Article Text

Abstract
AIM To identify features to help paediatricians differentiate between natural and unnatural infant deaths.
METHOD Clinical features of 81 children judged by criminal and family courts to have been killed by their parents were studied. Health and social service records, court documents, and records from meetings with parents, relatives, and social workers were studied.
RESULTS Initially, 42 children had been certified as dying from sudden infant death syndrome (SIDS), and 29 were given another cause of natural death. In 24 families, more than one child died; 58 died before the age of 6 months and most died in the afternoon or evening. Seventy per cent had experienced unexplained illnesses; over half were admitted to hospital within the previous month, and 15 had been discharged within 24 hours of death. The mother, father, or both were responsible for death in 43, five, and two families, respectively. Most homes were disadvantaged—no regular income, receiving income support—and mothers smoked. Half the perpetrators had a history of somatising or factitious disorder. Death was usually by smothering and 43% of children had bruises, petechiae, or blood on the face.
CONCLUSIONS Although certain features are indicative of unnatural infant death, some are also associated with SIDS. Despite the recent reduction in numbers of infants dying suddenly, inadequacies in the assessment of their deaths exist. Until a thorough postmortem examination is combined with evaluation of the history and circumstances of death by an experienced paediatrician, most cases of covert fatal abuse will go undetected. The term SIDS requires revision or abandonment.
-
Covert unnatural deaths are most common in children younger than 8 months
-
The child’s mother is the usual perpetrator
-
Many of the infants killed have had previous unusual illness episodes or recent admission to hospital
-
Infants who die in the afternoon or evening, after recent admission to hospital, or who come from a family in which a previous child has died unexpectedly should raise suspicion
-
Over a third of the infants believed to have been smothered had either petechiae or frank blood about the face, although many do not disclose other significant abnormality at postmortem examination
- child abuse
- unnatural death
- smothering
- sudden infant death syndrome
Statistics from Altmetric.com
Infants who die suddenly and unexpectedly, and in whom a thorough postmortem examination reveals no cause, are placed in the category of sudden infant death syndrome (SIDS). It is recognised that among those infants there are some who have died as a result of direct harm from their parents.1-3 Opinions about the size of that proportion have varied greatly.4-6 The number of infants dying from unidentifiable natural causes has diminished as a result of the following: (1) methods for the prevention of severe illnesses in infancy have improved; (2) parents and doctors now recognise ill infants earlier; and (3) diagnostic tests and postmortem procedures have also improved. Unless unnatural deaths diminish at a similar rate, the proportion of babies categorised as SIDS who have died unnatural deaths will increase and become more important to recognise.
Smothering is thought to be the commonest covert reason for such unnatural sudden infant deaths because, unlike most other forms of physical abuse, fatal smothering can occur without external signs on the face or body, and without incriminating evidence at postmortem examination. Moreover, there have been several studies indicating that smothering of children by parents is not particularly rare—although fortunately most children abused in this way do not die.7-12
This study concerns the clinical features of 81 young children who, although thought initially to have died of natural causes, subsequently were deemed by either criminal or family courts to have been killed by their parents.
The aim was to identify features that might help paediatricians differentiate between natural and unnatural infant deaths.
Methods
The cases were from the past 18 years, and the information was assembled from my contemporaneous notes about the children and their families, which were made when they were encountered. Apart from a small number of local cases, I was involved at the request of medical colleagues, social services, or the police from different areas of the UK. During the same period I was requested to be involved in a larger number of similar cases, but refused involvement because of work commitments. The series of cases reported is not thought to differ qualitatively from other cases notified to me with which I was not involved. During the 18 year period I was involved with over 200 other families in which children were adjudged to have been abused, but in which no child died. At the time of my involvement it was usual for me to see all the documented material including general practitioner, hospital, health visitor, and social service records relating to the child, the siblings, and the parents. In the criminal cases, and one third of the family court cases, information was supplemented by transcripts of police interviews and investigations. In most cases I met separately, and jointly, the child’s mother and father and key social workers and, sometimes, other relatives. For some of the earlier cases, a record had not been kept about every feature and, therefore, there is not reliable information relating to each of the studied features for each of the 81 children, or for each of the 50 families. The number of children, or families, with reliable records is noted in the relevant part of the “Results” section.
The causes of death of the 81 children from 50 families were considered in detail during court proceedings, which concluded that a parent had been responsible for the child’s death (table 1). In 19 families, the case was heard in a criminal court, where a jury delivered its verdict “beyond all reasonable doubt” on the evidence presented to it by the different parties. For 41 families, there were hearings in the family court where a judge, after considering the detailed evidence, gave judgment based on a high degree of probability. (Ten of these cases were also proved in a criminal court, the other 31 were not accompanied by criminal proceedings.) In most cases, the family court proceedings took place because of abuse of a subsequent child (particularly by smothering), or a subsequent child being born to a mother who was found to have had previous infants who had died. In those cases, the task of the family court, in considering the welfare of the subsequent child, was to decide on matters of fact relating to the nature of the deaths of the previous children. In 19 of the 50 families, a parent confessed to harming or killing the child by smothering or choking. The confessions occurred five months to eight years after the deaths, usually in the context of court proceedings.
Proof of parental responsibility for children’s deaths in 50 families
Results
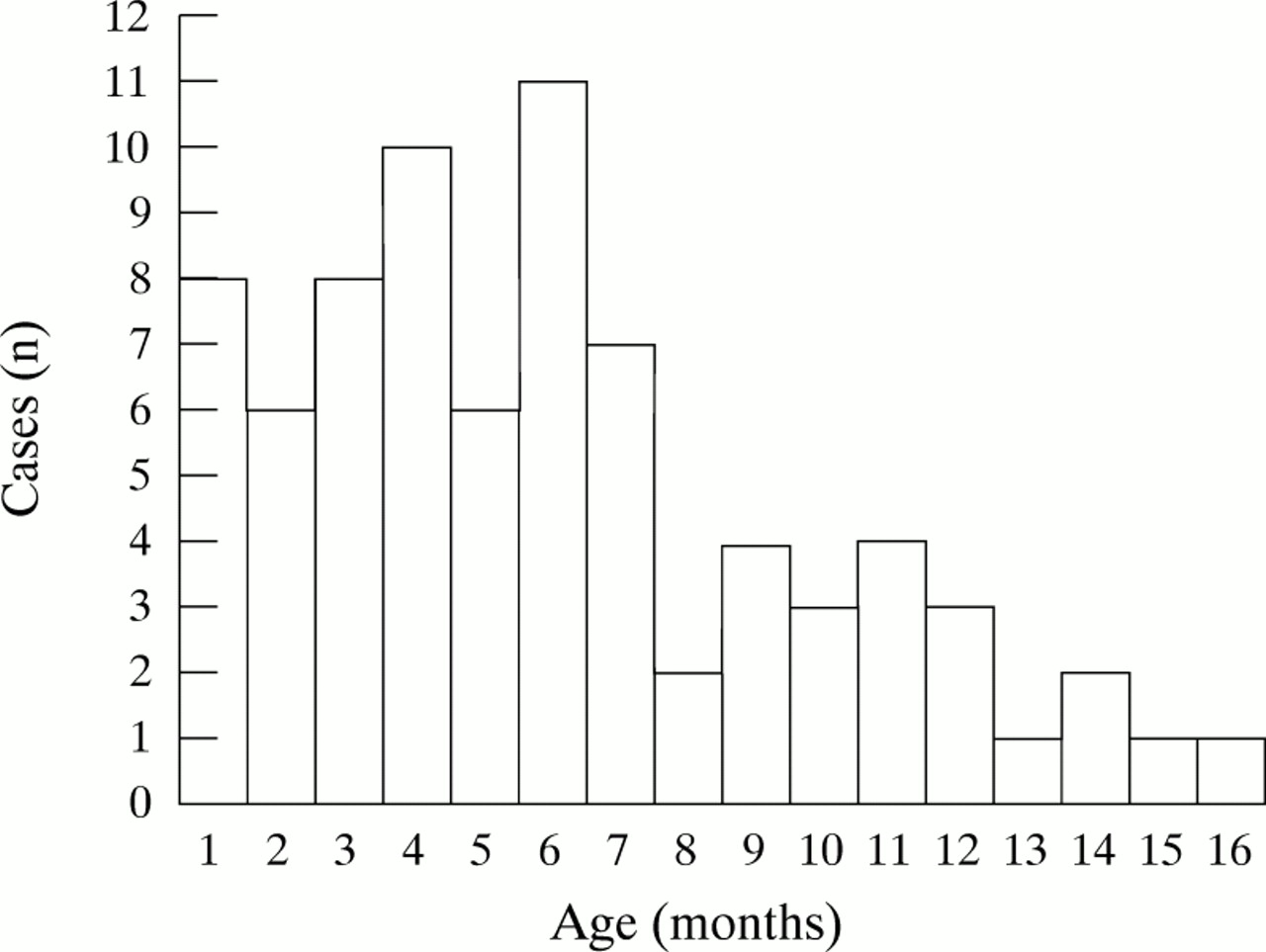
The 81 children came from 50 families. In 24 families in which two or more infants died, the deaths occurred sequentially to successive infants (two deaths in 18 families; three deaths in five families; and four deaths in one family). There were 46 boys and 35 girls. All except one of the children (a step child) were the natural children of the perpetrator. The age at death ranged from 1 week to 16 months and the distribution of ages is shown in fig 1. In addition, there were four older children who had died aged 1½, 2½, 4, and 5½ years who were siblings of younger dead children. Those older children had been believed to have died natural deaths, but were subsequently deemed to have died unnaturally. The four older children are excluded from those parts of the results that deal with the characteristics of infant deaths, although the five children aged 12–15 months are included, because they had been categorised initially as SIDS.

{kind=link}
The age (month of life) at which 77 young children died (those in the one month column were under the age of one month).
BIRTH ORDER (50 PARENTS)
Most of the dead children were born to mothers who had not had a previous live, healthy child. Thus, for 36 parent perpetrators there was no living previous child, and for the 14 parents who had a previous child living, 12 of their 17 previous children, in retrospect, were considered to have been abused.
PERINATAL HISTORY (73 HISTORIES)
Pregnancy
Thirty eight pregnancies were considered to be normal. The other 35 included significant problems, particularly alleged antepartum bleeding and abdominal pains, necessitating admission to hospital.
Gestation
The length of gestation was < 30 weeks for seven babies, between 30 and 36 weeks for 10 babies, and > 36 weeks for 56 babies.
Birth weight
Twenty babies weighed less than 2500 g, 13 weighed 2500–3000 g, and 40 had a Birth weight of > 3000 g.
Neonatal care
Nine infants had major neonatal problems requiring expert management in neonatal intensive care units. One baby had residual respiratory problems attributed to bronchopulmonary dysplasia. The others were considered healthy.
MEDICAL HISTORY
Previous events (75 infants)
Most of the children had had previous unusual or unexplained events reported by the perpetrator. By far the most common reports were of infants stopping breathing, looking blue, appearing dazed, twitching, or fitting. An acute life threatening event was deemed to have happened if the parents’ story of the event was supported by a health professional observing the infant to be collapsed, unrouseable, or breathless, or if on arrival at hospital there was clear biochemical evidence (such as acidosis or high blood glucose) indicative of a recent major stressful event. Forty six children had episodes of apnoea/seizures, of whom 24 had one or more acute life threatening event, and 11 had other unexplained illnesses. Of the rest, three had an acute life threatening event, and nine had another unexplained illness. Seventeen had an unexceptional previous history.
The season of death is shown in table 2, and the time at which the child was found dead or moribund by the carer in table 3. These timings have been used because of similar studies that have been performed on children dying of natural causes,13 but the three time bands disguise what was a very clear predominance of deaths occurring in the afternoon and evening. Fifty five infants were found moribund or dead between 11:00 and 22:00.
Season of death of 77 infants
Time of death of 72 infants
The last occasion before death when the child was seen to be normal, or in near normal health, was recorded for 65 children. The observers and reporters of that time interval were the child’s carers, although in several cases there was confirmatory evidence of the child’s previous wellbeing from relatives or friends and, occasionally, from health visitors or doctors. Fifty five children were observed to be well within two hours of death, five within two to six hours, and five within six to 12 hours of death.
The usual account of events was that the parent would discover the lifeless child, seek help from someone in the house or next door, telephone “999” for the emergency services, and attempt resuscitation. When the paramedical staff arrived they too would attempt cardiopulmonary resuscitation, although intubation would only be performed on arrival at the emergency department of the local hospital. Several of the moribund children made an initial partial response to that resuscitation before dying.
Recent medical examination or hospital admission (77 children)
More than half the children had been examined by doctors in the preceding week and considered to be healthy. These included 43 children who had been patients on children’s wards in the previous four weeks, where they had been examined and considered to be normal by paediatric staff who arranged for their discharge from hospital. The interval between discharge from hospital and death is shown in table4.
Interval between recent hospital admission and death
Nearly half of the children had been discharged from hospital within the preceding week. Most of those had been admitted briefly because of an unusual or unexplained event reported by the carer, but on investigation and observation in hospital had been found to be well. The usual circumstance for the 15 children who had been discharged from hospital within the previous 24 hours was that the child was discharged in the morning, and then died at home that evening.
Other unusual features of these deaths included seven children whose deaths were foreseen by the carer—the parent predicting the day on which the child would die; and another four children who died on the anniversary of a previous siblings death.
EXTERNAL SIGNS AT DEATH (70 CHILDREN)
Twenty seven children were reported to have been found with blood apparent in the mouth, nose, or on the face. In deciding upon the report of bleeding, care was taken to establish that the finding was of frank blood, rather than the common sero-sanguineous froth that can be present in moribund children, particularly when subject to resuscitation. On examination by medical staff, stale blood was seen on 20 of those 27 children. Ten children had either unusual bruises or petechiae, on the face or neck. Forty children had neither bruises, petechiae, nor report/finding of bleeding.
POSTMORTEM EXAMINATION FINDINGS
Information on the postmortem examinations of 77 children was available, but the quality of that information was extremely variable. The postmortem examinations had been performed in different parts of the country by different pathologists, and extended over an 18 year period during which time standards of practice had changed greatly. In many of the earlier cases, tissues had not been examined microscopically by newer histological techniques. A minority of cases underwent detailed neuropathological examination. An effort had been made previously to arrange for re-examination of relevant tissues, but in most cases material was no longer available for re-examination. Therefore, this account is based on the contemporaneous postmortem reports from the relevant pathologist, who was usually the local district hospital pathologist, although in the last five years was more likely to have been a forensic pathologist or paediatric pathologist. In most cases it was the pathologist’s report that led to the decision of the coroner as to the cause of death and the entry on the death certificate. Forty two children were categorised as SIDS or “cardiopulmonary arrest−SIDS”, six as “not ascertainable” (three of whom had been found to have fractures of the skull or arm), and 29 were given a specific cause for natural death (table5).
Specific pathological diagnoses (29 cases)
Unusual features of the 42 infants categorised as SIDS included five “infants” over 12 months of age; two infants who had fractured ribs, which were considered to be the result of resuscitation; two infants under the age of 6 months who had several balls of paper in the stomach, which were deemed to have been screwed up and eaten by the young infant. Twenty eight of the infants had had previous unexplained or unusual events in their recent medical history.
THE PERPETRATORS
For two of the 50 families, the courts could not decide which parent was responsible. For the others, 43 mothers were judged to be the perpetrator and five fathers. All were white European adults. Other features of the perpetrators are described below.
Social class
Using the Registrar General’s classification, one family was graded social class I, one as class II, 10 as class III, 10 as class IV, five as class V, and 20 were unclassifiable. There was a preponderance of families in which there was no regular wage earner. At least 35 were receiving income support.
Maternal smoking habits (69 children)
Fifty nine of the children were born to and cared for by a mother who smoked cigarettes regularly. Ten had mothers who did not smoke.
Although many of the mothers consumed alcoholic drinks, there was nothing to suggest regular overindulgence or addiction to alcohol.
Perpetrators’ health
The health records of 44 perpetrating parents had been studied for evidence of somatisation. Evidence was sought for either somatising disorder or Munchausen syndrome (defined as factitious disorder with predominantly physical signs and symptoms, plus pseudologia fantastica14). Munchausen syndrome was present for 10 parents (seven mothers and three fathers) and somatising disorder was present in another 11 parents (defined as either mild/moderate factitious disorder or somatoform disorders—that is, physical complaints not attributable to medical condition, although not intentionally produced). Twenty three perpetrators had neither somatising disorder nor Munchausen syndrome.
Other features
Unusual features in the lives of the perpetrators included five who had been involved with fire raising (arson), six who had been, or were, involved in litigation against doctors or hospitals, and seven who had sought media publicity in relation to their child’s death.
Discussion
The childhood deaths that were studied were covert unnatural deaths which, at the time of death, had been thought to be the result of natural causes. The series does not include young children who had obvious signs at presentation in hospital, or at postmortem examination, of major traumatic abuse, neglect, or poisoning.
The likelihood that the court verdicts about parental responsibility for death were correct is very high indeed. Even in the family courts, where the judgment is made on the balance of probabilities, all experts, particularly the judge, are aware of the dire implications of the verdict in terms of a parent being allowed to care for a future child.
The circumstances of the deaths, and of the families, were scrutinised carefully before the court hearings. Therefore, in addition to the information presented in this paper, there was usually much additional incriminating evidence, including the recurrence of events and death always with the onset in the presence of one carer, inconsistent and untruthful accounts of the events from the perpetrator, evidence of smothering or other abuse of a subsequent child, and sometimes admissions by the perpetrator. This study addresses certain general features that might be useful to paediatricians who encounter sudden infant death, but in each case the paediatrician must take into account the additional specific features of that individual case.
It is necessary to consider how much the described features are the result of case selection, and how much they are characteristic of all covert unnatural infant deaths.
It is likely that the number of cases occurring in the context of “Munchausen syndrome by proxy” abuse, or which were caused by parents who had Munchausen syndrome themselves is high because of such cases being referred preferentially to me.15-17Similarly, since publishing “Suffocation, recurrent apnoea and sudden infant death” in 1990, many similar cases have been referred to me.
Because the cause of death was proved in court, some of the features will have been used as evidence, to persuade juries and judges to pronounce that a child had been killed unnaturally. These features will be more characteristic of legally proven unnatural infant death than covert unnatural infant death in general. Multiple deaths, previous undiagnosed events, and maternal somatisation are likely to be overrepresented because of that.
In contrast, some of the described features will have been used in court in favour of a natural cause, and the verdict will have been reached despite the fact that those features were advanced in favour of a natural cause (maternal smoking, low birth weight, neonatal problems, and low social class are cited frequently in court as favouring a natural cause).13
Other features, for instance birth order, will not have been considered in court and will not have influenced the verdict.
The reason that more than half the reported families included more than one dead child is likely to be because the courts were impressed by evidence that it was highly improbable for two or more children to die in infancy of undiagnosable natural causes: “if there is a 1/1000 chance of a child dying suddenly and unexpectedly of natural causes in the first year of life, the chance of two children within a family so dying is 1/1 000 000”. A parent who kills only one child is much less likely to be incriminated than one who kills or abuses two or more. Nevertheless, the finding of 26 serial killers is worrying.
Other Australian and English studies confirm that the youngest or only child in the family is most likely to be killed.18Although most of the mothers were young, that was not the only reason for the finding that it was nearly always the first (or the first few) children who were killed. It was rare for the perpetrator to have had a previous child who was well and who had not been abused. This has important implications for those assessing future risk and for parental treatment.
Death was much commoner in the first 7 months of life. Older infants are more robust and more personable. Some of the factors that make it particularly stressful for a young mother to look after a young infant might be less severe after the early months. The moderate excess of boys fits in with previous studies, and with reports of smothering of infants who have not died.10-12 Homicide is more likely in the 1st year than any other year of life.19 Young children are usually killed in the home, and the infant is most likely to be killed by their own parent in their own home.
Nearly all the perpetrators were the child’s mother. This is likely to be a correct conclusion for these sorts of death. Fathers may be responsible for an infant’s death, but previous work suggests they are less likely than mothers to kill children under 1 year of age and they are more likely to kill the child by shaking or by direct physical force, which usually cause signs that are unlikely to be mistaken for a natural death. It is interesting to reflect that the fathers cause death by methods that are more indicative of impetuous violence, whereas the methods used by mothers suggests a clear intent to kill or cause grievous bodily harm.18
Deaths were commonest in disadvantaged families, receiving income support. During the study period, the proportion of adult women smokers in the UK has been in the range 25–30%.20 Most of the perpetrating mothers were regular smokers, and few if any desisted during pregnancy. Both these factors have been cited as risk factors for SIDS, smoking in pregnancy being particularly important.21 22
The perinatal events and early histories of the children are relevant. The pregnancies contained an excess of problems. Part of that excess was due to some mothers who, in retrospect, were considered by the obstetricians to have had factitious obstetric disorder.
About a quarter of the infants were low birth weight, compared with the general UK proportion of 7% (and a proportion of 10–12% in disadvantaged families). About three quarters of the infants had unusual previous medical histories. The story of recurrent episodes of apnoea and seizures is one that has been reported before in children who are smothered, and particularly in those who are incurring Munchausen syndrome by proxy abuse.7 10 12 About half the deaths occurred in what seemed to be the context of Munchausen syndrome by proxy,23 which is a similar proportion to that found for children who survived suffocation in the 1992–94 British Isles survey.11 Some of the other episodes are less easy to understand, but the findings accord with experience of other fatal child abuse in which there has been an excess of preceding unusual medical events or hospital admissions,24 and it is also a finding that has been observed in the UK in babies subsequently labelled as “cot death”.25
Most of the deaths are likely to have been caused by smothering. Many of the preceding histories were typical of smothering. The 19 (of 50) perpetrators who confessed to killing their child described the smothering. One was a mother who had also pushed balls of paper down the infant’s throat because she thought that would choke the child (it did not—the balls of paper went into the stomach). Several of the more recent cases have been the subject of meetings involving all the medical experts of the different parties; and the usual conclusion has been that the mode of death has been smothering. In three cases the neuropathological changes, and the external marks on the body, raised the likelihood of shaking as the cause, or as a contributory factor.
No cases of poisoning were identified. About one third of the cases, mainly the recent ones, had undergone detailed toxicological tests that were negative. The possibility that a few of the earlier deaths were attributable to poisoning cannot be excluded, but the contemporaneous information does not make it likely.
Paediatricians are familiar with the story of natural SIDS death when a previously healthy 4 month old baby is found dead in his cot in the morning as his parents awaken, having seemed normal or merely snuffly the previous evening. Quite often those bereaved parents say they last saw their child to be well eight or 10 hours earlier. These deaths were different. Nearly all the children were seen to be well shortly before they died, and most of them died in the daytime or early evening. This should not be surprising—obviously, when asleep, parents do not kill their children. Moreover, it is likely that many natural deaths occur more slowly, the child becoming gradually iller during the night, unobserved. Nevertheless, near miss cot deaths should always be reviewed carefully: the chance of a parent finding a child dying a natural death a few seconds before stopping breathing is very small. If the parent is on the scene at that time it must raise the possibility that the parent has been responsible for the child not breathing. Natural cot deaths are more likely to be associated with a child being found dead, rather than moribund. Most of the deaths occurred when there was just one parent in the house, although a significant proportion happened when both parents were at home, with one parent being alone with the child for long enough to kill.
Nearly half of the children had had brief admissions to hospital within the preceding week. Fifteen children had been discharged from hospital children’s wards in the last 24 hours. All paediatricians will feel that those infants were discharged inappropriately and too early. It is neither a shortage of hospital beds nor of facilities that causes paediatricians to discharge children so rapidly, it is part of an evolutionary culture which correctly believes home to be a safer and happier place than hospital for most children, and which seeks to admit ever fewer children to hospital for ever shorter periods. But now that the average length of stay in the UK for an acute paediatric admission is under two days, it is time to recognise that too many risks are being taken. If a young child is admitted to hospital as a result of a young, harassed mother from a poor home recounting a startling or unusual event, and the baby is found to be completely normal, it does not mean all is well. When next morning the pathology reports and thex ray reports come back normal, it would be safer to discharge the hospital notes and normal investigation reports out of the door than the baby. That mother has brought the child to hospital for a reason that we have not understood. There is ample evidence that children suffering recurrent physical abuse, as well as Munchausen syndrome by proxy abuse, have many warning signals and previous hospital encounters before the final event that maims or kills.
This study did not include reliable data on the status of the young children in terms of previous entry on the Child Protection Register. A minority are known to have been on Child Protection Registers; most were not. Even though a recent study from North America suggested that screening child protection agency records for previous referrals was an ineffective way of detecting infanticides misdiagnosed as SIDS,26 checking the Child Protection Register is a sensible step when dealing with young infants who present with unusual or recurrent events.
Currently, many paediatric units are failing to heed warning signs and failing to protect some very vulnerable children. Many of the mothers who killed their child in the afternoon/evening, after their being discharged in the morning, had been resident in hospital with their child. One wonders how often a doctor or nurse sat down with that mother before discharge to find out whether she was confident and happy to return home with her infant, or discussed the family with their health visitor or general practitioner.
Because these were cases considered originally to be natural deaths, major external signs would not be expected. The association of bleeding with smothering has been reported before.10 12 It is important, nevertheless, to distinguish between the pinkish brown sero-sanguineous mucus that may be on the face of a dead baby who has been subject to resuscitation, and the bleeding or crusted red blood that may be found after smothering and physical abuse. Although smothering was believed to have been the cause of death for most of the children, neither purpura nor petechial haemorrhages were common. More than half the children had neither bruises, petechiae, nor signs of recent bleeding. The corpse appeared normal. Similarly, fatal smothering might not reveal any specific abnormality during postmortem examination.
The circumstances of the study did not allow the sort of pathological re-evaluation that was needed. Reliance had to be placed on the notes taken from postmortem reports that had been performed by a variety of investigators in different parts of the country, over a long period of time. Those pathologists would have been commissioned by the local coroner who has to be informed of sudden unexpected deaths. That coroner has an assistant, the coroner’s officer, who explores the background to the death. Unless there is something very unusual or suspicious about the circumstances, the coroner invites the local hospital pathologist to do a postmortem examination. That pathologist might not have particular experience of infants and children, and is rarely a paediatric pathologist.
Both the coroner and the pathologist are under pressure to provide a diagnosis fast so that a death certificate can be issued and the body released to the family for burial. Essentially, they are having to provide a quick decision about a natural or unnatural death, and the pathologist has to do that before detailed histological or other test results are available. If the pathologist does not provide a natural cause for the coroner, the coroner has to arrange for a formal inquest, and there is considerable pressure to avoid such events. Inevitably, there is a tendency for all parties to seek a natural cause rather than an unnatural one. It is unusual for either the coroner or the coroner’s officer to have a medical background. If the coroner’s officer has identified obvious suspicious features, the coroner commissions an approved forensic pathologist. Some, but not all, forensic pathologists have considerable experience of infants, but their work will be related to forensic examinations and they are not involved regularly with postmortem examinations of ordinary infant deaths.
The postmortem examination conclusions demonstrate the inadequacies of the past practice. SIDS has been used at times as a pathological diagnosis to evade awkward truths. In this series it was used for infants over the age of 12 months, for infants with fractures, and in bizarre circumstances, such as when coins, balls of paper, and mittens were present in the airways or intestines of the children. Such findings were explained away on the basis that the infant had grasped and eaten the object (even though their developmental age made that impossible). Postmortem examination had revealed unusual foreign bodies in the stomachs of five children, and in the airways of two children. At the time of postmortem examination, these had been considered to be the result of accidental, coincidental ingestion. Yet, those dealing with accidental ingestion know how rare it is for children below the age of 1 year to swallow foreign bodies. Moreover, the chance of such a young child accidentally ingesting a foreign body, and then dying of natural causes within the next four hours while the foreign body is still in the stomach, must be infinitesimally small. The finding of a foreign body in the alimentary canal of an infant who is thought to have died of natural circumstances should arouse considerable suspicion.
Another distressing feature to a paediatrician is the way that some respiratory and cardiac conditions that make children ill were diagnosed on the basis of a few inflammatory cells in the relevant organ, and no account was taken of the history; the problem being that the pathologist probably only had a brief story from the coroner’s officer, and had no adequate previous medical history, and no advice or help from a paediatrician. For the pathologist it was not customary to ask the local paediatrician whether it was feasible for a 3 month baby to pick up a small coin and eat it, or to die from bronchopneumonia half an hour after being observed by two parents to be awake, happy, and in normal health.
There continues to be much interest in the development of more specific tests (such as intra-alveolar haemosiderin)27 that might identify smothering and other forms of child abuse.28 The UK Royal College of Pathologists has issued guidelines on minimum prerequisites for a thorough postmortem examination of infants.29 Despite the considerable resource implications of this thorough assessment and investigation, it is likely that most infants who die suddenly and unexpectedly in the UK are now having that thorough postmortem examination. Nevertheless, unless it is combined with a careful evaluation of the child’s previous history, by an experienced paediatrician, mistakes will continue to be made. The price of those mistakes is high because other siblings born to the perpetrator are at risk. Those countries and USA States that have an experienced “child death review team” are much less likely to make dangerous mistakes, particularly if a death scene investigation is included.30-33 The UK Confidential Enquiry into Still-births and Deaths in Infancy (CESDI) continues to perform useful research and studies of selected issues,34 35 but it is not a substitute for careful multidisciplinary investigation of all unexpected infant deaths.
As the number of infant deaths continues to fall, it becomes feasible to organise a multidisciplinary confidential enquiry into every unexpected infant death. The time for such comprehensive investigation has already arrived. Even though the number of infants categorised as SIDS in the UK has fallen in recent years to below 400/year, it is a national scandal that we accept a situation in which so many young children die of unknown causes. If one out of every thousand 21 year olds died suddenly and unexpectedly without an identifiable cause there would be a national outcry.
It is sad that the term SIDS has become a barrier to the sensible and sensitive investigation of infant deaths. Despite the compassionate and constructive work of so many lay and medical people concerned with SIDS organisations in different countries, the label has become counterproductive. For many of the cases in this series, SIDS deaths were presented to court as if they represented a single disorder, and information given regardless of the fact that nearly all the earlier epidemiological surveys of SIDS will have included many children who died of covert unnatural deaths. Many social workers, and sometimes health professionals, had been misled at case discussions and conferences, and in the assessment of many of these families, because of the way that the label SIDS had been given to a previous child—“We don’t have to worry about that death, it was a natural one, the child died of SIDS”.
If the term SIDS is to continue to be used then it should be limited in the way suggested by the expert panel of the US National Institute of Child Health and Development36 to “the sudden death of an infant under 1 year of age which remains unexplained after a thorough case investigation, including performance of a complete autopsy, examination of the death scene and review of the clinical history”.
However, it would probably be in the best interests of children to abandon the term and acknowledge that when a previously well child dies suddenly, and a thorough assessment and postmortem examination reveals no cause, we say “unexplained” or “undetermined” rather than pretending that it is a natural death from some yet to be identified agent. Nobody doubts that there are many different causes of death for children categorised as SIDS, and yet we continue to use the term as a diagnostic category, and to discuss it as a single disease entity. We should be honest and admit that we do not know and, above all, we should be angry and intent on preventing so many young children dying suddenly and unexpectedly so early in life.
Warning to meta-analysts
Some of the cases reported in this paper will have been included in other papers originating from the UK—notably references 10, 12, and17. It would be unwise to include another UK paper in any meta-analysis alongside this paper, because of the risk of overlap.
Acknowledgments
I am grateful to the many colleagues who have involved me with these families, and who have been generous in supplying additional information for the study. I thank J Darling and D Smith for their thoughtful comments and M Jones for her efficient work with so many drafts.