Article Text

Abstract
Objective To study bronchoalveolar lavage (BAL) findings in various respiratory diseases in children in Kashmir India.
Design Prospective observational study.
Setting Paediatric department of the tertiary care hospital.
Patients Children of both genders from 1 month to 17 years of age
Intervention All studied patients underwent flexible bronchoscopy and BAL.
Outcome measure To observe the BAL findings in various respiratory diseases in the studied population.
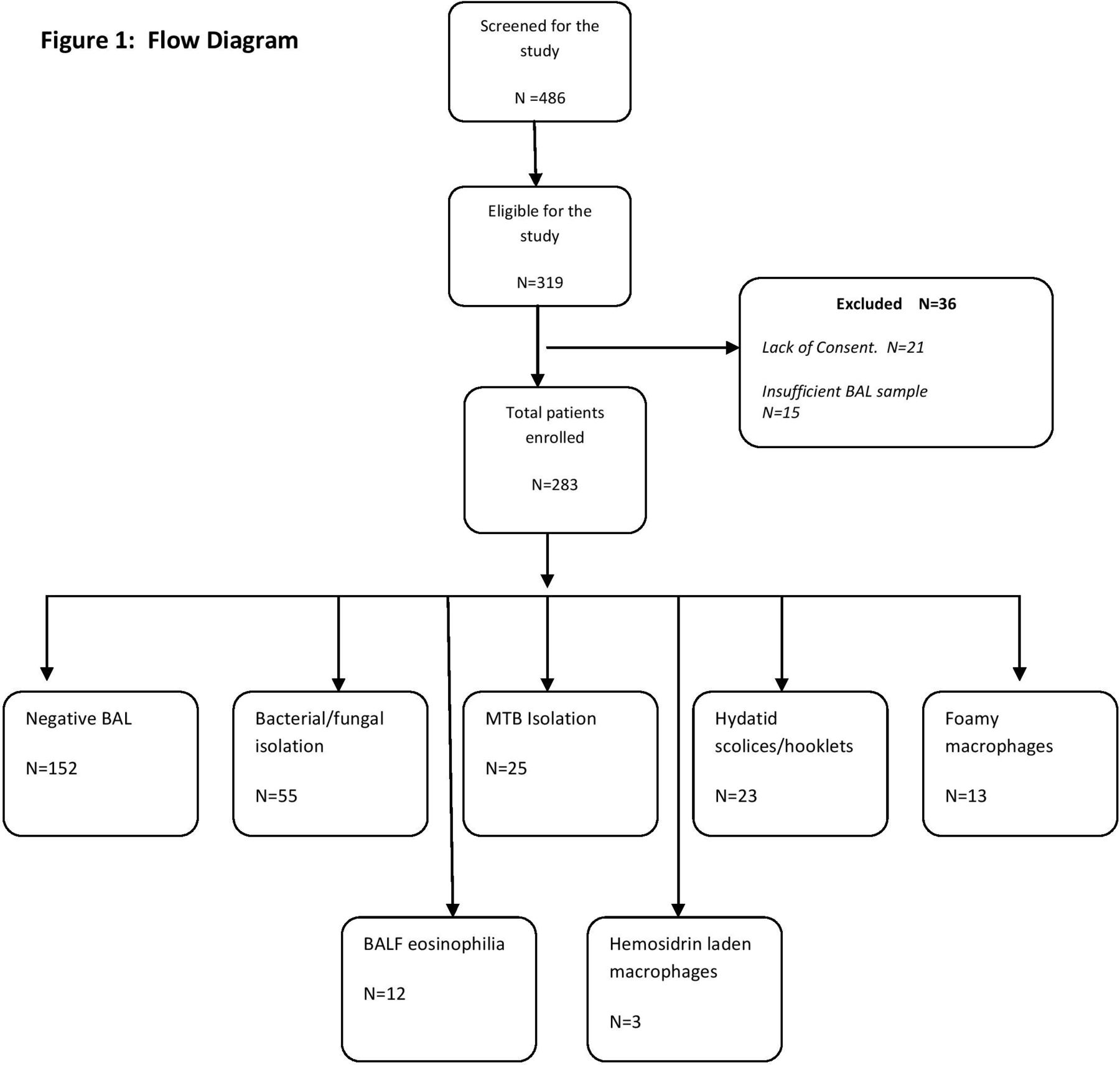
Results A total of 283 patients underwent BAL procedure. The positive BAL report was received in 131 (46%) patients. Out of these, 55 (42%) patients had positive BAL culture/ microscopy for different bacterial (50) and fungal species (Candida spp (3), Mucormycosis (1) and Aspergillus (1)). MTB was isolated in 25 (19%) patients. Twenty-three (17.5%) patients had bronchoalveolar lavage fluid (BALF) positive for pulmonary hydatidosis. Foamy macrophages were seen in 13 patients, significant eosinophilia in nine patients and hemosiderin-laden macrophages were seen in three patients.
Conclusion We found BALF a very useful sample for the evaluation of many infective and non-infective respiratory diseases in our region, which otherwise lacks high end diagnostics. 46% of our patients had some abnormalities in the BAL specimen. It provided us with valuable information regarding organism profile and drug sensitivity in case of lung infection. BALF analysis was also found useful in the diagnosis of some non-infective pulmonary disorders like acute eosinophilic pneumonia, aspiration syndromes and bronchial asthma.
- Respiratory Medicine
- Microbiology
Data availability statement
Data are available upon reasonable request.
Statistics from Altmetric.com
What is already known on this topic
Flexible bronchoscopy and bronchoalveolar lavage (BAL) is a useful investigation in many paediatric respiratory diseases.
What this study adds
BAL can help to diagnose various infective and non-infective lung diseases especially in low-income and middle-income countries where more sophisticated diagnostics are lacking.
BAL fluid analysis is a good diagnostic tool in pulmonary hydatidosis.
How this study might affect research, practice or policy
This study has provided audit of BAL findings in various paediatric respiratory diseases.
The study findings will help to improve diagnosis of various respiratory diseases in places with limited resources and lack of sophisticated diagnostic facilities.
Introduction
Flexible bronchoscopy (FB) is one of the important tools in the evaluation and management of various respiratory disorders of children.1 2 The diagnostic yield is enhanced further by the information obtained from the bronchoalveolar lavage (BAL). BAL has enormous diagnostic value in the spectrum of paediatric respiratory disorders ranging from the evaluation of complicated childhood pneumonia to diagnostically challenging parenchymal lung disorders.3–5 The ideal way of managing childhood pneumonia, especially in a high-risk population is pathogen-directed antimicrobial therapy. Since most of the children cannot produce sputum, the collection of bronchoalveolar lavage fluid (BALF) for the microbiological analysis has been found very useful in the management of complicated pneumonia. Several studies have documented the diagnostic utility of BAL in patients with complicated pneumonia, including patients with ventilator-associated pneumonia (VAP), non-resolving consolidation, pneumonia in immunocompromised and cystic fibrosis.6–8 BAL analysis is seldom diagnostic by itself in childhood interstitial lung diseases (ILDs), but BAL cell pattern results may support the diagnosis and/or narrow the differential diagnosis when considered in the context of the medical history, physical examination and radiological findings.5 The utility of the BAL in the evaluation of various respiratory disorders has more significance in low-income and middle-income countries like ours, as most of the advanced diagnostic tests either are lacking or lack expert interpretation.
Bronchoscopic BAL is safe procedure as well with very little complication rate and can be done safely under conscious sedation.6 The present study was conducted with the aim to study the role of bronchoscopic BALF analysis in various paediatric respiratory diseases especially in context of resource-constrained settings.
Materials and methods
This was a cross-sectional observational study conducted in a tertiary care hospital of northern India. It is a public hospital and is the one of the few places in the region where FB and BAL analysis is routinely done. The study was conducted from January 2016 to December 2020. A total of 486 patients underwent various bronchoscopy procedures during the study period. The procedure was done intranasally in non-intubated patients and via endotracheal tube in case of intubated patients. BAL was collected in a total of 283 patients. FB was performed by using Olympus BF-XP160F (Olympus Medical Systems, Japan) hybrid fibre-video bronchoscope. Vital parameters like pulse, oxygen saturation and ECG were continuously monitored using multichannel monitor (Edan IM80 Patient Monitoring Device). During the procedure, all patients received supplemental oxygen via nasal cannula. BAL was performed in patients based on clinical indication for the procedure. The total instilled volume was normal saline 3 mL/kg, administered in three divided doses in children weighing <20 kg and 20 mL portions in children weighing >20 kg. Contamination of BALF from upper airway secretions was prevented by gentle suction of excessive nasal and oral secretions before inserting the bronchoscope, flushing of oxygen through the suction channel while passing the bronchoscope through the upper airway, avoiding suctioning through the bronchoscope until the tip of the instrument is deep within the lungs. Furthermore, the BAL site was always preselected and it was performed as soon after entering the trachea as possible to minimise the chance of aspirating significant volumes of oral secretions into the specimen. BAL sample was sent for different investigations, including Gram staining, bacterial culture, fungal culture, total count, differential count, absolute eosinophil count, lipid-laden macrophages, special staining, acid-fast bacillus (AFB) and gene expert for Mycobacterium tuberculosis (MTB), depending on the clinical suspicion. The positive BAL report was defined as either of the following: growth of an organism with at least 105 colony-forming units from the BALF, detection of acid-fast bacilli either by Ziehl-Nelson stain and/or tuberculosis (TB) culture and/or by positive RTPCR, the presence of protoscolices and/or hooklets, of Echinococcus spp, presence of abnormal cell types and/or ratio of different cell types in the BALF, which includes ≥25% eosinophils or presence of lipid-laden macrophages or presence of hemosiderin laden macrophages. If the BALF analysis did not conform to the aforementioned case definition, then it was taken as a negative BAL report. A combination of midazolam and ketamine or propofol was used to achieve satisfactory sedation. A standardised data extraction form was used to obtain the demographic and clinical data which include patient age, gender, weight, provisional diagnosis, co-morbidities, procedure indication, procedural complication, bronchoscopy findings, BAL report etc. Finally, the diagnostic value of the BAL was assessed in our studied population.
Statistical analysis was performed using SPSS V.20. Parametric data are expressed as mean±SD and non-parametric test as median (IQR). Categorical variables are presented as percentages.
Results
A total of 486 bronchoscopy procedures were performed during the study interval. BAL was taken from 319 patients. A total of 283 patients were included in the study. Figure 1 describes the study flow and the reasons for exclusion. The age of patients ranged from one Mo to 17 Y with a median (IQR) age of 34 (57) months. The median (IQR) weight of the enrolled patients was 14 (7.5) kg with a slightly higher female preponderance (52.3%). The common indications for bronchoscopy and BAL were suspected pulmonary TB (88), suspected hydatid lung disease (55), cystic fibrosis (37), ventilator associated pneumonia (28), non-resolving pneumonia (27), recurrent wheeze (18), suspected recurrent aspiration (10), chronic cough (9), recurrent hemoptysis (5), suspected ILD (5) and persistent pneumonia in a type 1 patient with diabetes (1). The positive BAL report was received in 131 (46%) patients. Out of these, 55 (42%) patients had positive BAL culture/microscopy for different bacterial (50) and fungal species (Candida spp (3), mucormycosis (1) and Aspergillus (1)). MTB was isolated in 25 (19%) patients. Twenty-three (17.5%) patients had BALF positive for pulmonary hydatidosis (figure 2). Foamy macrophages were seen in 13 patients, and eosinophils were seen n BALF in 12 patients. However, significant eosinophilia, defined as an eosinophil count of ≥25%, was seen in nine patients. Hemosiderin-laden macrophages were seen in three patients. Antibiotics were modified in 40 of 50 patients as per sensitivity report. All patients with MTB isolates in the BALF were put on antitubercular medication. Twenty-one patients with positive BALF for hydatid cyst were subjected to the surgical intervention. Table 1 shows the organism profile of BALF. As seen in table 1, the most common bacterial species that was grown from the BALF was Pseudomonas aeruginosa. All these patients were known cases of cystic fibrosis. Polymicrobial growth was observed in seven (5.3%) patients.

Flow diagram. BAL, bronchoalveolar lavage; BALF, bronchoalveolar lavage fluid; MTB, mycobacterial tuberculosis.

{kind=link}
{kind=link}
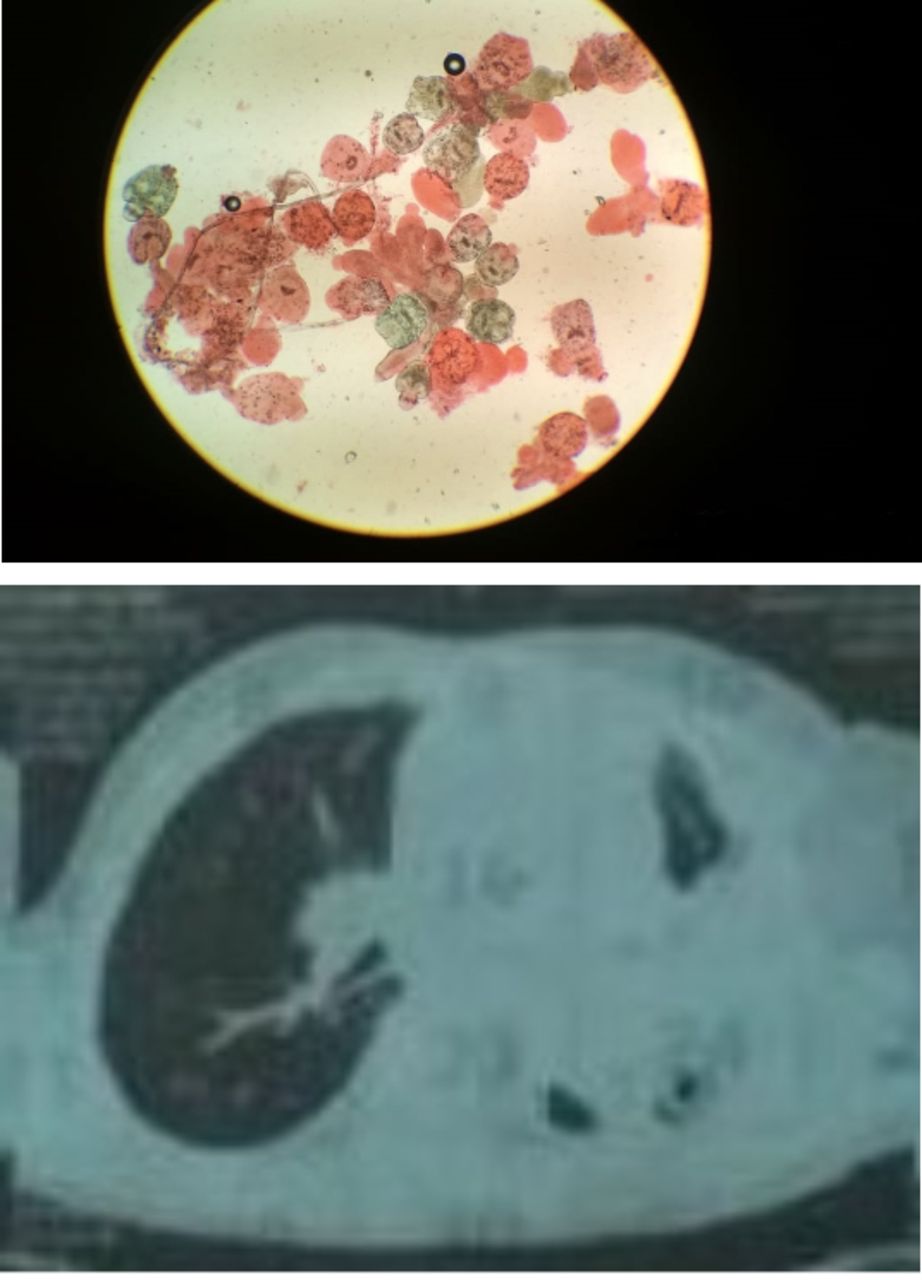
CT of the chest with collapse consolidation of the left lung and H&E staining of the bronchoalveolar lavage fluid for protoscolices.
Organism profile of the bronchoalveolar lavage fluid (N=103)
Discussion
We found that 131 patients out of 283 had positive BAL findings; this included 55 patients with bacterial and fungal isolation, 25 patients with pulmonary TB and 23 patients with BALF suggestive of pulmonary hydatid disease. Similarly foamy macrophages were seen in 13 patients, eosinophilia in 12 patients and hemosiderin-laden macrophages in three patients.
FB is a valuable tool to evaluate various paediatric airway diseases.1 BAL samples collected from the lower airways can be subjected to routine microbiological, cytological, and various advanced molecular and flow cytometric tests to diagnose the underlying disorder.9 Special staining of BALF, like Oil red O staining for lipid-laden macrophages, H&E stain for suspected hydatid disease, periodic acid–Schiff staining for pulmonary alveolar proteinosis and Prussian blue stain for hemosiderin-laden macrophages, has further expanded the role of BAL in the evaluation of paediatric lung diseases.10–12 Emerging investigations like ratio of CD4:CD8-positive cells in BAL may be helpful in diagnosing diseases like hypersensitivity pneumonitis and sarcoidosis.13
We collected BAL in 88 patients with suspected pulmonary TB. MTB was isolated in 15 patients from this subgroup. In all these 15 patients, prior gastric aspirate for MTB was negative. BAL was also positive for MTB in four patients with non-resolving pneumonia and two patients with chronic cough. Many studies have confirmed the superiority of BALF for the diagnosis of suspected TB in children.7 8 It is more sensitive than gastric aspirate or posterior pharyngeal specimen.4
The second most common indication for BAL collection in our study cohort was suspected hydatid lung disease. Hydatid disease is a zoonotic disease and is very common in this part of the world.14 The standard confirmatory test for pulmonary hydatid disease is histopathological examination of the surgical specimen. CT scan of the chest is the most commonly employed diagnostic test for such condition in low-income countries. It has excellent sensitivity in uncomplicated hydatid lung disease; however, in case of infected or ruptured pulmonary hydatid disease, sensitivity is variably reduced. Direct cyst aspiration with subsequent analysis or positron emission tomography is another investigation in case the CT findings are non-confirmatory.15 In our study cohort, 55 patients had suspected hydatid cyst lung based on chest CT findings. BAL analysis for the cyst membrane and protoscolices helped us to firmly confirm the disease in 18 of our patients. Bronchoscopy and staining of BAL has been found useful in this condition, especially in case of the ruptured hydatid cysts, infected and centrally located cysts.9 10
Cystic fibrosis, VAP and non-resolving pneumonia were also common reasons for the BAL collection in our study cohort. All 37 patients with cystic fibrosis in our study cohort initially underwent culture of oropharyngeal (OP) swab or sputum culture at the time of pulmonary exacerbation. Twenty-three patients showed nil growth of organisms. In eight patients, despite growth of an organism, antibiotic treatment did not improve the pulmonary exacerbation. Six patients had growth of mixed flora. Bronchoscopic BAL culture was positive in 15 patients. P. aeruginosa was the most frequently isolated organism, and antipseudomonasal antibiotics were started in all these patients. The culture of the expectorated sputum is considered the ‘gold standard’ for older children. For infants and other non-expectorating patients, an OP swab is the usual respiratory sample.11 The use of molecular assays has markedly increased the isolation of punitive organisms from these samples. However, such techniques are not available in our set-up. BAL culture provides a very useful option in case upper airway cultures are uninformative as it has better sensitivity than OP swabs.13 Bronchoscopy with BAL should be considered in patients with uninformative OP culture or poor response to antibiotics directed towards pathogens isolated from OP swabs.13 The proportion of positive BAL for different organisms was higher in patients with VAP (18/28). Mostly these patients grew Acinetobacter baumanii, Staphylococcus aureus and Klebsiella spp. Quantitative BAL culture in patients with VAP has been found a useful investigation in early diagnosis of VAP and for its optimal management.16 In a study by Riaz et al,17 the use of quantitative culture of BAL was found useful for the accurate diagnosis of VAP and limiting the unnecessary use of antibiotics.
We enrolled 27 (9.5%) cases of non-resolving pneumonia. The BALF analysis in this subgroup revealed the growth of organisms in seven patients, MTB isolates in four patients and the presence of protoscolices/hooklets in three patients. Non-resolving pneumonia is a common entity in hospital practice. Aetiology of non-resolving pneumonia is varied. In low-income countries like India, many of these children get empirical antitubercular therapy that imposes a threat of drug resistance. It is important to identify a cause for proper management. The diagnostic tests available for the evaluation of the aforementioned condition in our context are chest- X-ray, CT scan, sputum for MTB and spirometry. Bronchoscopy in this subgroup can improve case management and can rule out other causes of non-resolving pneumonia like foreign body aspiration, hydatid lung disease and bronchomalacia.3
BAL is also a useful investigation in immune deficient patients, in these patients’ pneumonia may be due to unusual organisms. In our cohort, based on bronchoscopic findings and wet mount of BAL sample, a case of pulmonary mucormycosis was diagnosed in a 13-year-old child with type 1 diabetes mellitus who presented with non-resolving pneumonia. BAL in immune-deficient patients should always be considered in case of unusual pulmonary presentation and/or non-resolving/rapidly progressive pneumonia.14
The main limitation of our study is that some advanced investigations were not conducted in the BALF like viral cultures, PCR analysis, CD4, CD8 count and BioFire microbiological study, which could have improved the sensitivity of BALF much further.18
Conclusion
We found 46% of patients had some abnormalities in the BAL specimen. It provided us valuable information regarding organism profile and drug sensitivity in case of the lung infection. BALF analysis has proven important diagnostic modality for the evaluation of many infective and non-infective respiratory diseases in the context of limited sophisticated diagnostic modalities available.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by DRB SKIMSNO SIMS/152/12/279. The participants gave informed consent to participate in the study before taking part.
References
Footnotes
Contributors JIB and ZMT conceived the idea of the study and wrote the manuscript; JIB and THS were involved in the sample collection; IAQ conducted the data analysis; BAC supervised the implementation of the study and contributed to the writing of the manuscript. JIB is guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.