer breastfeeding or breastfeeding at the time of gluten introduction provides permanent protection against CD or merely delays onset.32
Significantly more serology tests were carried out in the East compared with the North and West per head of population, although it is not certain how many were due to follow-up. Requests from primary care will likely have been for new cases, and in contrast to the West, significantly more tests were requested by GPs in the East (data on the proportion requested from GPs in the North were unavailable).
In summary, this study is the first in the UK to observe a ‘real world’ paediatric CD incidence on a national scale. There is a rise in case ascertainment compared with earlier studies, an older age at presentation and an upsurge in targeted screening. Although uniformity between regional networks was seen in relation to age and gender ratios, there was a stark difference in incidence. Evidence of more screen-detected cases and more serology requested from GPs in the East region suggest that education in primary and secondary care may have played a role. An environmental influence cannot be excluded since more classic cases of CD were also diagnosed in the region. Further research is needed to see whether this trend in incidence continues, and a longitudinal, prospective study is necessary to highlight the role of any exogenous factors, such as infant feeding or childhood infections in the development of CD. The 1990 ESPGHAN criteria required a biopsy for diagnosis: the new ESPGHAN 2012 guidelines allow symptomatic patients with significantly elevated tTG to undergo second-line blood testing to confirm diagnosis. It will be a challenge to ensure that robust diagnosis is maintained or improved through better awareness and is an opportunity to kickstart a long-term national data collection project.
Acknowledgments
We acknowledge the tremendous efforts and help from Neil McIntosh, David Goudie, Vicky Alexander and the other members of the SPS and SSPGHAN who replied to emails and helped recruit patients for the study. We are indebted to Coeliac UK and The Gloag Foundation for funding this work.
References
Footnotes
-
Contributors LW analysed the data and wrote the paper. EB revised the questionnaire and the paper. PMcG, DK and EC reported patients from the three other main centres involved in the study and commented on the paper. PG formulated the SPSU study, wrote the questionnaire, oversaw the e-mail data gathering during the study and revised the paper.
-
Funding Coeliac UK and The Gloag Family Foundation.
-
Competing interests None.
-
Ethics approval NHS Lothian Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.