Article Text

Abstract
Objective Compare trends in coronary artery (CA) abnormality diagnoses to trends in adverse cardiac outcomes among American children with Kawasaki disease (KD) to assess the fit of detection of CA abnormalities to an established model of overdiagnosis.
Design Multicenter retrospective cohort.
Setting 48 US children’s hospitals in the Paediatric Health Information System database.
Participants Children <18 years receiving care for KD between 2000 and 2014.
Main outcome measures The main outcomes were rates of CA abnormality diagnoses and adverse cardiac outcomes, measured during a child’s incident KD visit and longitudinally at all subsequent visits to the same hospital, through December 2016. CA abnormalities were considered severe if long-term anticoagulation other than aspirin was prescribed. Trends were tested using mixed effects logistic regression, adjusting for patient demographics.
Results Among 17 809 children treated for KD, a CA abnormality was diagnosed in 1435 children (8%), including 1117 considered non-severe and 318 severe. The rate of non-severe CA abnormality diagnoses increased from 45 per 1000 patients with KD in 2000 to 81 per 1000 patients with KD in 2014, representing an adjusted 2.3-fold increased odds (95% CI 1.8 to 3.0) of diagnosis. There was no significant change in diagnoses of severe CA abnormalities. Adverse cardiac outcomes were stable over the study period at 19 per 1000 patients with KD (P=0.24 for trend).
Conclusions The rising rate of detection of non-severe CA abnormalities accompanied by an unchanging rate of adverse cardiac outcomes among American children with KD fits an overdiagnosis pattern.
- epidemiology
- health services research
- cardiology
Statistics from Altmetric.com
What is already known on this subject?
Increased detection of smaller, less clinically important forms of thyroid cancer and pulmonary emboli have been shown to be overdiagnosed in adults.
There are no studies that apply this overdiagnosis model to a paediatric condition.
What this study adds?
Diagnosis of coronary artery abnormalities among children with Kawasaki disease doubled over the study period, while the rate of adverse cardiac outcomes did not change.
The combination of increased diagnosis of coronary artery abnormalities without a change in adverse patient outcomes fits an overdiagnosis model.
Background
Overdiagnosis occurs when a patient is correctly diagnosed with an abnormality but will not experience net benefit as a result of detection of the abnormality (ie, the harms of detection outweigh the benefits).1 Therefore, contrary to errors in testing or cognition that lead to inaccurate diagnoses (like misdiagnosis and false positives), overdiagnosed patients truly have the detected condition.2 Persuasive arguments for overdiagnosis of thyroid cancer3 4 and pulmonary emboli (PE)5 have been reported among adult populations using a method that compares trends in disease detection to trends in a patient outcome related to that disease. For example, widespread use of CT pulmonary angiography in the late 1990s was associated with a nearly twofold increase in detection of PE, but mortality from PE remained largely unchanged over the same time period.6 Smaller, less clinically meaningful thromboses were likely increasingly detected with improved imaging resolution7; however, anticoagulation complications increased.6 This is not to say that all patients with PE were overdiagnosed. Rather, the focus is on the additional patients diagnosed beyond the prior baseline as a result of improved imaging technology. These additional patients did not have clinically important disease and likely experienced more harm than benefit as a result of their PE diagnosis.
While children are likely impacted by overdiagnosis,8 there are no studies using a similar model comparing disease trends to outcome trends to test for potential paediatric overdiagnosis. We hypothesised that coronary artery (CA) abnormalities diagnosed among children with Kawasaki disease (KD), an acute childhood vasculitis that is a leading cause of acquired heart disease,9 might fit the overdiagnosis model for the following reasons: (1) the US 2004 KD guideline recommended early and repetitive echocardiography at diagnosis, 2 and 8 weeks postdiagnosis and more often if abnormalities are noted,10 (2) the majority of detected CA abnormalities resolve within months of the acute KD illness11 and (3) the least severe forms of CA abnormalities appear to be increasingly diagnosed.12 13 The present study evaluates CA abnormalities in the context of a model testing for overdiagnosis by comparing the rate of CA abnormality diagnoses to the rate of adverse cardiac outcomes over time among American children with KD.
Methods
Study design and setting
We identified a retrospective cohort of children treated for KD using the Paediatric Health Information System (PHIS) database. The PHIS database provides de-identified information detailing hospital and patient demographic data, administrative data such as discharge diagnosis and procedure coding and detailed billing information including laboratory, imaging, pharmacy and supply charge data for patients cared for at 48 US stand-alone children’s hospitals, representing approximately 20% of all US paediatric hospitalisations. Patients are assigned a single identifier allowing longitudinal linkage of all visits within a single PHIS centre. Data for the present study were abstracted from emergency, inpatient or observation visits.
Participants
Patients <18 years admitted to a PHIS hospital between January 2000 and December 2014 with an International Classification of Diseases, Ninth Revision (ICD-9) discharge diagnosis code for KD (446.1) were eligible for inclusion. Children were excluded if they did not receive intravenous immunoglobulin (IVIG) during at least one of their KD hospitalisations, mirroring prior investigations using the PHIS database,14 or if they had an ICD-9 discharge diagnosis code for a severe congenital heart lesion (online Supplementary appendix 1) during any hospital encounter since birth.
Supplementary file 1
CA abnormalities
In lieu of specific imaging findings, which are not contained in PHIS, a CA abnormality outcome was assigned to patients with an ICD-9 discharge diagnosis code for a CA abnormality within 60 days of their index KD hospitalisation (online Supplementary appendix 2). Sixty days were chosen because the 2004 US KD guideline, in place during the study period, recommended echocardiography testing 6–8 weeks after the onset of KD symptoms, because new CA abnormalities are rare after this time among patients with normal echocardiography.10 CA abnormalities were considered severe if long-term anticoagulation (see the ‘Medications’ section below) was prescribed within 60 days of the index KD hospitalisation, as the 2004 US KD guideline recommended anticoagulation for large coronary artery aneurysms or multiple or complex aneurysms in the same vessel.10
Adverse cardiac outcomes
A composite adverse cardiac outcome measure included: mortality; ICD-9 codes for ischaemic heart disease, cardiac arrest, cardiogenic shock or arrest, cardiac conduction disorders or cardiomyopathy; ICD-9 procedure codes for stents, angioplasty, coronary artery bypass graft, heart transplant, cardiac assist devices or pacemakers; or hospital charges for thrombolytic therapy by intravenous infusion, CPR, cardioversion or defibrillation (online Supplementary appendix 3). Adverse cardiac outcomes were measured through December 2016. A crosswalk available from the Centres for Medicare and Medicaid Services15 was used to convert ICD-10 diagnosis and procedure codes after September 2015 (when the USA began using ICD-10 coding) to ICD-9 diagnosis and procedure codes. Potential follow-up time was measured as the difference between 2016 and the year of a patient’s index KD encounter.
Imaging
The number and timing of echocardiograms were determined using ICD-9 procedure codes (online Supplementary appendix 4) and hospital imaging charges for echocardiography. Time to first echocardiogram was calculated as the number of days between the index KD admission day and the first echocardiogram. Patients with a time to first echocardiogram >60 days were excluded from this measurement (n=174 patients, 1%) because these patients likely received an echocardiogram outside the hospital setting. ‘Other cardiac imaging’ included cardiac angiography, tomography and MRI (online Supplementary appendix 4).
Medications
Long-term anticoagulation was defined as a hospital charge for low molecular weight heparin (LMWH), warfarin or an antiplatelet agent (such as clopidogrel and dipyridamole). Our long-term anticoagulation definition did not include aspirin, because guidelines recommend aspirin for all patients with KD.10 16 Only systemically administered steroids were included and steroids charged to children with a concomitant diagnosis of ‘chronic obstructive pulmonary disease (ICD-9 490–496.XX)’ or ‘chronic lung disease (ICD-9 770.7)’ were not counted. Definitions for IVIG and ‘other immune-modulating medications’ are provided in the online Supplementary appendix 5. IVIG retreatment was defined as a second dose of IVIG ≥2 days after initial IVIG treatment.
Statistical analysis
Categorical variables were summarised with frequencies and percentages and continuous variables were summarised with median and IQR. Trends in outcomes were tested using mixed effects logistic or Poisson regression, for dichotomous or continuous count outcomes, respectively. Age, gender, insurance type (government, private or other), and race (non-Hispanic white, non-Hispanic black, Hispanic, Asian or other) were treated as fixed effects. Hospital site was treated as a random effect because compared with patients at other hospitals, patients at the same hospital are likely not completely independent. Data are presented as the OR or incidence rate ratio (IRR) of the change in an outcome over the 15-year study period. The primary analysis of adverse cardiac outcomes included all events through December 2016. However, to account for the possibility that longer follow-up time among patients diagnosed with KD in earlier years might bias the adverse cardiac outcome trend, we also conducted a sensitivity analysis guaranteeing equivalent follow-up time for each patient by using only adverse cardiac outcomes experienced within 2 years of a subject’s KD diagnosis. All analyses were performed using STATA V.14.
Results
Study population
Of 19 262 children diagnosed with KD at 48 children’s hospitals during the 15-year study period, 1453 children were excluded from the analysis: 1061 who did not receive IVIG during a KD hospitalisation and 392 for congenital heart disease. Over half of included children were male and 84% were <6 years of age (table 1).
Demographic characteristics of patients with Kawasaki disease (n=17 809)
CA abnormalities
A CA abnormality was detected in 1435 children (8%), including 1117 considered non-severe and 318 severe. The rate of CA abnormality diagnoses increased from 57 per 1000 patients with KD in 2000 to 104 per 1000 patients with KD in 2014, representing an adjusted 2.1-fold increased odds (95% CI 1.7 to 2.6) of diagnosis. As shown in figure 1, the rate of non-severe CA abnormality diagnoses increased from 45 per 1000 patients with KD in 2000 to 81 per 1000 patients with KD in 2014, representing an adjusted 2.3-fold increased odds (95% CI 1.8 to 3.0) of diagnosis. There was no significant change in diagnoses of severe CA abnormalities (figure 1, P=0.13 for trend).

Trends in the rate of severe and non-severe coronary artery abnormalities among children with Kawasaki disease, 2000–2014.
Adverse cardiac outcomes
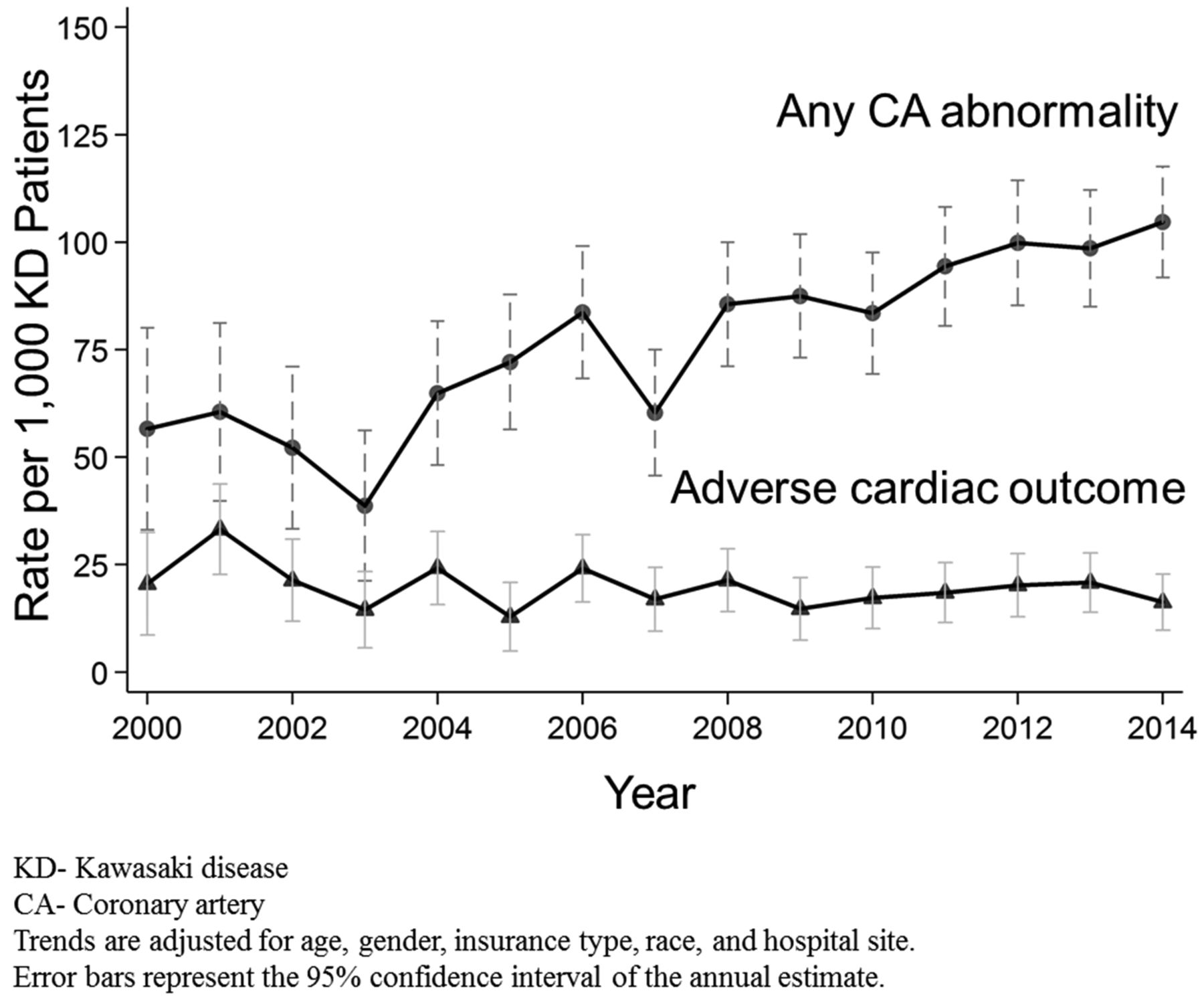
Despite a doubling of CA abnormalities, adverse cardiac outcomes for children with KD (figure 2) were stable over the study period at 19 per 1000 patients with KD (P=0.24 for trend) using all available follow-up time and 17 per 1000 patients with KD (P=0.89 for trend) when the analysis was restricted to only the first 2 years after KD diagnosis. Of the 342 children who experienced an adverse cardiac outcome (table 2), 86% did so within the first year of their KD diagnosis. Ischaemic heart disease and/or heart failure accounted for 62% of the adverse cardiac outcomes. Patients had a median potential follow-up time of 8 years (IQR 4–11 years).
{kind=link}
{kind=link}
Trends in the rate of any coronary artery abnormality and adverse cardiac outcomes among children with Kawasaki disease 2000–2014.
Percentage of each morbidity among patients who experienced an adverse cardiac outcome (n=342 patients)
Imaging
On average, 93% of children with KD received an echocardiogram during their index visit, with increasing odds over the study period (OR 2.3, 95% CI 1.8 to 3.0). Time to first echocardiogram (median 1 day, IQR 0–2 days) and total number of echocardiograms (median=3 echocardiograms/patient, IQR 1–3 echocardiograms) decreased (IRR 0.50, 95% CI 0.47 to 0.52 and IRR 0.54, 95% CI 0.52 to 0.56, respectively). The odds of exposure to other forms of cardiac imaging did not change (OR 1.4, 95% CI 0.9 to 2.2), but children were less likely to undergo cardiac catheterisation (OR 0.2, 95% CI 0.1 to 0.3).
Adjunctive medications
Children with KD were increasingly likely to receive multiple doses of IVIG and immune-modulating therapies (table 3). While there was no change in the proportion of children receiving anticoagulation as a whole, patients were increasingly provided LMWH as warfarin prescriptions declined.
Trends in exposure to adjunctive medications among children with Kawasaki disease, 2000–2014 (n=17 809)
Discussion
Among American children with KD, we found that the rate of CA abnormality diagnoses nearly doubled over the last 15 years, driven almost entirely by non-severe forms, with no measurable change in the rate of adverse cardiac outcomes. Considering these results in the context of existing adult overdiagnosis models and knowledge of CA abnormality epidemiology in children with KD, we evaluated the possibility that a portion of CA abnormalities might be overdiagnosed.
In adults, comparing the rate of detection of abnormalities to patient outcomes over time has been a successful method to demonstrate overdiagnosis of PE6 and thyroid cancers.3 4 Regarding the latter example, studies in the USA3 and Korea4 measured an increasing trend of thyroid cancer diagnoses over a defined time period with a stable rate of thyroid cancer mortality over the same time period. The overdiagnosis model was further supported by the fact that the increase was nearly completely due to a rise in small papillary cancers, a form known to be found incidentally in autopsies. Similar to these adult studies, we found increased diagnosis of non-severe forms of an abnormality (CA abnormalities), without a change in patient outcomes (major cardiac sequelae or death).
While our findings mirror those of adult overdiagnosis studies, important pieces to the puzzle remain. Insufficient follow-up periods and/or latent disease outcomes can result in lead time bias, which will temper any estimate of overdiagnosis.17 Children in the present cohort had at least 2 years of follow-up time, which covers the acute and subacute phases of KD illness during which the majority of adverse cardiac outcomes occur in childhood.18–20 However, a portion of these children will undoubtedly go on to experience cardiac events as adults, particularly those with large and multisite aneurysms.11 18 21 Given that our study found a rise in non-severe CA abnormalities in particular, the important question related to overdiagnosis potential is whether non-severe CA abnormalities place children at increased risk of adverse cardiac events in adulthood and whether abnormality detection in childhood reduces that risk. Unfortunately, the existing body of literature does not provide a clear answer. Epidemiological studies following KD children into adulthood have not shown that small CA abnormalities lead to adverse cardiac events in adulthood, though their follow-up period is limited.11 22 Surrogate marker data among adults with a history of KD are conflicting: some studies report late calcification,23 arterial wall thickening,24 flow abnormalities25 and worse coronary vascular health26 only among those with a history of larger CA abnormalities, while others found that even children without documented CA abnormalities demonstrate long-term surrogate marker dysfunction.27 28 For these reasons, it will be important to re-evaluate our findings as more is learnt from long-term follow-up of adults diagnosed with non-severe CA abnormalities in childhood.
The implications of our results require judicious consideration. Foremost, this study examines overdiagnosis of CA abnormalities, but should not be interpreted as suggesting overdiagnosis of KD itself as early diagnosis of KD and treatment with IVIG is highly efficacious.29 30 Second, given the uncertainty about cardiac risk in adulthood, it would be premature to alter CA diagnostic strategies and disease definitions presently. Rather, further research aimed at understanding ideal timing and frequency of echocardiography, optimal thresholds for abnormal CA dimensions and the amount of increased cardiac risk that specific lesions portend into adulthood are needed. Such research efforts are imperative because, much like adults with overdiagnosed PE who experienced bleeding complications from anticoagulation, it is possible that diagnosis of non-severe CA abnormalities could have unintended consequences. For example, knowledge of these abnormalities could lead to parental perception of their child’s vulnerability31 and increased exposure to sedation (for further echocardiography), which has been linked to small decreases in future neurocognitive performance.32 33
Our study has important limitations. The degree to which our results might generalise to non-tertiary centres or other countries is unknown. While treatment of complications related to KD generally requires the services of a tertiary children’s hospital, patients could have experienced adverse cardiac outcomes, received testing (such as echocardiogram) or been prescribed medications outside of the children’s hospital of their index KD visit (in an ambulatory or other hospital setting), which would not have been captured in the PHIS database. Differential misclassification of diagnoses, exposures or outcomes from 1 year to the next in the database would bias the observed trends. Finally, because we relied on prescription of long-term anticoagulation as a surrogate measure of CA abnormality severity, misclassification is possible if patients received long-term anticoagulation for a different reason.
Conclusion
Trends in diagnosis of CA abnormalities among US children with KD mirror an established adult model of overdiagnosis. Improved understanding of which CA aberrations are clinically meaningful is needed to maximise benefit and minimise harm for these children.
References
Footnotes
Contributors ERC designed the study, wrote the statistical analysis plan, cleaned and analysed the data and drafted and revised the paper. He is the guarantor. JW cleaned and analysed the data and revised the paper. SLB and RS designed the study and revised the paper.
Funding None declared.
Competing interests None declared.
Ethics approval University of Utah.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Editorial