Article Text

Abstract
Objective The understanding of acceptability of existing dosage forms is limited in most of the world and hinders the development of acceptable, age‐appropriate medicines. The attributes of paediatric medicine acceptability may differ from country to country based on culture, healthcare infrastructure and health policies. This study was designed to map the acceptability of oral medicines in paediatric patients treated in hospital in India.
Methods An observational, cross-sectional study was conducted in patients aged below 18 years and taking any form of oral medication. Acceptability scores were obtained using CAST–ClinSearch Acceptability Score Test tool.
Findings 490 patients were recruited and 193 evaluations of different pharmaceutical products available in 20 dosage forms and 7 routes of administration were studied. Oral liquids (50%) and tablets (35%) were the most commonly prescribed and administered forms. Regardless of the therapeutic class and age, the oral liquids were ‘positively accepted’ in infants and toddlers. Acceptability of tablets improved with age and appeared to be generally good from the age of 6.
Conclusion This study indicates the limited progress towards adoption of age-appropriate dosage forms in India and thus impact on the acceptability of existing oral dosage forms. The key challenges posed by the adoption of age-appropriate formulations in India are (1) awareness of importance of appropriate administration and acceptability of medicines to children in India, (2) availability of age-appropriate dosage forms and (3) lack of child-appropriate medicine policies.
- dosage form
- pharmaceutical preparations
- age appropriate
- child
- medicines
- administration and dosage
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information. All data relevant to the study are included in the article or uploaded as supplementary information.
Statistics from Altmetric.com
What is already known on this topic?
The development of acceptable dosage forms for children in low-to-middle-income countries (LMICs) is one of the priorities of WHO to address childhood morbidity and mortality issues.
Children and adults differ in many aspects from the other age subsets of the population and require particular considerations in medication acceptability.
Selecting an appropriate adapted dosage form for children permits healthcare professionals to improve acceptability. However, the understanding of acceptability is still relatively nascent in LMICs.
What this study adds?
The study helped to understand the real-time scenarios of formulations acceptability in paediatric population in the hospital setting in India.
Liquid formulations are most commonly prescribed and acceptable to the overall age groups; however, their shortcomings make it a suboptimal dosage form for children.
Tablets are acceptable to children over 5 years; however, the administration was often not supported with proper instructions and followed inappropriate manipulation practice.
Introduction
Improving the understanding of the acceptability of different dosage forms for children is currently an area of high interest, to help address the global issue of lack of age-appropriate medicines for children and widespread off-label/unlicensed medicines use in paediatric population.1 2 A lack of sufficient consistent evidence required to make an informed decision on acceptability and preference of dosage forms in different age groups hinders the development of acceptable, age-appropriate medicines.3 Most of the acceptability studies published are conducted in Europe and the USA.4–7 However, the attributes of acceptability that are important to this cohort may differ from country to country based on culture, healthcare infrastructure and health policies. Hence, it is important to gauge the factors that may hinder the acceptability of dosage forms in children in different countries. WHO also have highlighted the need for the methodological research on assessing the acceptability and that the economic and cultural context in which children live and ease of administration in both hospital and home care setting should be taken into consideration in the development of appropriate formulations for children.8 This observational study was conducted in a hospital in India to investigate the acceptability of dosage forms in the local paediatric population.
Methods
Study design and setting
This prospective, cross-sectional, observational study was carried out in the outpatient department of a tertiary care hospital in Pune, India. The observed participants in the study were parents, carers, healthcare professionals and paediatric patients aged 0–15 years.
Participants and recruitment
The participants were included without any randomisation in the study as per the inclusion/exclusion criteria and study methodology summarised in figure 1. The consent was obtained from the parents/carers, and children of 8 years and above, while assent was obtained from children under 8 years.

Study methodology. This figure was created by Thibault Vallet, one of the coauthors of the manuscript.
Data collection
The medicine acceptability was evaluated using a validated methodology, ClinSearch Acceptability Score Test (CAST) entailing a standardised web questionnaire to collect evaluations of medicine intake and data analysis process to score acceptability.6 9–13 Each participant was interviewed by a trained researcher (observer) who completed the web questionnaire as per the parent’s/caretaker’s and patient’s response and reported their own observations (figure 1).
Each evaluation of one medicinal product taken or used by one patient in a specific context corresponded to a particular combination of an observed measure (eg, the required dose fully taken) for each of the nine observational variables (eg, the result of intake) which describe many aspects of acceptability.
Data analysis
The acceptability reference framework is based on multivariate analysis mining a large set of 3130 evaluations, composed of those from India study herein and those collected from six other countries in both domestic and hospital settings since May 2015.6 9–13
First a multiple correspondence analysis (MCA) visualised similarity between evaluations and the key relationships between the 21 observed measures into a comprehensible and low-dimensional Euclidean space: the 3D acceptability map. All of the evaluations were positioned on the map depending on their similarity: the most similar evaluations converged. Afterward, hierarchical clustering on principal components and k-means consolidation gathered similar evaluations. The clusters defined coherent positively and negatively accepted profiles materialised by a green and a red area on the map, respectively.
The evaluations collected in India were successively partitioned into subgroups of interest, according to patient age groups and medicine dosage forms. In each case, the subgroup of interest was positioned on the map at the barycentre of the selected evaluations. If a barycentre, along with the entire 90% confidence ellipsis surrounding it, belonged to the green area of the map, the subgroup could be classified as ‘accepted’. A minimum of 30 evaluations are required to obtain a reliable acceptability score. The R packages FactoMineR14 and MissMDA15 were used to perform multivariate investigation and to deal with missing information, separately.
Results
Patients and medicines
A total of 490 participants were recruited and the use of 193 distinct pharmaceutical products were identified from the data collected (table 1). Antiepileptics (14%) and antibacterial (12%) were the commonly prescribed therapeutic subgroups of medicines followed by analgesics (11%) and vitamins (10%). The oral liquids including syrups and oral suspensions (50%) and tablets (35%) were mostly prescribed and administered forms. Hence, the focus of this study was limited to oral liquids and tablets only due to the insufficient number of evaluations (n<30) for the other oral pharmaceutical forms (table 1).
Patient and medicine characteristics
Acceptability of commonly prescribed dosage forms as per age group
For all the 415 evaluations (oral liquids (n=244) and tablets (n=171), 64% of the patients expressed a positive reaction towards the acceptance of the medication. Ninety-one per cent took all the prescribed dose administered by the caretaker or via self-administration. The barycentre of 244 evaluations for oral liquids and 171 for tablets, along with the confidence ellipses surrounding them, were fully located in the green area of the acceptability map corresponding to the ‘positively accepted’ profile (figure 2).
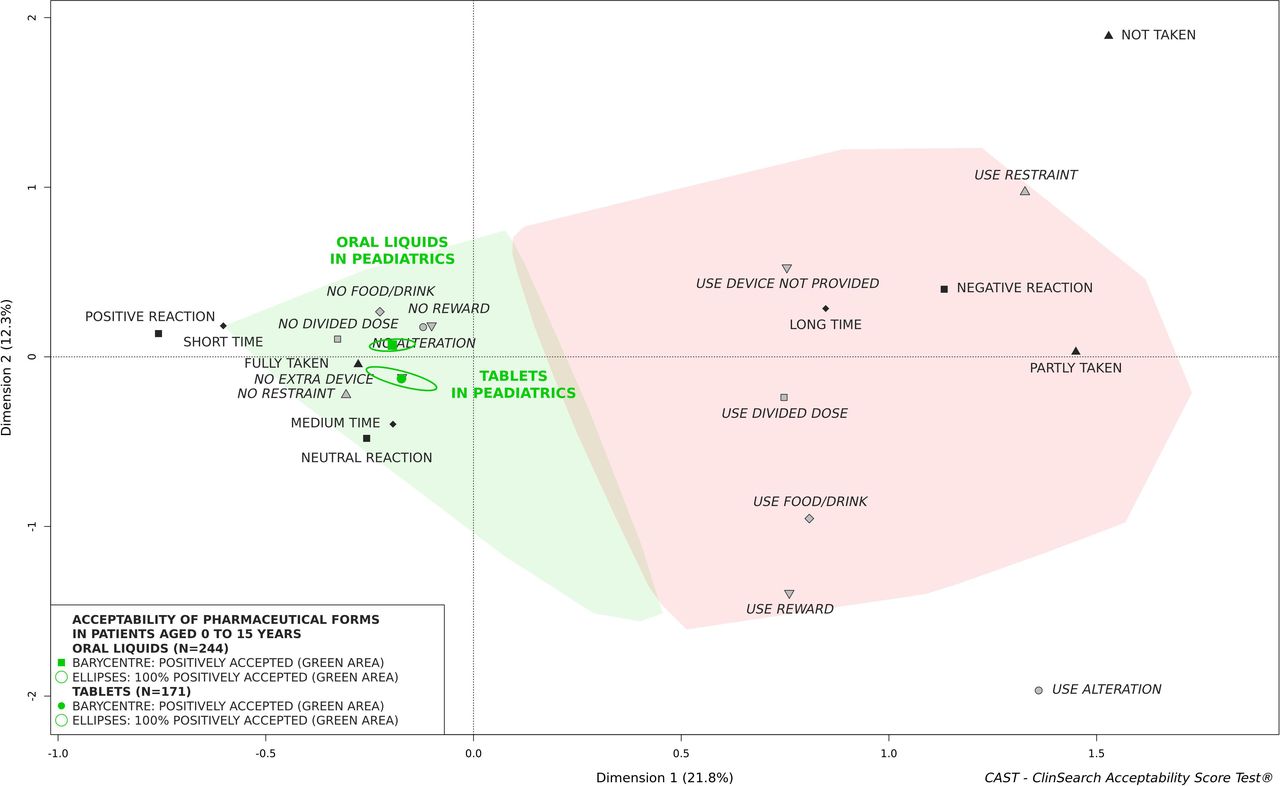
Acceptability of liquids and tablets. This figure was created by Thibault Vallet, one of the coauthors of the manuscript.
Oral liquids were well accepted regardless of the patient’s age (figure 3). Due to a very small number of evaluations (n=9), children aged 12 and over were not represented on the map. Syrups and suspensions could be classified as accepted (online supplemental figure 1). Seventy-two per cent of the 69 liquid products included information on the flavour or sweetener while for 27% no information was available on the inclusion of flavour or sweetener but cannot be concluded they did not contain flavour or sweetener. The flavour used were mixed fruit, menthol, strawberry, pineapple and raspberry.
Supplemental material

Acceptability of liquids depending on age. This figure was created by Thibault Vallet, one of the coauthors of the manuscript.
Tablets could be classified as ‘positively accepted’ in children aged 6 and over. For children aged 3 to 5 years, a significant part of confidence ellipses fell within the red area of the acceptability map, and the barycentre of 36 evaluations in children aged 0 to 2 years was also located in this area, indicating that tablets were not positively accepted in children aged 0 to 5 years (figure 4). Different methods were used to ease administration of tablets: (1) division of the required dose intake (27%); (2) use of administration devices that were not provided with the medication (11%); (iii) use of food or drink (21%) either by mixing the drug or taking it before or after the intake to mask the taste or ease swallowing. Alteration of the intended use of medicinal product was seen for 20% of the evaluations. All the negatively connoted observed measures were stated more frequently in the younger children aged 0 to 2 years and for the products that had to be administered by the carers (online supplemental tables 1 and 2).
Supplemental material
Supplemental material

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Acceptability of tablets depending on age. This figure was created by Thibault Vallet, one of the coauthors of the manuscript.
Discussion
This study is the first to systematically assess the acceptability of oral dosage forms in children in India. The available studies from India are focused on prescription pattern and drug use but do not refer to the acceptability of dosage forms.16 This reflects that the importance of acceptability may not be recognised in India.
The data were collected for a broad category of medicines (20 dosage forms and 7 routes of administration) in patients up to 15 years with distinctive diseases (47 therapeutic groups). The liquid forms were mostly prescribed form (55%) followed by tablets (35%) and hence the discussion is limited to oral liquids and tablets only. The majority of patients in this study were ≥6 years (54%), for whom liquid formulations or manipulating existing dosage form remains to be the only option when no age-appropriate solid dosage form was available. Tayal et al 17 found that some regularly prescribed medicines to children (eg, amoxicillin, albendazole) were in tablet form and had to be fragmented, despite that they were available in liquid forms in the state essential medicines list. Few studies have emphasised the need of educating doctors about prescribing liquids instead of prescribing tablets or capsules that need manipulation to ease administration in younger age groups.18 19 This reflects the discrepancy between the availability of the marketed paediatric medicines and the medicines needed in daily practice, which drives the prescription pattern.
Considering the liquid formulation can sometimes be the only available option for treatment, there is a greater need to ensure the acceptability of these preparations. Our study indicated that regardless of therapeutic area, oral liquids were well accepted by the children aged 0–15 years in India. This is in contrast to a similar study performed in Morocco.13 Oral liquids considered as a whole, either ready to use or to be reconstituted, were positively accepted in children aged 3 and over in Morocco as opposed to India, where it was accepted by all age groups including under 3 years. The medicine was fully or partly taken without almost any alteration or promise for a reward for the liquid forms that were acceptable. However, 41% reported division of the dose to ease administration. The preparation steps such as reconstitution, dose division are risk factors for medication errors associated with liquids. The irrationality in manufacturing paediatric liquid dosage forms in relation to the age group is an issue and is highlighted by Naik et al.20 The study analysed paediatric antibacterial liquid formulations in India and found that majority of manufacturers dispensed inadequate volume of antibacterial drugs which was not sufficient for one course of therapy. This resulted into inadequate dose, wastage of drug (residual volume), resistance, and unnecessary social and financial burden to the patient. Furthermore, the use of devices that was not provided with the products (eg, household spoons, oral syringes, droppers) was reported by 15%. Published studies have highlighted that caregivers lacked proper knowledge of the use of appropriate devices and the administration of proper doses to children.21 Another issue is that liquid formulations often require multiple or high level of excipients to address the issues with stability, palatability and so on. The poor organoleptic properties are well known to negatively impact the acceptability of oral liquids and hence sweeteners or flavours are used.22 In this study, most of oral liquid products included flavour or sweetener. This may have helped with the acceptability of liquids in children as reported in the study in Tanzania.23 The sweeteners such as sucrose which is predominantly used in paediatric medicines and its impact on the oral health status of children need to be considered.24 Physiologically acceptable acids (eg, citric acid) can be used along with sucralose to upturn the taste-masking efficiency of the sweetener.25 Considering the cariogenic and erosive potential of sweetened and acidic medications prescribed to children, it is important to educate paediatricians and parents to ensure adequate oral clearance after each dose of medication to minimise the risk of erosion and dental caries in children. In addition, liquids often include other excipients of concern such as preservatives and solvents, with reports of possible toxicity in paediatric patients.26 27 The list of the excipients is neither included on the label nor in the patient information leaflet in India. In general, there is less awareness of the concerns of exposure of excipients in paediatric patients and shortcomings of liquid formulations in resource-poor settings.28
The other commonly prescribed dosage forms in this study were tablets (35%). The tablets were prescribed for all age groups from 0 to 15 years. Although tablets are not considered suitable for children under the age of 2 years, it was seen that 20% of children in this age group received tablets even when liquid formulations were available for some drugs such as azithromycin. This could be due to the high cost associated with the liquid formulations. For 64% of the children (0–2 years) who were prescribed tablets, parents had to make modifications. Splitting, crushing tablets and mixing with food were the most frequently reported methods of administration for children aged 0 to 10 years. Previous research looking at the acceptability of tablets in children in the USA,5 UK29 and Europe,30 31 and Tanzania23 aligns closely with the findings of this study, suggesting that although the culture, healthcare infrastructure and health policies may be quite different, acceptability of tablets in children over 3 years and administration practices for children under 3 years were similar in India. It was seen that the tablets that were not meant to be broken or crushed such as delayed release orally disintegrating tablets (eg, lansoprazole) were crushed and administered with an oral syringe.32 This indicates that the manipulation of tablets by parents was not supported by instructions.
The globally designed child-appropriate formulations are still absent in the low-to-middle-income countries (LMICs). WHO now recommends that for paediatric treatment, liquid formulations should be avoided when possible in favour of solid dosage forms and ideally if dispersible, fixed-dose combination tablets are available.33 These child-friendly formulations are becoming increasingly available for diseases like malaria and HIV in LMICs. However, it may take a while for these formulations to be available for other disease areas, becoming the first choice and replacing the need for liquids. Moreover, evaluations of alternative to liquids such as dispersible tablets and granules are required to effectively assess the acceptability of dosage forms. Also, generic formulations could vary a lot depending on manufacturers or countries and can have an impact on acceptability.34 Hence, further investigations assessing the differences in formulations (eg, flavour, viscosity), geographical regions and its impact on acceptability are required. The need to assess the acceptability of medicines to children has become more represented in the published literature in recent years. Although the evidence base is growing, most of the publications are predominantly from resource-rich settings4 31 and very few from resource-limited countries.35 It is a relatively new topic for many resource-limited countries, for whom the foremost priority is to improve the availability and affordability of medicines for children. However, there is a need to educate healthcare professionals and policy decision-makers that the acceptability of medicines is equally important to access of medicines. The European Medicines Agency (EMA) has included a section on acceptability in their guideline on the development of medicines for paediatric use.36 Similarly, for LMICs, the integration of evaluation of acceptability and appropriate administration of solid oral dosage forms in prescription and dispensing policies may help improve the situation. There is a need for coalitions between actors to influence the development of policies and facilitate communication with communities. Hence, the Paediatric Medicines and Healthcare Initiative (PMHI) has been established to foster discussions needed to develop a road map for formulation and adoption of age-appropriate medicines for children in India.37
Conclusion
The relevant knowledge on oral medicine acceptability extracted from this Indian study will help raise awareness of concerns associated with medicine administration practices, limitations of currently available dosage forms and its impact on acceptability in India. Importance of acceptability is still relatively new, even in countries with a well-established research tradition; it may take time for it to gain traction in countries such as India without this tradition. There is a need to integrate the importance of acceptability with appropriate administration practice in health policies in India. This may consequently have an impact on the transition to child-appropriate formulations in India.
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information. All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
Approval was obtained by the Institutional Ethics Committee of Bharati Hospital and Medical College, Pune (BVDUMC/IEC/11).
Acknowledgments
We would like to acknowledge Dr Swati Mutha, Asst Professor from Vishwakarma University, Pune, India for her kind support in collection of part of the data for the study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors FR and TV conceptualised and designed the study. TV provided support in the design of the study towards the calculation of the sample size; conducted the data analysis, reviewed and revised the manuscript, and approved the manuscript as finally submitted. SS and VP supervised the conceptualisation and design of the study, supervised the recruitment process and data collection, reviewed and revised the manuscript, and approved the final manuscript as submitted. MS provided support in the design of the study towards the participant recruitment and was responsible for internal affairs at the hospitals. MS, RS and SA coordinated the participant recruitment, collected data/responses from patients and supported manuscript preparation through data analysis. SS drafted the initial manuscript and approved the final manuscript as submitted. VP, MSF, FR and TV reviewed and revised the manuscript and approved the final manuscript as submitted. SS will be acting as guarantor and accepts full responsibility for the work and/or the conduct of the study, had access to the data, and controlled the decision to publish.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Linked Articles
- Highlights from this issue