
Abstract
Deaths in temporal association with vaccination of hexavalent vaccines have been recently reported. The objective of this paper is to assess whether these temporal associations can be attributed to chance. Standardised mortality ratios (SMR) for deaths within 1 to 28 days after administration of either of the two hexavalent vaccines in the 1st and 2nd year of life were determined using the respective annual rates for sudden unexpected deaths (SUDs) from the national vital statistics. The distribution of SUD cases and the vaccination uptake by month were estimated from surveys and sales figures for the individual vaccines. Sensitivity analyses were performed to account for limitations in the data sources. For one of the vaccines, Vaccine B, all SMRs were well below one. For the other, Vaccine A, SMRs exceeded one insignificantly on the 1st day after vaccination in the 1st year of life. In the 2nd year of life, however, the SMRs for SUD cases within 1 day of vaccination with vaccine A were 31.3 (95% CI 3.8–113.1; two cases observed; 0.06 cases expected) and 23.5 (95% CI 4.8–68,6) for within 2 days after vaccination (three cases observed; 0.13 cases expected). Extensive sensitivity analyses could not attribute these findings to limitations of the data sources. Conclusion: These findings based on spontaneous reporting do not prove a causal relationship between vaccination and sudden unexpected deaths. However, they constitute a signal for one of the two hexavalent vaccines which should prompt intensified surveillance for unexpected deaths after vaccination.


Similar content being viewed by others

Abbreviations
- DTPa-IPV-HBV-Hib :
-
diphtheria, tetanus, pertussis, poliomyelitis, hepatitis B, Haemophilius influenzae type b
- PEI :
-
Paul Ehrlich Institute
- SMR :
-
standardised mortality ratio
- SUD :
-
sudden unexplained death
References
Bouvier-Colle MH, Flahaut A, Messiah A, Jougla E, Hatton F (1989) Sudden infant death and immunization: an extensive epidemiological approach to the problem in France—winter 1986. Int J Epidemiol 18: 121–126
Edwards IR, Biriell C (1994) Harmonisation in pharmacovigilance. Drug Safety 10: 93–102
Fine PE, Chen RT (1992) Confounding in studies of adverse reactions to vaccines. Am J Epidemiol 136: 121–135
Fleming PJ, Blair PS, Platt MW, Tripp J, Smith IJ, Golding J (2001) The UK accelerated immunisation programme and sudden unexpected death in infancy: case-control study. BMJ 322: 822
Gilbert RE, Fleming PJ, Azaz Y, Rudd PT (1990) Signs of illness preceding sudden unexpected death in infants. BMJ 300: 1237–1239
Golding J (1986) Immunisations. In: Butler NR, Golding J (eds) From birth to five: a study of the health and behaviour of Britains’ 5-year-olds. Pergamon Press, Oxford, pp 295–319
Griffin MR, Ray WA, Livengood JR, Schaffner W (1988) Risk of sudden infant death syndrome after immunization with the diphtheria-tetanus-pertussis vaccine. N Engl J Med 319: 618–623
Hoffman HJ, Hunter JC, Damus K, Pakter J, Peterson DR, van Belle G et al (1987) Diphtheria-tetanus-pertussis immunization and sudden infant death: results of the National Institute of Child Health and Human Development Cooperative Epidemiological Study of Sudden Infant Death Syndrome risk factors. Pediatrics 79: 598–611
Hutchins SS, Escolan J, Markowitz LE, Hawkins C, Kimbler A, Morgan RA et al (1989) Measles outbreak among unvaccinated preschool-aged children: opportunities missed by health care providers to administer measles vaccine. Pediatrics 83: 369–374
Jonville-Bera AP, Autret-Leca E, Barbeillon F, Paris-Llado J (2001) Sudden unexpected death in infants under 3 months of age and vaccination status—a case-control study. Br J Clin Pharmacol 51: 271–276
Keller-Stanislawski B, Löwer J (2003) Todesfälle in zeitlichem Zusammenhang mit Sechsfachimpfung. Kinder- und Jugendarzt 8: 608–613
Marks JS, Halpin TJ, Irvin JJ, Johnson DA, Keller JR (1979) Risk factors associated with failure to receive vaccinations. Pediatrics 64: 304–309
Mitchell EA, Stewart AW, Clements M (1995) Immunisation and the sudden infant death syndrome. New Zealand Cot Death Study Group. Arch Dis Child 73: 498–501
Platt MW, Blair PS, Fleming PJ, Smith IJ, Cole TJ, Leach CE et al (2000) A clinical comparison of SIDS and explained sudden infant deaths: how healthy and how normal? CESDI SUDI Research Group. Confidential Inquiry into Stillbirths and Deaths in Infancy study. Arch Dis Child 82: 98–106
Roberts SC (1987) Vaccination and cot deaths in perspective. Arch Dis Child 62: 754–759
Roper J, Day S (1988) Uptake of immunisations in low birth weight infants. Arch Dis Child 63: 518–521
Schmitt HJ, von Kries R, Hassenpflug B, Hermann M, Siedler A, Niessing W et al (2001) Haemophilus influenzae type b disease: impact and effectiveness of diphtheria-tetanus toxoids-acellular pertussis (-inactivated poliovirus)/ H. influenzae type b combination vaccines. Pediatr Infect Dis J 20: 767–774
STIKO (2002) Empfehlungen der ständigen Impfkommission (STIKO)am Robert Koch-Institut/Stand Juli 2002. Epidemiol Bull 28: 227–242
Van Puijenbroek EP, van Grootheest K, Diemont WL, Leufkens HG, Egberts AC (2001) Determinants of signal selection in a spontaneous reporting system for adverse drug reactions. Br J Clin Pharmacol 52: 579–586
Acknowledgements
The reports for the SUD cases in temporal association with the administration of hexavalent vaccines were made available to us by Dr. Brigitte Keller-Stanislawski from the PEI, Langen, Germany. This work was supported by a grant from the PEI.
Author information
Authors and Affiliations
Corresponding author
Additional information
In this paper the two vaccines have been labelled Vaccine A and Vaccine B. The brand names are not conveyed since the European licensing agency has not recommended regulatory action against either vaccine. http://www.emea.eu.int/pdfs/human/press/pus/588903en.pdf
Appendix
Appendix
Let T denote the time to death from SUD by months. To derive the expected deaths needed in calculating the denominator of SMRs, estimations of the following quantities are available:
Let \( \lambda _{i} = P{\left( {i \leqslant T < i + 1\left| {T \geqslant i} \right.} \right)} \) denote the mortality from SUD for month [ i,i + 1). From
we obtain the following recursive formula for the \( \lambda _{i} {\text{'s}} \)
and
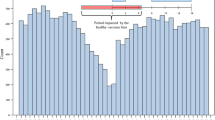
Let S denote the set of all birth cohorts crossing the rectangle, and let N k be the number of children from cohort \(k \in S\) who contribute to the study period (being the rectangle in the Lexis diagram). Furthermore, let I k denote the number of age classes of cohort \(k \in S\) which fall into the study period. Because, children vaccinated in month [ i,i + 1) of age are at risk of sudden death in the following month with incidence
on average, concerning cohort \(k \in S\), for the number of expected deaths among the vaccinated children in age class \(i \in I_{k} \) contributing to the study period we obtain the expression \( \frac{{\lambda _{i} + \lambda _{{i + 1}} }} {2}p^{{(v)}}_{i} N_{k} . \) Thus, the expected number from SUD cases in the 1st month after vaccination is
Rights and permissions
About this article
Cite this article
von Kries, R., Toschke, A.M., Straßburger, K. et al. Sudden and unexpected deaths after the administration of hexavalent vaccines (diphtheria, tetanus, pertussis, poliomyelitis, hepatitis B, Haemophilius influenzae type b): is there a signal?. Eur J Pediatr 164, 61–69 (2005). https://doi.org/10.1007/s00431-004-1594-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00431-004-1594-7