Article Text

Abstract
Aims To determine reference values for oxygen saturation (SpO2) among healthy children younger than 5 years living at moderately high altitude in Papua New Guinea and to determine other factors that influence oxygen saturation levels.
Methods 266 well children living at 1810–2630 m above sea level were examined during immunisation clinic visits, and SpO2 was measured by pulse oximetry. Potential risk factors for hypoxaemia were recorded and analysed by multivariable analysis.
Results The median SpO2 was 95% (IQR 93%–97%), with a normal range of 89%–99% (2.5–97.5 centiles). On multivariable analysis, younger children, children of parents who smoked, those asleep and babies carried in bilums, a traditional carry bag made of wool or string, had significantly lower SpO2.
Conclusion The reference range for healthy children living in the highlands of Papua New Guinea was established. Besides altitude, other factors are associated with lower SpO2. Some higher-risk infants (preterm, very low birth weight, recurrent acute lower respiratory infection or chronic respiratory problem) may be more prone to hypoxaemia if they have additive risk factors: if parents smoke or they are allowed to sleep a bilum, as their baseline oxygen saturation may be significantly lower, or their respiratory drive or respiratory function is impaired. These findings need further research to determine the clinical importance.
- respiratory
- physiology
Data availability statement
Data are available upon request
Statistics from Altmetric.com
What is already known on this topic?
Oxygen saturation is lower at high altitude and in youngerinfants.
What this study adds?
At 1800–2600 m above sea level, the normal range of oxygen saturation is 95% (IQR 93%–97% and third centile 90%) and is lower at younger ages and when asleep.
In Papua New Guinea, infants carried in bilums (a traditional bag made of wool or string) and infants whose parents smoked had significantly lower baseline oxygen saturation, and may be more at risk of hypoxaemia under certain circumstances.
There have been reports of sudden unexpected deaths in infants sleeping in some types of bilums, and the design of these may need to be considered to ensure adequate ventilation.
Introduction
Pneumonia and other acute lower respiratory infections are the the most common cause of childhood admission to the hospital and deaths in Papua New Guinea.1 Hypoxaemia is the most commonly recognised complication and risk factor for death, and hypoxaemia seems to be more severe and prolonged in some settings, especially in the highlands regions.2 Pulse oximetry has been a great advance in patient management, offering non-invasive estimation of arterial oxygen saturation. Pulse oximetry has become a common practice in a variety of clinical situations and is now often part of standard patient observations.
A study done in four countries from 2017 to 2018 involving 1570 children living in altitudes ranging up to 4300 m showed that WHO thresholds for fast breathing and hypoxaemia overlap with respiratory rate and SpO2 values that are normal for children at higher altitudes. Potentially, use of WHO definitions for fast breathing could result in misdiagnosis of pneumonia in children who live at moderate to high altitudes and show acute respiratory signs, and the same may be true for hypoxaemia.3
Enga Province is in highlands of Papua New Guinea, and its major township of Wabag: situated at a longitude of 143 and a latitude of −5.5, and 2630 m above sea level.4 Clinics are conducted in villages at 1810–2630 m above sea level in a radius up to 13 km from the hospital and Wabag town. The population of Wabag town and district is 73 649 people (2011 census). Enga Hospital, in Wabag town, sees more than 100 sick children a day, and pneumonia is the most common reason for hospital presentation and admission. In 2019, Enga Hospital admitted 395 children with pneumonia, having four deaths with a case fatality rate (CFR) of 1%, and children with WHO-defined severe pneumonia had a CFR of 2.9%.5 In comparison to past years, the CFR of severe pneumonia has reduced. One reason for this is the introduction of pulse oximetry and better oxygen systems. It is thus recommended by the National Department of Health and Paediatric Society of Papua New Guinea that all hospitals ensure that there is regular clinical monitoring, including the use of pulse oximetry.5
Understanding the reference ranges of oxygen saturation in healthy children at a given high altitude is of clinical significance to prevent a misleading classification of hypoxaemia or severe pneumonia in a child with a lower respiratory tract infection. Lack of clarification on this could result in unnecessary admissions, inappropriate use of antibiotics and the use of oxygen, a resource to be carefully managed in settings where resources are limited. The dilemma of discharging inpatients while they have a lower SpO2, despite showing minimal signs of respiratory distress, is faced daily in some settings; this may prolong length of hospital stay, leading to unnecessary overcrowding in hospitals where bed spacing is limited.
Sudden unexpected death in infancy (SUDI) is poorly recognised and studied in developing countries, yet the risk factors for SUDI are common, and many unexplained infant deaths occur.6 SUDI has been closely linked to sleeping position and type of bedding.7 8 In Papua New Guinea, it is common for mothers to use a bilum to carry and hold their sleeping baby. A bilum is a bag made of string or wool, or traditionally the bark of atree, carried slung behind from the mother’s head and capable of carrying loads of considerable weight (figures 1 and 2). In the coastal areas, bilums are made from string, with an open weave, and in the highlands, bilums are more commonly made of wool, and the weave is tighter. We have noted three babies in the last 3 years being found dead in bilums in Enga Province: brief case vignettes are in the box 1.
Cases of sudden unexpected death in infancy in Enga Province, Papua New Guinea
2018, sudden death of a healthy, well-nourished 5-month-old female infant found dead in her baby bilum. One month previously, she was admitted to the ward with moderate pneumonia and had been discharged well. On the day of her death, she was irritable, crying a lot, so she was breast fed by her mother who carried her in the bilum and hung the bilum in a tree. The parents blamed the death on sorcery.
2019, death of an 8-month-old girl. She had cough and shortness of breath, which worsened overnight. Her mother brought her to hospital early the next day carried in her bilum. She died on the way.
2019, death of a 3-month-old girl who was brought to a district health centre. She was a second twin and preterm, and had a previous admission for pneumonia but was considered to have recovered. With her other twin, she was brought for their third vaccines. She was irritable afterwards. The mother tried breast feeding and then carried her in the bilum and swayed her around in an attempt to calm her. She was found dead in her bilum. The family blamed the health centre and the vaccines.

Mother with baby in bilum, Enga Province, Papua New Guinea (with kind permission).

Baby in an open bilum (with kind permission).
We conducted this study to determine the reference range for normal SpO2 among children at different ages, and we sought to understand if the oxygen saturation was affected by sleep state, being nursed in a bilum, parental smoking and household cooking smoke.
Methods
A descriptive observational study was conducted from May to July 2020, linked to the well-child clinic vaccination programme at Enga Provincial Hospital.
A total of 304 children were initially recruited, but 38 children were ineligible, leaving 266 healthy children from 1 to 60 completed months recruited. The recruitment of participants took place in Enga Provincial Hospital well-baby clinic and in five other clinics in villages in Wabag district: Kwimas (2380 m), Yokomanda (1960 m), Birip (1830 m), Akom (1810 m) and Rakamanda (1920 m). The participating children and their mothers were lifetime residents of Wabag district, and almost all were native Engan. Enrolment was sorted into five age groups: 1–3, 4–6, 7–12, 13–24 and 25–60 months. We included healthy children who had no known airway, pulmonary or cardiac problems. Children were excluded based on the following: irritable, crying or uncooperative children such that valid pulse oximetry readings were not possible; history of chronic illness like pulmonary tuberculosis, hyperactive airway disease or asthma, congenital heart disease, severe malnutrition; history of respiratory infection (pneumonia and bronchiolitis) in the last 2 months; and history of prematurity, low birth weight or past hospital admission as a neonate. From these criteria, 38 children were excluded, 2 with a history of neonatal admission for low birth weight, 3 siblings who showed signs of tuberculosis during screening and were sent to the hospital for further assessment, 4 with incomplete data, 12 infants who were too uncooperative for a steady-state oximetry reading, 3 who had been admitted within the past 2 months and 14 children who did not have a proper age record or in whom the date of birth was uncertain.
Pulse oximetry readings were obtained for each child prior to vaccination using a handheld Lifebox pulse oximeter, model number AH-M1 (www.lifebox.org). These oximeters have been validated and met the US Food and Drug Administration (FDA) requirements of precision and reliability.9 A paediatric or neonatal transducer appropriate to age was placed on the index finger, thumb or large toe of each subject. For the saturation of oxygen to be considered valid and recorded, the oximeter had to track the peripheral pulse for at least 30 s, giving a regular pulse rate and waveform.
Further information recorded included birth history, immunisation status, the age of weaning, parents’ smoking habits, open fireplace in home for cooking and medical history.
During the time of examination, observations were made to explore factors that might contribute to a lower oxygen saturation apart from high altitude and age. While recording a subject’s SpO2, the child’s physiological state was not disturbed, and whether the child was sleeping or awake was noted. In addition, if the infant was brought in a bilum, we checked the SpO2 while in the bilum and noted whether the child was awake or asleep.
Statistical analysis
Data were entered into an Excel V.2016 spreadsheet and transferred into Epi Info V.7 and STATA V.16 for analyses. As the data had a non-normal distribution, medians and IQRs were calculated for all age groups and comparisons. The lower limit of normal for age was taken as the 2.5th centile. Wilcoxon rank-sum test was used to compare SpO2 between those with the characteristic and those without, and associated factors with low SpO2 were further explored by multivariable regression analysis.
Results
Data from 266 children were analysed. The median age was 14 months (IQR 4–31 months); 124 were female and 142 were male. Table 1 shows characteristics of the study population, the potential risk factors that were assessed and the median values of subjects exposed or not exposed to these factors.
Subject characteristics and oxygen saturation
The median SpO2 was 95 (IQR 93–97), with a normal range of 89%–99% (2.5–97.5 centiles). Median values, IQRs and 2.5th centiles for each age group are summarised in table 2.
Oxygen saturation by age categories
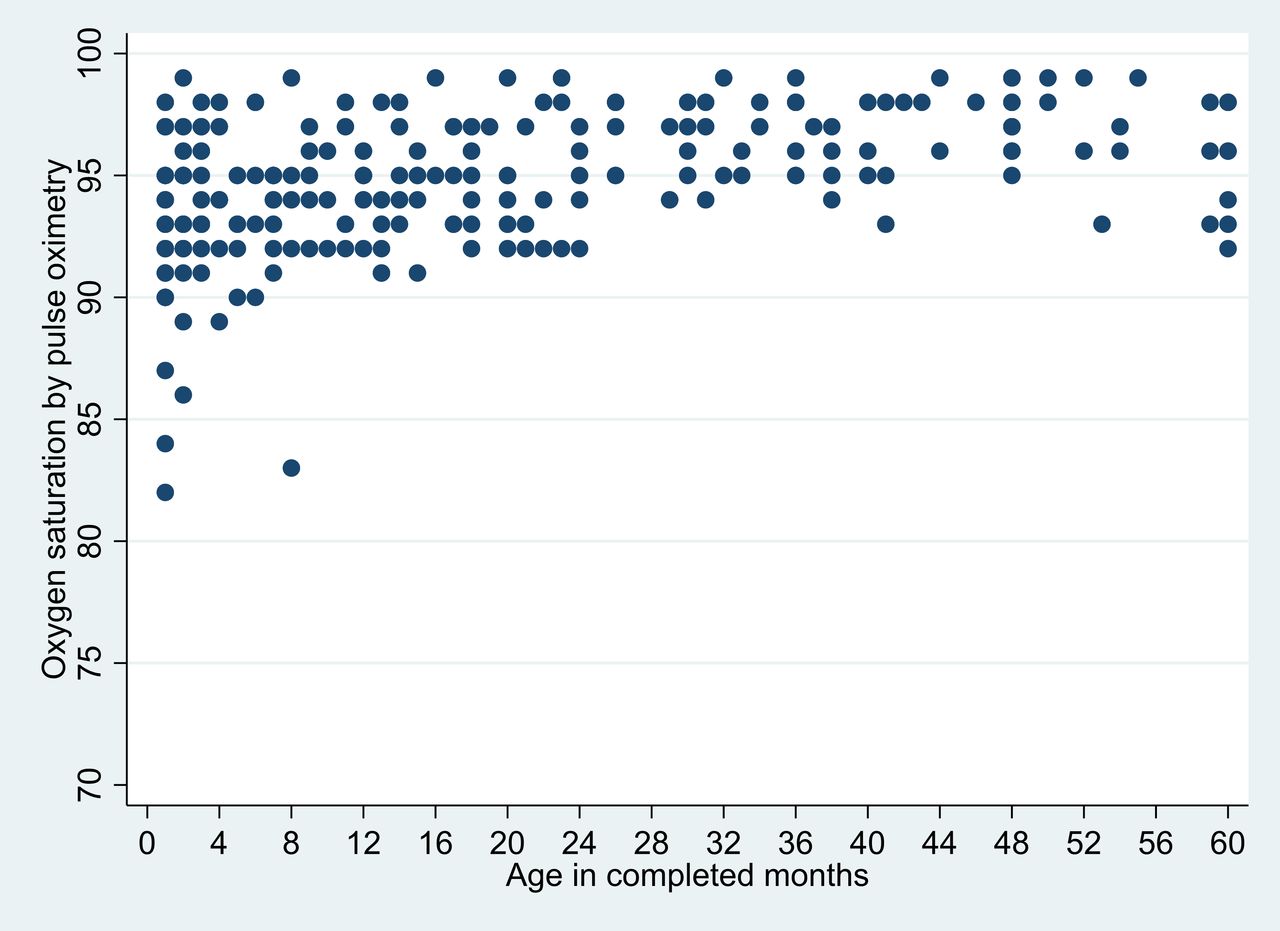
The median values for oxygen saturation in younger children was statistically lower than those in the older age groups. Figure 3 shows a scatter graph of SpO2 against months. The significant age gradient extended beyond early and late infancy. For example, children between 1 and 2 years of age had a small but significantly lower SpO2 than children over 2 years of age: 94% (92%–95%) vs 97% (95%–98%) (p<0.0001) (table 2).

{kind=link}
{kind=link}
{kind=link}
Oxygen saturation (%) by age.
Infants asleep (n=35) had a significantly lower SpO2 than those who were awake: 93 (91–96) vs 95 (93–97) (p<0.0001). Infants who were in bilums (n=55) had significantly lower SpO2 than those not in bilums: 93 (92–95) vs 95 (94–97) (p<0.0001).
Variables not associated with differences in oxygen saturation were the location of birth, any history of illness in the neonatal period, whether the parent reported a current cough, the child’s immunisation status, whether the infant was formula fed and the type of home fireplace.
In the multivariable analysis, age was the strongest independent factor influencing SpO2; also independently significantly affecting SpO2 were being in a bilum (p=0.011), parents smoking (p=0.011) and whether the infant was asleep (p=0.08) (table 3).
Multivariable analysis of risk factors for lower oxygen saturations
Discussion
This study established reference ranges for oxygen saturation at 2600 m above sea level in highlands Papua New Guinea and confirmed they are lower than the general referenced standards at sea level. This has been shown by previous studies.3 10–13 The threshold for giving oxygen recommended by WHO in pneumonia: SpO2 of <90% is appropriate for children over the age of 1 year, but in the 85 children below 6 months in this study living at 2600 m, the observed 2.5th centile for SpO2 was 84%. For reasons explained below it is still appropriate to give oxygen if the SpO2 <90% in unwell children with pneumonia at altitude, but this does overlap with the normal reference range.
The strongest factor influencing SpO2 at this altitude was young age. Infants have lower SpO2 for the following reasons: during the first year of life, some physiological compensations stimulated by low oxygen tension may not yet be developed; infants have comparatively less functional residual capacity than older children; and their smaller airways generate a higher airway resistance.14 In our study, the age gradient extended beyond early infancy; children between 1 and 2 years of age had a small but significantly lower SpO2 than children over 2 years of age. That sleeping was associated with a decrease in mean SpO2 has also been reported in previous studies.2 12 During sleep, there is mildly decreased functional residual capacity; the infant takes more frequent and shallow breaths. This may lead to pulmonary atelectasis, and some ventilation:perfusion mismatching leading to lower SpO2. Periodic breathing and sleep apnoea in young infants has been reported at 2500 and 3200 m above sea level in South America.15 16 High-altitude pulmonary oedema also occurs in children living above 1800 m, related to muscularisation of pulmonary arterioles and arteries and hypertrophy and dilatation of the right ventricle, with subsequent congestive right-sided heart failure.17–19 Children with even mild pulmonary hypertensive changes may have exacerbations if they develop a respiratory infection, and respond well to oxygen. This suggests that even if the apparent normal range of some age groups in the population is below the threshold of SpO2 90% for receiving oxygen, if a child has respiratory distress and an SpO2 of 90% or less, oxygen is likely to be of therapeutic benefit.
The clinical significance of our observations on infants being carried in bilums is uncertain, but some young infants may be at higher risk of hypoxaemia in some situations. We have noted the sudden unexpected deaths of three infants in the community in bilums in the last 3 years in Enga Province. In the highlands of Papua New Guinea, woollen baby bilums are tightly woven to keep the infant warm, but these may have inadequate space for ventilation. String woven bilums are mostly used in coastal areas; these are open weave with knots far apart and may provide better ventilation. There is now a trend in the highlands of weaving bilums like on the coast, still of wool, but leaving bigger space for better ventilation. Infants such as those who are preterm, have very low birth weight or who have recurrent viral lower respiratory infection may be at more risk of hypoxaemia if both are asleep and in a bilum. A variety of potentially unsafe sleeping environments have been identified as risk factors for sudden unexpected death in infants.8 While infants are generally supine in a bilum, airway obstruction, hypoxaemia or hypoventilation may occur if a young and high-risk infant is flexed in a bilum, especially during sleep. Some types of swaddling of some young infants had been shown to lower oxygen tension20; however, being carried in a bilum is not directly analogous to swaddling as in many traditional societies.21
We found a trend towards lower saturation if one or both parents smoke, and this is also a known risk for SUDI and lower respiratory drive.22–24 Thus, it is possible that sleep state, being in a bilum and parental smoking provide additive risks for high-risk infants in PNG, especially those at altitude where baseline oxygen saturations are lower, where periodic breathing may occur and where pulmonary hypertension may have a role.19 The clinical and public health significance of these observations and theories are uncertain but require further research.
Conclusion
This study provides a definition of normal SpO2 in a healthy population of children living at an altitude of 2600 m. Younger children have a lower mean SpO2 than older children living at this altitude, and this gradient continues beyond infancy. Sleep had a lowering effect on arterial oxygen saturation, and babies in bilums whether awake or asleep had lower SpO2 compared with other children. While the clinical significance of these are uncertain, some young babies may be more at risk of hypoxia and adverse events if asleep in a bilum and if parents also smoke, and this requires further research and public awareness.
Data availability statement
Data are available upon request
Ethics statements
Patient consent for publication
Ethics approval
Verbal informed consent was obtained from parents or guardians before examination and inclusion in the study. The study was approved by the ethics committee of the School of Medicine and Health Sciences, University of Papua New Guinea, in 2020, and the Enga Provincial Health Authority.
References
Footnotes
Contributors VB and TD designed the study, performed the data analysis and wrote the first drafts of the manuscript. VB recruited subjects and gathered the data. DP and RK assisted in the data collection. DP, TD and VJ supervised the study.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.