Article Text

Abstract
In recent years, most of the focus on improving the quality of paediatric care in low-income countries has been on improving primary care using the Integrated Management of Childhood Illness, and improving triage and emergency treatment in hospitals aimed at reducing deaths in the first 24 hours. There has been little attention paid to improving the quality of care for children with chronic or complex diseases. Children with complicated forms of tuberculosis (TB), including central nervous system and chronic pulmonary TB, provide examples of acute and chronic multisystem paediatric illnesses that commonly present to district-level and second-level referral hospitals in low-income countries. The care of these children requires a holistic clinical and continuous quality improvement approach. This includes timely decisions on the commencement of treatment often when diagnoses are not certain, identification and management of acute respiratory, neurological and nutritional complications, identification and treatment of comorbidities, supportive care, systematic monitoring of treatment and progress, rehabilitation, psychological support, ensuring adherence, and safe transition to community care. New diagnostics and imaging can assist this, but meticulous attention to clinical detail at the bedside and having a clear plan for all aspects of care that is communicated well to staff and families are essential for good outcomes. The care is multidimensional: biomedical, rehabilitative, social and economic, and multidisciplinary: medical, nursing and allied health. In the era of the Sustainable Development Goals, approaches to these dimensions of healthcare are needed within the reach of the poorest people who access district hospitals in low-income countries.
- tuberculosis
- quality of care
- low and middle income countries
- meningitis
- chronic lung disease
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
In low-income countries central nervous system (CNS) manifestations of tuberculosis (TB) are common, and many children with pulmonary TB present with, or develop, complicated forms of chronic lung disease. These conditions present challenges for paediatric doctors, nurses and allied healthcare workers. A variation of the ‘inverse care law’1 is that the most complex patients present in hospital settings which have the least resources to manage them, including in district and provincial hospitals. In the last two decades the major focus of improving quality of paediatric care in these settings has been around triage and emergency care, and reducing deaths in the first 24 hours of hospitalisation.2 Children with complicated forms of TB are often both acutely and chronically ill, and there has been minimal focus on approaches to such disease processes in resource-limited settings. This includes effective models for ensuring ongoing community care.
This paper outlines some of the practical challenges of these illnesses in the acute and chronic phases, beyond those of antimicrobial chemotherapy, especially where resources are limited. These settings are typically small hospitals, often in rural or remote regions, with basic laboratory facilities and essential medicines.3 In such settings, a meticulous approach to the diagnosis, supportive care and monitoring of children with complex TB-related disease can achieve good outcomes. It is the attention to the most accurate diagnosis possible given the resources available, identification and avoidance of complications, supportive care, a focus on nutrition and physiotherapy, together with care provided by parents or caregivers that results in improved quality of life for many such children.
Articles have been published in the last few years on the epidemiology of childhood TB, multidrug resistance and advances in chemotherapy.4–7 Here, we focus on the clinical aspects of management, not to understate the challenges of antimicrobial therapy in an era of increasing drug resistance, but to convey that comprehensive approaches to improving the quality of clinical care are needed, and are accessible to district-level and provincial-level hospitals.
Considerations of complex care in district-level hospitals
WHO promotes an overall approach to all seriously ill children which includes triage, emergency treatment, history, examination, laboratory tests, diagnosis and differential diagnoses, treatment, supportive care, monitoring, discharge planning and follow-up.3 These stages of management are relevant to complicated TB infection, and represent a standard of care that is possible in a first-referral-level hospital. Care of chronically ill children, which is described in this paper, does not need to be high technology care or expensive care, and is not beyond the capacity of many district and provincial hospitals. Some technologies which are mentioned in this paper, such as CT scans and GeneXpert PCR testing, are unavailable in most district hospitals in rural settings. However, these are merely adjuncts to diagnosis in selected cases, and there is limited evidence that use of such technology in children with suspected TB improves outcomes. The majority of treatment decisions in most patients can be made effectively on clinical grounds. This is not substandard care, or unethical care, it represents optimal clinical care in a realistic environment. For referral beyond the district or provincial hospital clinical care to a tertiary level of care, the specific benefit to the child of such referral should be identified. Sometimes, the benefit of tertiary referral is less than what we as healthcare professionals or the family might imagine, if good medical, nursing and rehabilitative care is in place at a first-referral-level hospital.
CNS tuberculosis
Clinical presentation, history, examination and investigations
The clinical presentation of CNS TB varies, including meningitis, seizures and acute encephalopathy, raised intracranial pressure which may manifest as chronic headaches, visual disturbances, cranial nerve palsies, focal motor deficits such as hemiplegia or hemiparesis, hydrocephalus, movement disorders including dystonia, coma and progressive loss of developmental milestones. Raised intracranial pressure in TB may result from the space-occupying nature of a tubercular granuloma, brain oedema, cerebral infarction, venous thrombosis or hydrocephalus. The manifestations of CNS TB overlap with other diagnoses, including CNS tumours, stroke, viral encephalitis, HIV encephalopathy, cryptococcal meningitis and postinfectious inflammatory encephalopathies such as acute disseminated encephalomyelitis. In settings with limited diagnostic capacity, many children with acute or subacute febrile encephalopathy or elevated intracranial pressure are empirically treated as tuberculous meningitis (TBM) because of failure to improve after antibiotic treatment for bacterial meningitis, or because their history suggests exposure to infectious TB. This is a practical approach and sometimes the only safe course of action.
Diagnostic specificity is enhanced by good history taking, including being very clear about the onset of illness and what the child was like developmentally before becoming unwell. Sometimes the onset is obvious and the demarcation between the child’s normal state and sickness is clear, but often it is necessary to ask probing questions about the attaining of normal developmental milestones in the months preceding the onset of illness. For example, an infant who at 6 months was able to sit unaided and smile and laugh, but now at 8 months has decreased conscious state, wasting and spasticity indicates a recent deterioration in neurological state, which favours a subacute encephalopathy such as CNS TB as a diagnosis over cerebral palsy of perinatal origin.
Diagnostic specificity is also enhanced by cerebrospinal fluid (CSF) examination, with moderate-to-high lymphocyte count (100–1000 cells/microlitre) and protein (100–500 mg/dL). If available, acid-fast bacilli staining, culture and GeneXpert MTB/Rif testing of CSF can increase specificity.8 9 However, the ideal volume of CSF needed to do these tests is 6–8 mL, and the CSF should be centrifuged to test the supernatant. Sensitivity is low so no laboratory test on CSF can exclude TBM.10
CT scanning, if available, can be useful in specific circumstances, including where the clinical diagnosis is in doubt, or there is a suspicion of developing hydrocephalus. The typical findings of CNS TB include diffuse basal leptomeningeal enhancement on contrast-enhanced CT, hydrocephalus, supratentorial and brainstem infarction, and tubercular granulomas.11–13 Precontrast hyperdensity of the basal cisterns has been reported to also be a specific feature of TBM in children.14 Large ventricles, from hydrocephalus and/or cerebral atrophy occur in up to 70% of children with TBM who have CT scans.12 Tubercular granulomas with caseation have central heterogeneous enhancement and a ring-enhancing capsule (figure 1); once a tubercular granuloma proceeds to liquefaction, the CT appearance is that of a hypodense central component with peripheral ring enhancement. Tubercular granulomas occur in up to 70% of children with TBM at presentation or some stage during treatment.12

CT scan showing cerebellar ring-enhancing lesion in a child with tuberculosis.
Supportive care and monitoring
Children with CNS TB have many supportive clinical needs, outlined in table 1. Medical and nursing staff are responsible for coordinating these aspects of care and ensuring that the child receives holistic care. Many people are involved, especially physiotherapists, nutrition nurses and the parents or other family caregivers.
Supportive care needs for children with central nervous system TB
Adjunctive treatments and complications
Adjunctive treatment with dexamethasone has some benefit in CNS TB, more so for tubercular granulomas, especially if there is surrounding oedema. Various regimens are used.15 If using dexamethasone: give 4 weeks of 0.4 mg/kg once a day x 1 week, 0.3 mg/kg once a day x 1 week, 0.2 mg/kg once a day x 1 week, 0.1 mg/kg once a day x 1 week, followed by 2–4 weeks of further tapering. If using prednisolone: 1 mg/kg two times a day for 2 weeks, then 1 mg/kg once a day for 2 weeks, then 0.5 mg/kg/day for 2 weeks then cease.
Children with TBM may develop hydrocephalus, prevalence rates are estimated as high as 70% in children having neuroimaging.15 Hydrocephalus can develop while a child is undergoing treatment, so this can be a reason for deterioration after commencing treatment. It is often difficult to identify the cause of deterioration while on treatment; which can include non-adherence with medications, multidrug-resistant TB (MDR TB) or development of hydrocephalus, stroke or epilepsy. A child with TBM who deteriorates on treatment or does not seem to be improving should be considered for cerebral imaging where possible. On CT scan, sometimes it can be challenging to distinguish between ventriculomegaly because of cerebral atrophy (not under pressure) and hydrocephalus; both are often present in chronic CNS TB. In true hydrocephalus, the ventricles are large and cerebral cortex is compressed with loss of normal spaces around the sulci and gyri. With ventriculomegaly due to cerebral atrophy, sometimes called ‘ex-vacuo hydrocephalus’, the sulci of the cortex are typically more spacious than the normal and the cerebral cortex is thin, with more extra-axial fluid spaces (around the brain). Children with ex-vacuo hydrocephalus will not have macrocephaly, and depending on the age may have failure of head growth or microcephaly. Children with hydrocephalus will have macrocephaly if their sutures are not fused, and a lateral skull X-ray may show a copper-beaten appearance to the bone, and widely split sutures (figure 2).

Lateral skull X-ray of a child with tuberculosis with raised intracranial pressure.
Diuretics, particularly acetazolamide (50 mg/kg/day) and/or frusemide, are often used as medical treatment for TB-related communicating hydrocephalus. This will benefit some children, but a proportion will fail medical therapy and require a ventriculoperitoneal (VP) shunt.16–18 Complications of diuretic therapy need to be monitored.
In TB-related hydrocephalus a VP shunt can be effective in improving outcome, especially if done early. Studies suggest that surgical placement of a VP shunt has a role even in advanced hydrocephalus, but that children less than 3 years of age may do worse than older children.19 Hydrocephalus can be associated with other brain lesions such as areas of vasculitis causing ischaemia or stroke, or a compressive tuberculoma, and this influences outcome. Complications of VP shunts, especially shunt blockage, shunt infection and hospitalisation with suspected infection are common.18
Monitoring and interpreting rates of improvement
The expected rate of improvement depends on the depth of unconsciousness and the types of neuropathology present at the commencement of treatment, and the presence of comorbidities such as HIV and malnutrition. Improvements require opportunity, and are less likely if a child is bed-bound and malnourished. Physiotherapy helps; putting weak or contracted joints and limbs through a full range of movement, sitting upright in a chair, mobilisation out of a ward in a wheelchair or with other supports, having age-appropriate stimulation, natural light and a day–night sleep–wake cycle are all important.
Some children with CNS TB require anticonvulsants for seizures, or medications to reduce dystonia, such as baclofen or gabapentin. The interaction of these drugs and TB treatment, and their effects on conscious state and ability to cooperate with rehabilitation need to be considered, and balanced.
Sometimes, difficult treatment decisions arise when children are slow to improve. If there has been no objective improvement in the 2 months of intensive phase of TB treatment, MDR TB should be strongly considered. Some questions in the assessment of improvement and in considering MDR TB as a possible cause of failure to improve are listed below.
Key questions in the assessment of improvement
Adherence issues
Has there been sufficient time for improvement?
Have the objective markers of inflammation, including fever, improved?
How deep was the unconsciousness or how severe were the neurological findings on commencing treatment? In this context, has there been sufficient time for improvement?
Have there been sufficient opportunities for rehabilitation?
Have there been iatrogenic complications that would slow the rate of improvement?
Have other comorbid conditions such as malnutrition, anaemia and HIV been addressed?
Are there any drug interactions that may affect improvement?
Are there untreated complications, such as hydrocephalus, or epilepsy, or established brain injury as a complication of CNS TB?
Is there any risk of exposure to MDR TB?
Is the diagnosis of CNS TB likely to be correct? Could there have been pre-existing neurological or developmental problems?
Chronic TB-related lung disease
Pulmonary TB can progress to complicated chronic lung disease in children. This is especially the case in late presentation, relapsed TB, extensive lung disease, poor adherence, MDR TB or HIV.20 The chronic lung pathologies may include cystic, emphysematous lung disease, pulmonary fibrosis, restrictive pleural disease or bronchiectasis. Higher bacterial load,20 21 coinfection with HIV22 and exposure to indoor air pollution from burning of biomass fuels appear to be risk factors for more severe TB-related lung disease.23
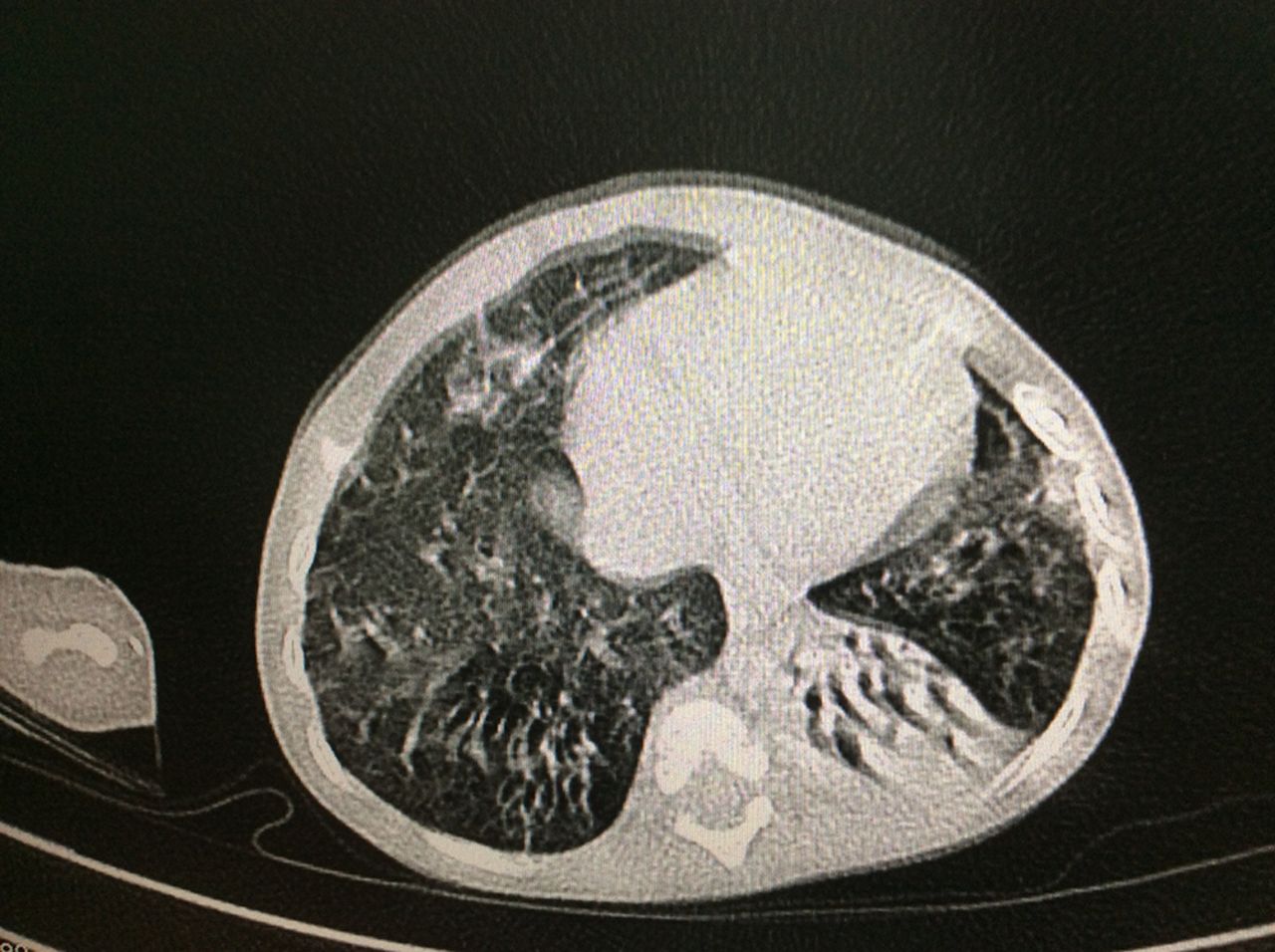
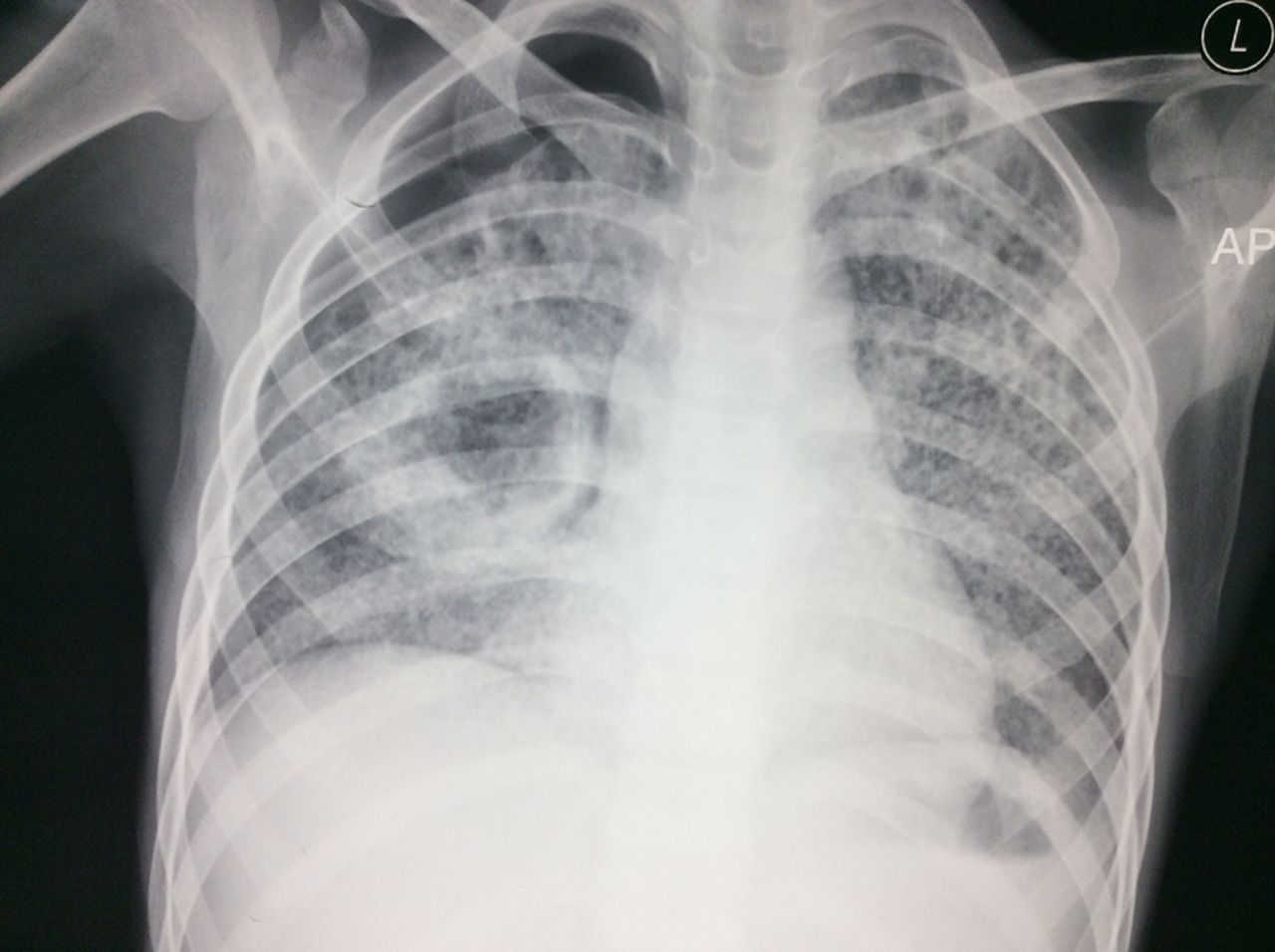
Table 2 lists other diseases which can mimic or complicate TB-related chronic lung disease, and distinguishing clinical features. Chest radiograph can help distinguish between these types of chronic lung diseases. Chest CTs, if available, provide clear definition of bronchiectasis, pleural thickening and other chronic changes (figure 3).21 A miliary pattern (figure 4) is pathognomonic, but radiology is rarely conclusive. The working diagnosis will usually be based on a combination of clinical features, radiography and laboratory investigations.

CT chest of a child with chronic cystic lung disease and bronchiectasis due to tuberculosis.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Severe miliary tuberculosis with cavitation and pneumothorax.
Differential diagnostic and treatment considerations in chronic lung diseases in children, including chronic and complicated pulmonary TB
Adjunctive treatments
Table 2 also outlines some of the adjunctive treatments that may help in some cases of specific chronic complicated TB and its differential diagnoses. In most cases, mobilisation, deep breathing exercises and physiotherapy are useful. Prolonged bed rest leads to dependent atelectasis, lobar collapse and reduced sputum clearance. Mobilisation, even if in a wheelchair, helps reinflate posterior collapsed lung segments and induces cough and aids sputum clearance. Many of the supportive care requirements listed in table 1 also apply to children with chronic TB-related lung disease.
Therapeutic trials and monitoring improvement
Sometimes, based on likely clinical diagnoses in table 2 or as adjunctive treatments for chronic lung disease, therapeutic trials are needed. These may be of bronchodilators, corticosteroids, nebulised hypertonic saline, diuretics, medications to reduce pulmonary hypertension, judicious use of prophylactic antibiotics and other therapies. Where possible such trials should have an objective assessment of effect, and treatments should be discontinued if there is no objective effect. A standardised 1–3 min walking or step exercise test,24 modified for the child, with measurement of respiratory rate, heart rate, oxygen saturation and spirometry or peak expiratory flow rates if the child is capable, at baseline and following exercise can be useful (see box 1). This can guide decision about the effectiveness of interventions, the need for oxygen for mobilisation and the safety of hospital discharge.
Simple exercise test
Start with a 1 min walking test, between cones separated by 10 m
Baseline measurements:
Respiratory rate (breaths per minute)
Heart rate
Oxygen saturation at rest
Self-assessment of respiratory difficulty
Peak expiratory flow rate or spirometry if it can be done (best of three attempts).
Ask the child to walk as fast as they can for 1 min, and then measure
Respiratory rate
Heart rate
Oxygen saturation
Self-assessment of respiratory difficulty
Peak expiratory flow rate or spirometry if it can be done (best of three attempts).
Do this test weekly. Progressively increase the exercise duration to 2 and then 3 min and the distance between cones to 20 m as tolerated.
Graph progress so that the child can see improvement. Point out to the child and the family the type of activities that can be done safely, if they can walk for 1 min without getting breathless or needing oxygen.
Nutrition in all complicated forms of TB
Almost all children with TBM, chronic pulmonary TB and other forms of disseminated TB have weight loss, many have severe wasting and stunting. Malnutrition is a significant risk factor in turning latent TB into active TB,25 and a body mass index (BMI) <16 is associated with significant higher mortality in adults with TB.26 Patients with active TB have decreased blood concentrations of micronutrients, including retinol, vitamins C and E, zinc, iron and selenium.27 If not addressed, the protein–calorie malnutrition worsens even after children commence treatment, because of chronic inflammation, anorexia (loss of appetite because of medications and general illness) and poor food intake.
Nutrition should be instituted as soon as possible, either orally or through nasogastric tube, according to WHO guidelines for the level of malnutrition,3 together with the TB drugs. Children with TB should be weighed regularly, given a nutritious diet, daily micronutrients and have their food intake monitored. Children on isoniazid should be on pyridoxine. Iron supplementation should be given to children with iron deficiency,28 as manifest by a low haemoglobin, low mean cell volume and a high red cell distribution width.
Administering nutrition to all those with malnutrition in a busy children’s ward is a full-time job, so it is important to a well-functioning nutrition unit and nurses who are informed and enthusiastic about nutrition. Plotting weight, mid-upper arm circumference and BMI in older children helps monitor progress.
Identifying and treating comorbidity
All children with TB should have an HIV test, and if positive commenced on antiretroviral therapy (ART) in a staged fashion. TB treatment should be started first, followed by ART as soon as possible thereafter, at least within 8 weeks of the start of TB treatment. Where a CD4 count can be done, if below 50 cells per mm3, ART should be commenced within 2 weeks of the start of TB treatment. WHO has detailed guidance for national TB programmes on the management of TB and HIV in children.29
Risk assessment and understanding the patient’s journey
Understanding the patient’s journey, from the time of first symptoms to presentation and effective treatment is important. For many children, this can involve a family member having TB, multiple presentations to health professionals, previous courses of antibiotic treatment or truncated courses of TB treatment, non-adherence or defaulting from treatment, premature discharge from a health facility and relapse with a more severe form of TB. Understanding the timeline and journey can help in risk assessment at the time of discharge planning, and it can help understand families’ experiences with health services.
Risk assessment is needed at milestones in the treatment. The risks are different on admission, in acute and chronic stages, and when contemplating discharge. Early risks include acute medical and nutritional complications, including nosocomial infections, and chronic phase risks include being the potential for non-adherence if discharged too early, or risks of chronic adverse health and developmental outcomes.
Psychological support to the child and family, providing a child or adolescent friendly and stimulating environment and education opportunities are important for recovery and optimising outcome.
For children who present too late to be cured and even for those in whom cure is uncertain or possible, providing palliative care is an important component of management. Sources of pain include raised intracranial pressure, pleuritic inflammation, bony infiltration or erosion, neuropathic pain from nerve compression in Pott’s disease or from isoniazid and chest wall muscle ache from coughing. Nausea and vomiting from drugs or gastrointestinal TB, the distress of breathlessness and coughing and night sweats are other symptoms that may need treatment. Following a pain ladder for appropriate use of paracetamol, oral morphine and codeine, using ibuprofen, amitriptyline or gabapentin for neuropathic pain and being aware of drug side effects and interactions are all important.30 Many families prefer palliative care to be provided in their homes, successful examples exist of community-based palliative care for TB patients.31
Discharge planning and follow-up
Since at the time of admission the outcome for children with severe complicated TB is often unpredictable, the parents should be advised of a realistic range of functional outcomes for their child. They should also be advised that it takes time to determine the prognosis and outcome, that everyone in the ward will do their best to optimise the outcome and that they—the parents—have a large role in helping the child improve, by adhering to medicines and providing supportive care, love and encouragement. Parents should be informed that the hospital treatment is long; 2 to 9 months of hospitalisation depending on the rate of recovery. Such information puts parents and staff in a much better position to accept positive or negative outcomes. It is important not to raise unrealistic expectations, but also important not to take away hope, which is essential for parent’s mental health and the recovery of the child.
Families should be fully informed early of the steps that are needed prior to discharge, including nutrition and physical rehabilitation. Some of the steps prior to discharge are outlined in box 2. These steps can be worked towards steadily during the child’s time in hospital, so that the parents and the child understand that progress is being made. Depending on the family’s social circumstances and how far they live from the hospital, and if certain community healthcare services are available (box 2), much of the treatment and rehabilitation can occur closer to home. Transition from hospital to outpatients and community requires services to be in place, and good communication to occur. Most countries have national TB programmes and WHO has guidance on integrating childhood TB management into national programmes, and family and community follow-up.29 A roving outreach TB nurse who visits families in their homes can greatly assist in follow-up.32 Understanding the environment to which the child is being discharged, the resources of the family and their vulnerabilities can help assess the risks of receiving adequate care after discharge.
Steps prior to discharge of children with complicated tuberculosis
The child is clinically well, and the original symptoms have resolved:
Not in severe respiratory distress
Not requiring oxygen
Not febrile
Eating well and gaining weight
Ascites or plural effusions resolving
Mobilising
Swallowing treatment well
Exercise tolerance test suggests the child can cope outside hospital with required daily activities.
The child and their parents or guardians understand about their condition:
Understand they have tuberculosis (TB)
Understand the duration of treatment required
Understand the need to take treatment daily, even if they are feeling well
Understand the consequences of stopping or interrupting their treatment
Understand the importance of nutrition, fresh air and activity to recovery.
HIV test done
Understand the result
Commenced on treatment if positive.
Family screening completed
Family members with TB are on treatment
Siblings under 5 years of age who are exposed but asymptomatic are on isoniazid preventative therapy.
Registration and ongoing treatment properly organised
Registered with the national TB Programme.
The clinic in which the child will receive treatment has been identified, and it is certain that the clinic can provide the necessary therapy.
A directly observed treatment, short-course provider is identified, and has undergone education about his/her role.
Community-based or outpatient TB and rehabilitative healthcare is organised and the child is linked with this
Rehabilitation can continue in the community, with physiotherapy, growth monitoring, assessment of adherence and symptoms if services are in place.
An outreach nurse or health worker visits the child in their home
Assessment of the environment and its suitability for the child in that phase of treatment and rehabilitation.
Assessment of what else the family needs in terms of social, nutritional and financial support.
There are a number of barriers to care for children with chronic complex healthcare needs, including access to services if they live in rural areas, lack of chronic disease programmes, perceived competition for hospital beds and the ethics of setting limits on escalation of care. However, the gains that can be made in health and quality of life if children are provided with holistic comprehensive care by hospitals within their community and the support this can be to their families are immense.
Watt33 speculated that addressing the inverse care law in deprived communities required a personal doctor, who knew his or her patients well, could see their problems in the family and community context and worked with patients over a long time to reverse risks and prevent complications. A personal doctor or child health nurse who takes responsibility for providing, coordinating and monitoring care is also needed for the best outcomes in complicated childhood TB and other chronic paediatric illnesses. In the era of the Sustainable Development Goals children with chronic conditions deserve this, wherever they live.
Acknowledgments
The Centre for International Child Health (CICH) is associated with the RE Ross Trust (Victoria). We are grateful for their support to this work. CICH is a World Health Organization Collaborating Centre for Research and Training in Child and Neonatal Health.
References
Footnotes
Contributors TD wrote the first draft; SKT, HP and HW contributed to the ideas presented and made substantial revisions. All authors reviewed and approved the final version of the paper.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.