
Retrospective Investigation of a Lead Poisoning Outbreak from the Consumption of an Ayurvedic Medicine: Durban, South Africa


Abstract
:1. Introduction
2. Methods
3. Results and Discussion
3.1. Profile of the Study Population
3.2. Source and Distribution of the Product
3.3. Diagnosis
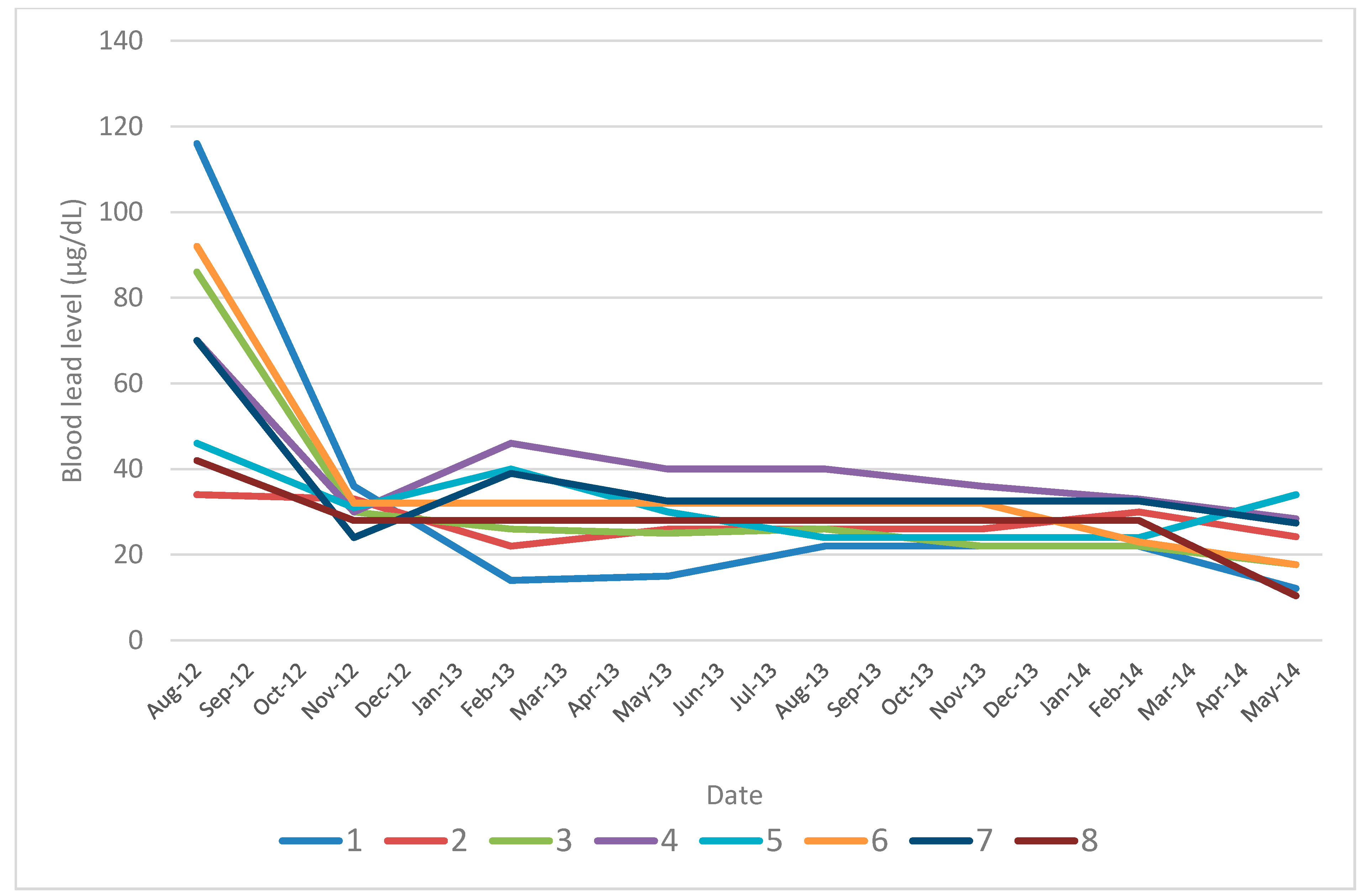
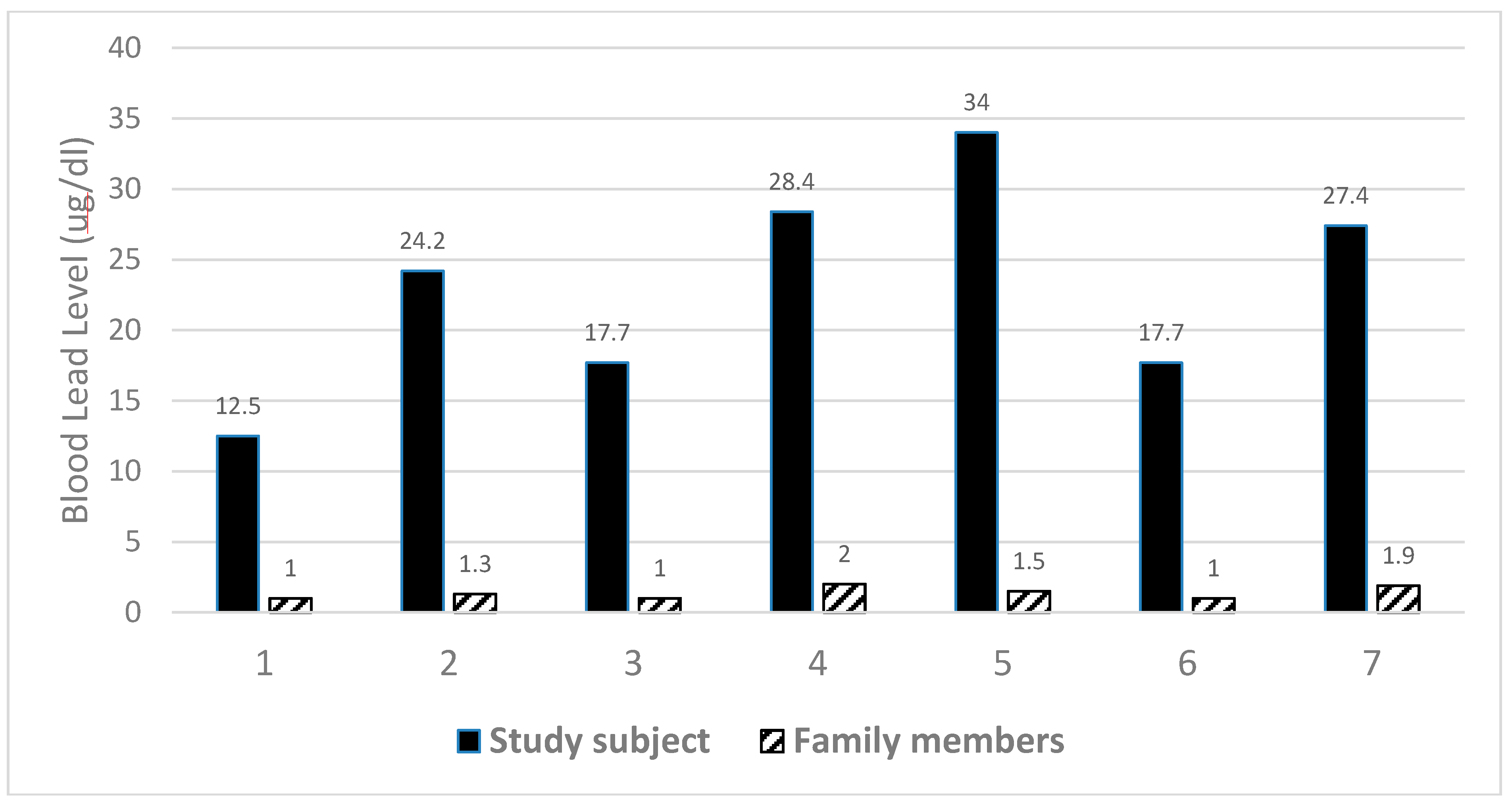
3.4. Blood Lead Distributions

{kind=link}
{kind=link}
| Study code | Sex | Year of birth | Occupation | Ingestion of Ayurvedic medication | Highest blood lead level | Current blood lead level | Chelation treatment | % body weight loss during acute phase | Symptoms during acute phase | Current health status |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | F | 1996 | School student | 4 capsules/day for 3 months | 116 | 12.5 | DMSA >13 courses over two years | 12.7 | Tiredness, nausea, anemia, abdominal cramps, shortness of breath, severe itching | Ankylosing spondylitis, polycystic ovaries, back, knee and hip aches |
| 2 | M | 1994 | School student | 4 capsules/day for 3 months | 34 | 24.2 | 2 courses (DMSA) | 8.6 | Nausea, tiredness, emotional instability | Tiredness, headaches, nausea, mood swings, occasional vomiting |
| 3 | F | 1998 | School student | 4 capsules/day for 1 month | 86 | 17.7 | 2 courses (DMSA) | 5.5 | none | Headaches, stomach pains |
| 4 | F | 1997 | School student | 3 capsules/day for 6 months | 72 | 28.4 | 2 courses (DMSA) | 20.0 | Abdominal cramps, headaches, soreness over entire body | Knee and back aches |
| 5 | M | 1997 | School student | 4 capsules/day for 2 years | 66 | 34.0 | 2 courses (DMSA) | 26.8 | Leg pains, loss of appetite, tiredness, difficulty concentrating, irritability, weakness & pain in joints & muscles, clumsiness | Feels “fine” |
| 6 | F | 1998 | School student | 4 capsules/day for 18 months | 92 | 17.7 | 3 courses (one course of Penicillamine, followed by two courses of DMSA) | 5.5 | Abdominal pain, nausea, anemia, tiredness, lethargy, drowsiness, extreme shortness of breath, vomiting, difficulty concentrating, impaired memory, irritability, weakness & pain in joints & muscles, severe itching, clumsiness | constipation |
| 7 | M | 1994 | School student | 4 capsules/day for 4 months | 76 | 27.4 | 4 courses (DMSA) | 4.2 | Abdominal pain, tiredness, headaches, difficulty concentrating | Feels “good” but occasional tiredness and abdominal pains |
| 8 | F | 1986 | Non-lead occupation | 3 capsules/day for 3 weeks | 42 | 10.4 | 1 course (DMSA) | 10.2 | Backache that worsened over time, severe nausea and abdominal cramps, loss of appetite, weakness, confined to bed | Well |


3.5. Health Status
3.6. Treatment
3.7. Lead Content of Implicated Ayurvedic Medicine
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References and Notes
- Saper, R.B.; Phillips, R.S.; Sehgal, A.; Khouri, N.; Davis, R.B.; Paquin, J.; Thuppil, V.; Kales, S.N. Lead, mercury, and arsenic in US-and Indian-manufactured Ayurvedic medicines sold via the Internet. JAMA 2008, 300, 915–923. [Google Scholar] [CrossRef] [PubMed]
- Kales, S.N.; Saper, R.B. Ayurvedic lead poisoning: An under-recognized, international problem. Indian J. Med. Sci. 2009, 63, 379–381. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Lead poisoning associated with Ayurvedic medications —Five States, 2000–2003. MMWR 2004, 53, 582–584. [Google Scholar]
- Saper, R.B.; Kales, S.N.; Paquin, J.; Burns, M.J.; Eisenberg, D.M.; Davis, R.B.; Phillips, R.S. Heavy metal content of Ayurvedic herbal medicine products. JAMA 2004, 292, 2868–2873. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Lead poisoning in pregnant women who used Ayurvedic medications from India–New York City. MMWR 2012, 61, 641–646. [Google Scholar]
- Desai, A.; Staszewski, H. Ayurvedic remedy for diabetes as a cause of lead poisoning: A case report. Am. J. Med. 2012, 125, e3–e4. [Google Scholar] [CrossRef] [PubMed]
- Gupta, N.; Goswami, B.; Singh, N.; Koner, B.C.; Garg, R. Lead poisoning associated with Ayurvedic drug presenting as intestinal obstruction: A case report. Clin. Chim. Acta 2011, 412, 213–214. [Google Scholar] [CrossRef] [PubMed]
- Dargan, P.I.; Gawarammana, I.B.; Archer, J.R.; House, I.M.; Shaw, D.; Wood, D. Heavy metal poisoning from Ayurvedic traditional medicines: An emerging problem? Int. J. Environ. Health 2008, 2, 463–474. [Google Scholar] [CrossRef]
- Naicker, N.; Mathee, A.; Barnes, B. Environmental lead—A public health challenge in South Africa. Epidemiology 2013, 24, 621–622. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Guidelines for Assessing Quality of Herbal Medicines with Reference to Contaminants and Residues. 2007. Available online: http://apps.who.int/medicinedocs/index/assoc/s14878e/s14878e.pdf (accessed on 3 June 2015).
- Mathee, A.; von Schirnding, Y.E.; Levin, J.; Ismail, A.; Huntley, R.; Cantrell, A. A survey of blood lead levels among young Johannesburg school children. Environ. Res. 2002, 90, 181–184. [Google Scholar] [CrossRef]
- Mathee, A.; Rollin, H.; Levin, J.; Naik, I. Lead in paint: Three decades later and still a hazard for African children? Environ. Health Perspect. 2007, 115, 321–322. [Google Scholar] [CrossRef] [PubMed]
- Mathee, A.; Singh, E.; Mogotsi, M.; Timothy, G.; Maduka, B.; Olivier, J.; Ing, D. Lead-based paint on playground equipment in public children’s parks in Johannesburg, Tshwane and Ekurhuleni. S. Afr. Med. J. 2009, 99, 819–821. [Google Scholar] [PubMed]
- Mathee, A.; Khan, T.; Naicker, N.; Kootbodien, T.; Naidoo, S.; Becker, P. Lead exposure in young school children in South African subsistence fishing communities. Environ. Res. 2013, 126, 179–183. [Google Scholar] [CrossRef] [PubMed]
- Montgomery, M.; Mathee, A. A preliminary study of residential paint lead concentrations in Johannesburg. Environ. Res. 2005, 98, 279–283. [Google Scholar] [CrossRef] [PubMed]
- Dubey, N.K.; Kumar, R.; Tripathi, P. Global promotion of herbal medicine: India’s opportunity. Current Sci. 2004, 86, 37–41. [Google Scholar]
- Wu, T.-N.; Yang, K.-C.; Wang, C.-M.; Lai, J.-S.; Ko, K.-N.; Chang, P.-Y.; Liou, S.-H. Lead poisoning caused by contaminated Cordyceps, a Chinese herbal medicine: two case reports. Sci. Total. Environ. 1996, 182, 193–195. [Google Scholar] [CrossRef]
- Street, R. Heavy metals in medicinal plant products—An African perspective. S. Afr. J. Bot. 2012, 82, 67–74. [Google Scholar] [CrossRef]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mathee, A.; Naicker, N.; Teare, J. Retrospective Investigation of a Lead Poisoning Outbreak from the Consumption of an Ayurvedic Medicine: Durban, South Africa. Int. J. Environ. Res. Public Health 2015, 12, 7804-7813. https://doi.org/10.3390/ijerph120707804
Mathee A, Naicker N, Teare J. Retrospective Investigation of a Lead Poisoning Outbreak from the Consumption of an Ayurvedic Medicine: Durban, South Africa. International Journal of Environmental Research and Public Health. 2015; 12(7):7804-7813. https://doi.org/10.3390/ijerph120707804
Chicago/Turabian StyleMathee, Angela, Nisha Naicker, and June Teare. 2015. "Retrospective Investigation of a Lead Poisoning Outbreak from the Consumption of an Ayurvedic Medicine: Durban, South Africa" International Journal of Environmental Research and Public Health 12, no. 7: 7804-7813. https://doi.org/10.3390/ijerph120707804