Article Text

Abstract
Background Burosumab, an antifibroblast growth factor 23 monoclonal antibody, improves rickets severity, symptoms and growth in children with X-linked hypophosphataemia (XLH) followed up to 64 weeks in clinical trials. International dosing guidance recommends targeting normal serum phosphate concentration; however, some children may not achieve this despite maximal dosing. This study compares clinical outcomes in children with XLH on long-term burosumab treatment who achieved normal phosphate versus those who did not.
Methods Single-centre retrospective review of a large paediatric cohort with XLH treated with burosumab. We evaluated growth and biochemical markers of bone health in those who did compared with those who did not achieve normal plasma phosphate concentration.
Results Fifty-five children with XLH with median age of 11.7 (IQR 6.8–15.5) years were included. 27 (49%) had low plasma phosphate concentration, and 27 (49%) had normal phosphate after a median burosumab treatment duration of 3.3 (IQR 2.6–3.7) years. 1 (2%) did not have a recent phosphate level recorded. No difference in growth was found between normal and abnormal phosphate groups (p=0.9).
Conclusions Young children with XLH experience sustained growth on long-term burosumab treatment, although without normal plasma phosphate concentration in many. Consideration should be made to changing burosumab dosing recommendations to target normalisation of alkaline phosphatase, as opposed to plasma phosphate concentration.
- growth
- nephrology
- endocrinology
- genetics
- paediatrics
Data availability statement
Data are available upon reasonable request. Anonymised data available upon reasonable request to the authors.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Burosumab is a monoclonal antibody that is being used to treat X-linked hypophosphataemia.
Current European guidelines recommend titrating to low–normal values of phosphate.
WHAT THIS STUDY ADDS
Long-term data supporting growth if treated with burosumab, irrespective of recent phosphate level.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Treatment guidelines on plasma phosphate targets for burosumab dosing may need to be reconsidered.
Background
X-linked hypophosphataemia (XLH) is the most common heritable cause of rickets. Girls and boys are affected through X-linked dominant inheritance of loss of function variants in PHEX. This leads to dysregulation of fibroblast growth factor 23 (FGF-23), causing kidney tubular phosphate wasting and suppression of 1-alpha hydroxylation of vitamin D.1 2 Affected children experience growth faltering, severe rickets with bone deformities and pain and dental complications.1 3 4
Conventional treatment for XLH comprises oral phosphate and active vitamin D supplementation.5 Common treatment complications include gastrointestinal symptoms, hypercalcaemia, hypercalciuria and hyperparathyroidism.2
Burosumab is a recombinant human IgG1 monoclonal antibody that targets FGF-23. Clinical trials in adults and children with XLH demonstrated efficacy of burosumab in increasing serum phosphate levels, improving growth and physical function and reducing pain and the severity of rickets.6–9 Improved growth in children has been reported to 64 weeks’ follow-up6–8 10 with one article reporting up to 160 weeks.11 In 2018, burosumab was authorised by the European Medicines Agency and the US Food and Drug Administration for the treatment of XLH in children with evidence of bone disease aged 1 year and older.12 13
International consensus dosing guidance recommends starting burosumab at 0.8 mg/kg with subsequent dose titration to achieve fasting serum phosphate concentration at the lower end of the normal range, with maximum dose of 2.0 mg/kg (or 90 mg) every 2 weeks.14 15
In a large cohort of young children with XLH treated with burosumab, we observed that plasma phosphate concentration did not reach the normal range in some despite maximal dosing. We hypothesised that normalisation of plasma phosphate may not be the best treatment goal in this group. We therefore compared clinical outcomes for children on long-term burosumab treatment with normal versus abnormal plasma phosphate concentration.
Methods
Study population
We performed a retrospective cohort study of children with XLH treated at our centre between December 2014 and August 2022. Children under 18 years of age with a confirmed diagnosis of XLH undergoing treatment with burosumab were included.
Data collection
Demographic data including age, sex, PHEX variant and previous treatment prior to commencing burosumab were collated and then anonymised for analysis.
Clinical anthropometric and biochemical data were extracted at three time points: the commencement of burosumab treatment, approximately 1 year into treatment and at the patient’s most recent clinical review. Data included height (cm), burosumab dose (mg/kg), serum phosphate (PO4, mmol/L), serum calcium (Ca, mmol/L), parathyroid hormone (PTH, pmol/L), alkaline phosphatase (ALP, IU/L), 25-hydroxy vitamin D (nmol/L) and creatinine (Cr, µmol/L), urine phosphate (mmol/L) and urine Cr (mmol/L). Age-specific and sex-specific reference ranges were used throughout. Missing values were recorded as such in the data set. In our clinical practice, we aim to obtain blood tests as close to the next dose as possible, so as to obtain ‘trough’ levels.
Data analysis
Age-specific and sex-specific height Z-scores were calculated using the WHO AnthroPlus Software tool.16 To compare phosphate levels for different age groups, a standardised phosphate value was calculated by dividing the phosphate level by the lower limit of normal for the age group using reference ranges which were generally parsed in intervals of 2–3 years.17 Thus, a value of <1 indicates a phosphate level below the lower limit of normal. Similarly, to compare ALP levels, the value was divided by the upper limit of normal for the age/sex group.17 Thus, a value of >1 indicates an ALP level above the upper limit of normal. The reference ranges can be found in online supplemental table 1.
Supplemental material
Tubular reabsorption of phosphate (TRP, %) and the renal tubular maximum reabsorption rate of phosphate to glomerular filtration rate (TmP/GFR, mmol/L) were calculated from Payne’s equation using urine and serum phosphate and Cr values.18 TmP/GFR values were divided by the lower limit of normal for age/sex to give a standardised value.
Continuous data are reported as median (IQR) and categorical data as number (%). All statistical analyses were performed using Stata/IC V.15.
Comparison of anthropometric and biochemical markers at baseline and most recent review
As height measurements were not available for all individuals at baseline and most recent review, we assessed within-individual and group aggregate changes in height. Within-individual change was defined as the change in height (cm) and the change in height Z-score between that individual’s first and last review. Group-level data were analysed in aggregate and reported as median (IQR) as previously mentioned. We used the Wilcoxon signed-rank test as a non-parametric, paired, statistical hypothesis test to compare group values at baseline and at the most recent review.
Anthropometric and biochemical markers at most recent review, stratified by normal or abnormal serum phosphate level
To assess the importance of serum phosphate levels, we stratified the study population by normal or abnormal serum phosphate at the most recent review. We then performed a Mann-Whitney U test (unpaired, non-parametric) to check for significant differences between group heights. Values of plasma phosphate were defined as normal if they fell between the age-specific lower and upper limits of normal at the time of the most recent review.
Linear regression analysis
To determine whether phosphate level at the most recent review was associated with a difference in height Z-score, we performed a series of linear regression analyses. For all models, change in Z-score for height was modelled as the dependent variable, whereas phosphate level (mmol/L)±age at the commencement of treatment (years)±duration of treatment (years)±burosumab dose (mg/kg) were the independent variables. To ensure that the assumptions of linear regression were satisfied, we performed a Shapiro-Wilk test to confirm the normality of the change in Z-score data.
Anthropometric markers at most recent review, stratified by normal or abnormal serum ALP levels
To assess the importance of serum ALP levels, we also stratified the study population by low/normal or high-serum ALP levels at the most recent review. Values of serum ALP were defined as low/normal if they fell below the upper limit of normal (unit/L) at the time of the most recent review. We then performed a Mann-Whitney U test (unpaired, non-parametric) to review the differences between group heights.
Results
Population demographics
We identified 60 patients with XLH undergoing treatment with burosumab. Of these, five patients were excluded as either their initial treatment or current management was elsewhere.
Of the 55 (21 male and 34 female) patients included in the analysis, 52 have confirmed PHEX variants with the remaining three having positive family histories. Prior to commencing burosumab, 51 were confirmed to be receiving phosphate supplements and 54 were receiving vitamin D.
The median age at the commencement of burosumab treatment was 9.0 (IQR 3.9–11.0) years, with 17 patients under the age of 5 years. The age at the most recent clinical review was 11.7 (IQR 6.8–15.5) years. The median treatment duration with burosumab was 3.3 (IQR 2.6–3.7) years. The dose of burosumab at the most recent review was 1.17 (IQR 0.86–1.41) mg/kg per dose.
Long-term change in height
The age-adjusted and sex-adjusted Z-score for height at the commencement of burosumab treatment was −1.19 (IQR −2.32 to −0.61) or 122.9 cm (IQR 88.3–138.9) in absolute height. At the most recent clinical review, the Z-score for height was −1.07 (IQR −1.79 to −0.55) or 141.6 cm (IQR 115.6–155.4) (figure 1). Of the 50 individuals with data at both time points, the median within-individual change in height Z-score was 0.23 (IQR −0.11 to 0.51] or 18.2 cm (IQR 10.0–23.8) in absolute change in height (cm).

Box plot demonstrating height Z-scores at commencement of treatment, 1 year of treatment and most recent review. Height Z-score variance decreased with duration of treatment, with a trend towards more normal heights.
Differences in biochemistry
A comparison of group-level biochemical data at the onset of treatment and the most recent review demonstrated several statistically significant differences. Serum phosphate levels significantly increased (baseline: 0.81 mmol/L, most recent review: 1.06 mmol/L; p<0.01). Serum ALP levels significantly decreased (392 and 209 U/L, p<0.01), as did serum Ca levels (2.33 and 2.30 mmol/L, p<0.01).
Total 25-hydroxy-vitamin D levels were higher at the most recent review (68 and 88 nmol/L, p=0.06), though 31 of 55 were concomitantly prescribed vitamin D. TRP (83%–94%) and the renal tubular maximum reabsorption rate of phosphate to glomerular filtration rate (TmP/GFR, 0.57 and 1.01 mmol/L) were significantly higher (p<0.01) at most recent review.
Comparison of parameters stratified by phosphate level at most recent review
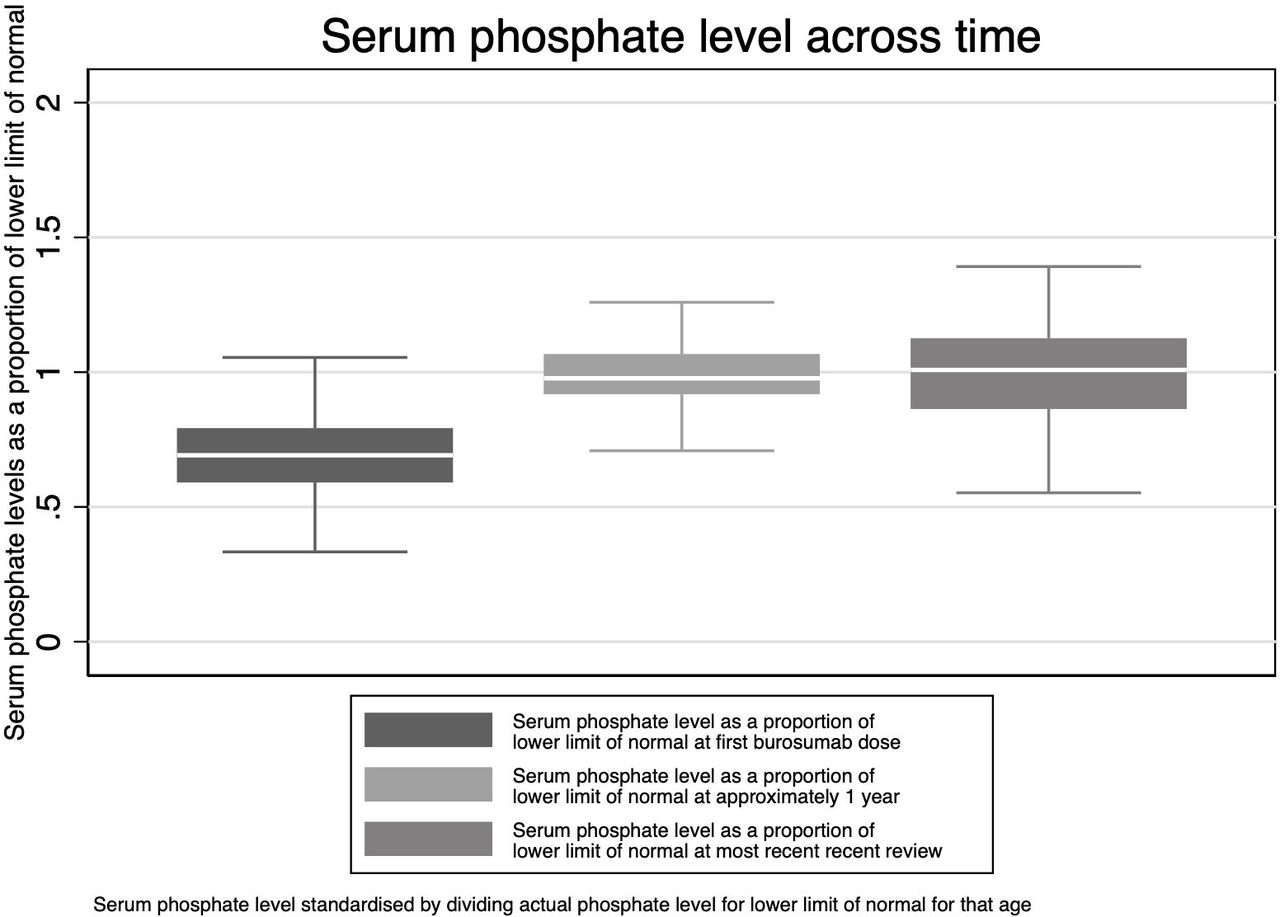
At most recent review, 27 patients (49%) had normal phosphate levels; 27 patients (49%) remained hypophosphataemic and one did not have a recorded value. This division between those with normal phosphate levels and those that were hypophosphataemic was similar at the 1-year review (figure 2), indicating that the most recent review was a valid time point for group stratification.

Box plot demonstrating serum phosphate level as a proportion of lower limit of normal (age-adjusted) at commencement of treatment, 1 year of treatment and at the most recent review. The plots demonstrate a tendency towards normalised phosphate levels with treatment.
At baseline, these two groups were not significantly different across anthropometric and biochemical measures, except for age, with the normal phosphate group older by 2.6 years (p=0.01). All other baseline characteristics were similar; these results are presented in table 1.
Comparison of anthropometric and biochemical markers at baseline and most recent clinical review based on most recent phosphate level
The change in height Z-score was not statistically significant nor was the duration of treatment; however, the dose of burosumab was higher in the hypophosphataemic group. A further comparison of various anthropometric and biochemical markers is demonstrated in figure 3, with the reference ranges for normal delineated with a black line.

Box plots of growth and biochemical markers at most recent review stratified by phosphate level. The results of a test of significance for these comparisons can be found in table 1.
Age at the commencement of treatment of burosumab
The age of commencement of burosumab treatment was negatively associated with height gain (figure 4). Linear regression analysis was performed, and this association remained significant (p<0.01) after adjustment for phosphate level at the most recent review, duration of burosumab treatment and dose of burosumab at the most recent review. By contrast, phosphate level, duration of treatment or burosumab dose was not significantly associated with change in height in any model.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Relationship between height Z-score and age at first dose of burosumab (years). The scatter plot shows that greater change in height Z-score is associated with commencing burosumab treatment at an earlier age.
Comparison of parameters stratified by ALP level at most recent review
A total of 41 patients recorded normal/low serum ALP levels at the most recent review with a median ALP level of 200 (161–273) IU/L or, as a proportion of the upper limit of normal, 0.53 (0.45–0.74). There was a median change in height Z-score of 0.28 (−0.09 to 0.51). Eleven patients recorded higher than normal ALP levels with a median value of 260 (190–388) IU/L or as a proportion of the upper limit of normal, 1.51 (1.12–2.90), with a change in height Z-score of 0.02 (−0.16 to 0.07). This was not statistically significant (p=0.56).
Discussion
Treatment of XLH with the FGF-23 monoclonal antibody, burosumab, has been shown to improve phosphate metabolism, decrease severity of rickets and improve growth and activity, as well as reduce pain.6 Due to the relatively recent availability of burosumab, current published experience is mostly limited to short follow-up periods (up to 64 weeks)6–8 10 with only one article recently published up to 160 weeks.11 This study shows longer-term data supporting a significant although modest change in height in children treated with regular (every 2 weeks) burosumab. Furthermore, growth did not differ between those who achieved normal plasma phosphate levels on burosumab treatment compared with those who did not. Of note, prior to the initiation of burosumab, the median height was higher and ALP lower than in previous studies, which may reflect better baseline disease control.6 7 This may have resulted in a relatively less marked clinical effect of burosumab and thereby impact the generalisability of the current study results.
Some of our data are in keeping with previous literature: no patient had a serum phosphate level above the upper limit of the normal range nor was there a notable change in serum Ca levels or serum PTH levels.6 There was a statistically significant decrease in serum ALP level. While there was a trend for better growth in those with normal/low ALP levels at the most recent review, the small number in the higher-than-normal level group precluded definitive analysis. These differences could potentially be explained by variations in pubertal timing or status by which a higher growth rate could be linked with lower ALP, so further studies could consider reviewing this. The finding of higher PTH activity and lower TRP in the normal phosphate group was surprising. The underlying cause of this cannot be determined from our data. Still, it may relate to less enteral Ca and phosphate absorption or a higher degree of bone deposition in the low-phosphate group. However, since the median PTH was in the normal range in both groups, it is difficult to ascribe specific physiological relevance to this difference.
European guidelines suggest targeting fasting serum levels of phosphate within the lower end of the normal reference range for age.15 In contrast, our data suggest that approximately half of our patients are currently not achieving normal phosphate levels, but despite this, they are still achieving good growth and biochemical parameters that are similar to those achieving normal phosphate levels and consistent with previous studies. This finding is in keeping with a previous study which demonstrated good growth on conventional treatment despite persistent hypophosphataemia.1 These data call into question whether normal phosphate levels are an appropriate treatment goal.15
Burosumab is an expensive drug and is administered subcutaneously, with many patients requiring multiple vials per dose, and there are subsequent, though largely well-tolerated adverse effects such as injection-site reactions. Those with lower phosphate levels were receiving higher doses of burosumab per kilogram of bodyweight. Our data question the clinical need for such higher dosing based on phosphate levels and may prompt reconsideration of current guidelines.
Early treatment with conventional therapy for children with XLH is associated with improved growth and skeletal outcomes.1 19 Burosumab improves outcomes both for younger and older children with XLH,19 but our current data support the importance of early treatment with burosumab to maximise height gain for children with XLH.
This retrospective cohort study has some limitations. Where values were age-specific and/or sex-specific, values were divided by the upper/lower limits of normal to compare groups. Z-scores would be an alternative method; however, we did not have the distribution nor SD to accurately calculate the value. Data were not complete for all patients as some clinical reviews coincided with the COVID-19 pandemic when outpatient face-to-face clinical interactions were reduced. Furthermore, regular X-rays and Thacher rickets scores were not performed, nor were data collected for dental complications, which would add to the previous literature. Our treatment strategy was guided by European guidelines to target normal serum phosphate concentration. Nevertheless, confounding cannot be excluded, given the retrospective real-world study design. However, this is a large cohort of patients with clinically significant findings which challenge the current recommendations.
Conclusions
The introduction of burosumab, the anti-FGF-23 monoclonal antibody for treatment of XLH, has benefitted children through improving phosphate homeostasis and decreasing the severity of rickets.6 This study demonstrates sustained growth with burosumab treatment in a real-world cohort of young children.
The data confirm that age of the commencement of burosumab is important to optimise growth. Newborns and infants of affected families or those with suspected XLH should be screened early to avoid delays in starting treatment.
The majority of children in this study did not achieve normal phosphate levels on burosumab with no apparent detriment to growth. These data call into question current recommendations to target low–normal serum phosphate levels as a treatment goal. The data suggest that normalisation of serum ALP may be a more clinically relevant goal for burosumab dose titration, but larger prospective studies are needed for confirmation.
Data availability statement
Data are available upon reasonable request. Anonymised data available upon reasonable request to the authors.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants, but local research ethics committee exempted this retrospective cohort study from informed consent due to the retrospective anonymised design. The need for informed consent was waived due to the retrospective nature of the anonymised data.
Acknowledgments
All research at Great Ormond Street Hospital NHS Foundation Trust and UCL Great Ormond Street Institute of Child Health is made possible by the NIHR Great Ormond Street Hospital Biomedical Research Centre. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @DocTimLindsay
Contributors All authors contributed to the study design. EYXW collated the data. EYXW and TAJL analysed the data. EYXW and WH drafted the manuscript. All authors reviewed and revised the final manuscript. WH is guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Linked Articles
- Highlights from this issue