Article Text

Abstract
Background: Inhaled corticosteroids (ICS) are effective treatment for childhood asthma. Cross-sectional studies indicate that some asthmatic children are treated with excessively high doses of ICS and are at risk of serious adverse effects.
Objective: To describe longitudinal trends in asthma prescribing for children, with particular reference to very-high-dose (unlicensed) ICS prescribing.
Design: Retrospective, cross-sectional, observational study of general practitioner prescribing for asthma drugs in children aged under 12 years with a recorded asthma diagnosis between 1992 and 2004 using the General Practice Research Database (GPRD).
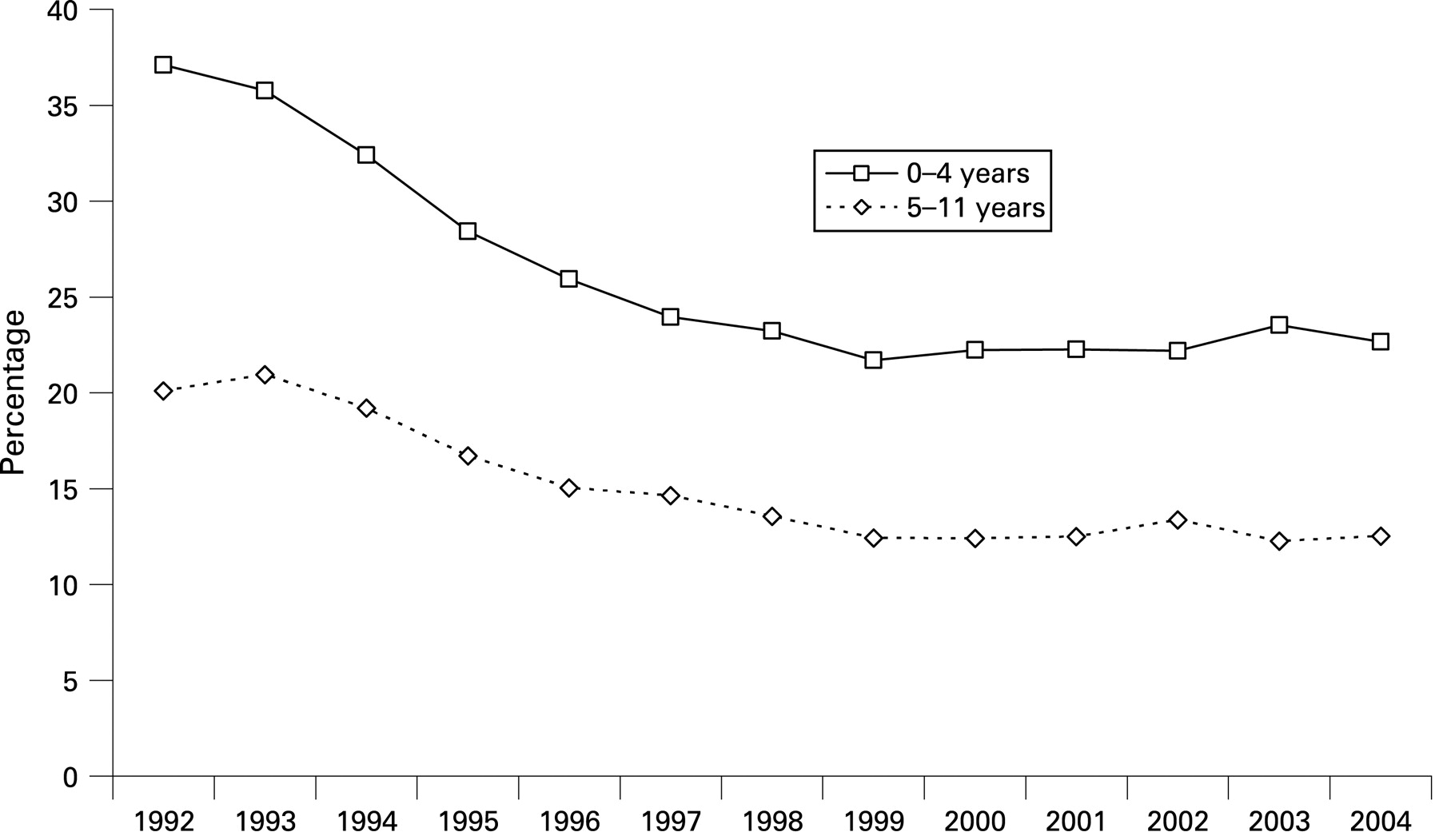
Results: Data were available for an average of 357 956 children per year. The percentage of children prescribed ICS increased from 2.7 in 1992 to 7.0 in 1997 and 1998 and then fell to 3.3 in 2004. In children under 5 years with asthma, very-high-dose ICS prescriptions (>400 μg/day) fell from 10.6% of all ICS prescriptions in 1992 to 4.5% by 2004. In contrast, very-high-dose ICS prescriptions (>800 μg/day) for asthmatic children aged 5–11 years rose from 1.1% in 1992 to 4.6% in 2004. Oral corticosteroid prescribing in under 5-year-olds who had been prescribed ICS fell from 37.1% in 1992 to 21.7% 1999 and remained constant thereafter; the respective percentages for those aged 5–11 years olds were 20.1 and 12.4.
Conclusions: Trends for corticosteroid prescribing in childhood asthma changed dramatically between 1992 and 2004. There are several plausible reasons for this.
Statistics from Altmetric.com
Asthma is a common childhood disease managed principally in the community. The prevalence of childhood asthma globally continues to increase, although it may have peaked in developed countries with an already high prevalence.1 Inhaled corticosteroids (ICS) are the principal preventive treatment for persistent asthma in children, and are advocated as maintenance treatment for all but the mildest disease.2 3 The safety profile of ICS when used in standard doses is good.4 Prospective studies have shown that, although at standard doses (up to 400 μg/day of beclometasone dipropionate or equivalent) a temporary reduction in growth velocity may occur after the start of ICS treatment, any reduction in the final adult height achieved is minor5 6 and prolonged treatment with such doses does not result in measurable effects on the hypothalamic–pituitary axis.7
What is already known on this topic
There is inappropriate high dose prescribing of inhaled corticosteroids (ICS) in asthmatic children.
What this study adds
The percentage of children prescribed ICS increased from 2.7 to 7.0 between 1992 and 1997 and then reduced to 3.3 by 2004.
For younger children, prescribing of ICS in unlicensed doses (ie, in excess of 400 μg/day) reached a peak in 1997.
In older children, prescribing of ICS in unlicensed doses (ie, in excess of 800 μg/day) increased progressively between 1992 and 2004.
Safety concerns do exist, however, in relation to exposure to high and very high (unlicensed) doses of ICS,8 9 and co-exposure to other topical corticosteroids (eg, nasal steroids) needs to be factored when assessing the total exposure.10 Clinicians are recommended to use the lowest effective dose of ICS, to use high-dose treatment only when all else has been tried, and to step down the dose when possible.2 3 In practice, however, it is possible that some people with asthma may be receiving higher doses of ICS than needed to maintain control.11 Case reports have documented fatalities and life-threatening adrenal crises in children receiving very high doses of ICS.12 13 Dose ranging studies have suggested that, for most children, the clinical effects of ICS reach a ceiling at relatively low doses (such as 200 μg/day fluticasone or 400 μg/day beclometasone dipropionate), and that measurable adrenal suppression is increasingly observed with progressively higher doses.14 15 Suppression of endogenous adrenal function has been found to be common in children receiving higher doses of ICS.7 16–18
Current guidelines2 3 recommend that the maximum dose of ICS in children under 5 years old is 400 μg/day beclometasone (or budesonide, 200 μg/day fluticasone). In children aged 5 to under 12 years, the ceiling recommended dose is 800 μg/day (400 μg/day fluticasone). Individual heterogeneity of response to ICS does exist,14 19 and some children with severe asthma may require higher doses of ICS to achieve disease control.15 Cross-sectional studies have, however, reported that some children in the community may be exposed to a very high ICS load.10 20 We aimed in this study to quantify prescribing and diagnostic trends in the community for childhood asthma over the period from 1992 to 2004 using a well-validated clinical and prescribing database, with particular reference to prescriptions for high doses of ICS.
METHODS
This was a retrospective observational study of UK general practitioner prescribing of asthma medication, using anonymised individual patient clinical and prescribing data contained in the General Practice Research Database (GPRD), a large well-validated UK database extensively used in pharmacoepidemiological studies.21 In the GPRD, a “history of asthma” represents a physician diagnosis, but the objective parameters underpinning this diagnosis are not consistently recorded in a retrievable format.
General Practice Research Database
The GPRD covers 484 practices equivalent to ∼6% of the UK population, which includes England, Scotland, Wales and Northern Ireland and has been validated for respiratory epidemiological studies in primary care.22 The GPRD is representative of all social strata: 18% of practices are in areas of the highest quintile of index of multiple deprivation, 21% in the middle quintile and 22% in the lowest quintile. The number of practices contributing to the GPRD has been relatively static since 2000, and more than 90% of all the practices that have ever contributed in GPRD are currently contributing.
Data extraction
The period of interest was 1992–2004, and data were collected in 2005. All children aged under 12 years on 31 December from 1992 to 2004 with a history of asthma and who received any asthma medication in that year and with full records held in the database from birth or at least 1 year before the first prescription for any anti-asthma drug were identified and analysed. Anti-asthma medication was defined as short-acting β-agonist, inhaled corticosteroid, long-acting β-agonist or chromone, leukotriene receptor antagonist or theophylline. In this study, 1 μg fluticasone dipropionate was assumed to be equivalent to 2 μg budesonide or beclometasone. An online supplement presents details of data extracted. Ethics approval for the study was provided by the scientific and ethical advisory group linked to GPRD.
Asthma admissions data
The number of children aged up to 14 years admitted to hospital in England and Wales with asthma (ICD-10 code beginning J45 or J46) was identified from Hospital Episode Statistics (http://www.hesonline.nhs.uk) and presented as the number of asthma admissions per 1000 admissions.
RESULTS
Table 1 shows the numbers of children in the GPRD on 1 January each year from 1992 to 2004; data were available for an average of 357 956 children per year. The percentage of children with a history of asthma in the database and who were prescribed any asthma treatment rose from 4.1 in 1992, peaking at 8.8 in 1997, before falling back to 4.2 by 2004 (fig 1).

Bronchodilator monotherapy in children with diagnosed asthma
The use of bronchodilator monotherapy (ie, without concomitant ICS) in children with diagnosed asthma rose from 1.4% in 1992 to a peak of 1.8% in 1995 and then fell to 0.4% in 2004 (fig 1).
Receipt of ICS in children with diagnosed asthma
Table 1 shows the number of children who had a diagnosis of asthma receiving ICS. The percentage of all children with diagnosed asthma aged under 12 years who were prescribed ICS rose from 2.7 in 1992 to a peak of 7.0 in 1997 and 1998 and then fell to 3.3 in 2004. When subdivided by age (tables 2 and 3), the percentage of children aged 0–4 years prescribed ICS for asthma showed a rise from 1.0 in 1992 to a peak of 4.8 in 1997 and 1998 and then fell to 1.8 in 2004, and for children aged 5–11 years the percentage prescribed ICS rose from 4.1 in 1992 to 8.6 in 1997 and subsequently fell to 4.2 in 2004.
Receipt of high-dose ICS in children with diagnosed asthma
Owing to imprecise dosing instructions in a proportion of patients (eg, “as directed”), the daily ICS dose was evaluable in an average 77.0% of patients (between 76.0% in 1999 and 77.8% in 1994). Tables 2 and 3 show the numbers of children prescribed high (>400 μg/day on dosing instructions) and very high (>800 μg/day) doses. In children less than 5 years, the percentage receiving ICS for asthma who were prescribed >400 μg/day rose from 10.6 in 1992 to a peak of 13.9 in 1994 and then fell progressively to 4.5 in 2004, and those prescribed >800 μg/day rose from 5.3% in 1992 to a peak of 6.5% in 1994 and then fell progressively to 2.0% in 2004. In children aged 5–11 years, the percentage prescribed >400 μg/day rose from 11.3 in 1992 to 13.9 in 1997 and fell to 8.2 in 2004; however, the percentage prescribed >800 μg/day showed a progressive rise from 1.1 in 1992 to 4.6 in 2004 (table 2 and fig 2). The steroid most commonly prescribed in very high doses was fluticasone dipropionate (fig 3) and consistently accounted for 60–75% of ICS prescribing in doses in excess of 800 μg/day between 1996 and 2004.


“Add-on” therapy in children with diagnosed asthma
The percentage of children with a diagnosis of asthma and prescriptions for ICS who were also prescribed add-on therapy rose progressively from 0.5 in 1992 to 10.7 in 2004. However, even in 2004 there was evidence of under-use of guideline-recommended add-on therapy in conjunction with higher doses of ICS; in the <5-year age group, 69.5% of those prescribed 401–800 μg/day and 49.0% of those prescribed >800 μg/day failed to receive add-on therapy, and in the 5–12-year age group, 60.3% of those prescribed 401–800 μg/day and 29.8% of those prescribed >800 μg/day were not receiving add-on therapy.
Oral corticosteroid courses in children with diagnosed asthma
The percentage of children aged under 5 years and prescribed ICS for asthma who received one or more courses of oral corticosteroids fell from 37.1 in 1992 to 21.7 in 1999, but thereafter remained constant (fig 4). In the 5–11-year age group, the percentage receiving oral steroid courses similarly fell from 20.1 in 1992 to 12.4 in 1999 and also remained constant over the following 5 years.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
DISCUSSION
In this study we have described general practitioner prescribing of asthma drugs in children between 1992 and 2004. An increase in all inhaled asthma treatment use was observed over the early 1990s to a peak in 1997, which fell thereafter. A rising trend for add-on prescribing was observed, but with ongoing evidence of under-use in relation to guideline recommendations for the introduction of add-on therapy in children uncontrolled on moderate doses of ICS alone. Paradoxically, we observed a rise in the percentage of older children prescribed off-licence very-high-dose ICS, an area highlighted by the UK National Prescribing Centre as of concern in paediatric prescribing,23 and this trend requires further investigation and action.
This study was not designed to determine why prescribing for childhood asthma is changing, but there are several plausible explanations. The incidence of asthma may be changing: epidemiological studies observed a rise in childhood asthma during the latter stages of the last century,24 consistent with the rise in the proportion treated for asthma between 1992 and 1996 (fig 1). The increase in prescriptions of ICS may reflect decreasing use of sodium cromoglicate, recommended as first-line asthma prophylaxis in 1993 guidelines25 but not recommended at all in later guidelines. The reduction in ICS prescribing seen between 1997 and 2004 may reflect falling asthma prevalence in the paediatric population. The asthma “epidemic” may be waning in developed societies.1 The percentage of children admitted to hospital with asthma fell between 1998 and 2004 (fig 1) and mortality from childhood asthma has also fallen since 1990.26 Reduced asthma severity may also explain falling ICS prescribing, but we found no evidence for this: prescriptions of bronchodilators without ICS (indicating milder disease/British Thoracic Society (BTS) guideline step 1) did not rise after 1997, whereas add-on prescribing (indicating moderate disease/BTS step 3) increased throughout the period of interest. In all likelihood, a combination of the factors discussed, and others currently unidentified, is likely to be important in the rise and fall of asthma prescribing.
This study is able to relate the 1997 guidelines for asthma management27 to changes in prescribing after that date. The guideline, dated 1995 but published 2 years later, recommended a maximal daily ICS dose of 2000 μg in older children,27 and adherence to this guideline may explain the rising percentage of children receiving ICS who were prescribed high doses (fig 2). The 1997 guideline27 recommended a maximal daily ICS dose of 400 μg in younger children, and there was a fall in high/very high ICS prescribing in this age group after 1995 (fig 2), suggesting that the guideline also influenced ICS prescribing in this age group. The 1997 guideline suggested theophyllines, and long-acting β-agonists could be considered in young children, but the first add-on to be licensed for the under 5s was montelukast in 2001. The low use of add-ons in the under 5-year-olds seen before 2001 may have been due to appropriate prescribing, ie, within licence. The high proportion of older children on high/very-high-dose ICS but not receiving add-ons seen in 2004 is not consistent with the 1997 (or 2003) BTS/Scottish Intercollegiate Guidelines Network (SIGN) guideline. Our observations suggest that the 1997 guideline may have influenced general practitioner prescribing, although there was no evidence of an abrupt change in prescribing at this time.
The percentage of children prescribed ICS reported in this study is approximately one-third of the asthma prevalence reported in epidemiological studies,1 26 but is consistent with other UK-based studies using different primary care databases.10 20 We do not believe that two-thirds of asthmatic children receive no medication. The prevalence of asthma “ever” in the population is inevitably higher than the incidence of current asthma, and prescribing is likely to reflect the latter and not the former; this may partly explain the difference between reported asthma and asthma prescribing. Further, only asthmatic children prescribed medication were eligible for our study. The GPRD is regularly monitored for data quality, and the search strategy used will reliably detect all children prescribed asthma medication and all in whom a physician diagnosis of asthma was recorded. It will not, however, identify all children who might be classified as having asthma in epidemiological surveys, as some patients do not present to a doctor and some who do present with wheezing or other respiratory symptoms may not be given a diagnosis of asthma and may not be prescribed anti-asthma medication.
There are some limitations to this study. Firstly, owing to imprecise dosing instructions in up to one-quarter of children, we were not able to obtain detailed prescribing instructions on all, and, although this is of some concern in itself, the large numbers studied and the smooth curvilinear trends observed reassure us that the results are valid and not substantially influenced by missing data; in addition, the results are consistent with other data obtained from a different source.20 Secondly, complete adherence with asthma drugs is not realistic and thus, although children may be prescribed high doses of ICS, they may not be receiving them. Thirdly, we cannot identify those prescriptions initiated in primary, secondary or tertiary care. Finally, although this study was able to describe the prevalence of asthma treatment in the population, we are not able to report on the prevalence of asthma in the population, as children not prescribed treatment for diagnosed asthma were not identified.
In summary, we have observed a number of changes in general practitioner prescribing of asthma drugs for children in the UK between 1992 and 2004. The stimulus for the changes in prescribing trends is not clear but may include increasing awareness of the 1997 BTS/SIGN guidelines and we expect that trends seen up to 2004 will have continued over the following years.
REFERENCES
Supplementary materials
web only appendix 94/1/16
Files in this Data Supplement:
Footnotes
Additional data are published online only at http://adc.bmj.com/content/vol94/issue1
Funding: Respiratory Research Limited provided funding for the database analyses reported here. Access to the GPRD database was provided by a grant from Schering Plough Ltd.
Competing interests: None.
Ethics approval: Obtained.
Linked Articles
- Atoms