Article Text

Abstract
Objective Racecadotril is an antisecretory agent that can prevent fluid/electrolyte depletion from the bowel as a result of acute diarrhoea without affecting intestinal motility. An up-to-date systematic review is indicated to summarise the evidence on racecadotril for the treatment of acute diarrhoea in children.
Design A Cochrane format systematic review of randomised controlled trials (RCTs). Data extraction and assessment of methodological quality were performed independently by two reviewers. Methodological quality was assessed using the Cochrane risk of bias tool.
Patients Children with acute diarrhoea, as defined by the primary studies.
Interventions RCTs comparing racecadotril with placebo or other interventions.
Main outcome measurs Duration of illness, stool output/volume and adverse events.
Results Seven RCTs were included, five comparing racecadotril with placebo or no intervention, one with pectin/kaolin and one with loperamide. Moderate to high risk of bias was present in all studies. There was no significant difference in efficacy or adverse events between racecadotril and loperamide. A meta-analysis of three studies with 642 participants showed significantly shorter duration of symptoms with racecadotril compared with placebo (mean difference −53.48 h, 95% CI −65.64 to −41.33). A meta-analysis of five studies with 949 participants showed no significant difference in adverse events between racecadotril and placebo (risk ratio 0.99, 95% CI 0.73 to 1.34).
Conclusions There is some evidence that racecadotril is more effective than placebo or no intervention in reducing the duration of illness and stool output in children with acute diarrhoea. However, the overall quality of the evidence is limited due to sparse data, heterogeneity and risk of bias. Racecadotril appears to be safe and well tolerated.
- Evidence Based Medicine
- General Paediatrics
- Gastroenterology
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
What is already known on this topic
Oral rehydration solution (ORS) is the mainstay of treatment for acute diarrhoea in children.
Racecadotril is an antisecretory agent with a different mechanism of action from existing antidiarrhoeal agents that can be used with ORS to prevent fluid and electrolyte depletion.
Previous reviews are limited by age and significant methodological flaws.
What this study adds
The evidence synthesised suggests that the addition of racecadotril to ORS can reduce the length of symptoms as well as the number and volume of stools passed during the illness.
The use of racecadotril appears self and well tolerated in children with acute diarrhoea.
The evidence base is generally of low quality and at high risk of bias.
Background
Acute diarrhoea, with or without vomiting, constitutes approximately 14% of presentations to paediatric A&E departments every year in the UK,1 leading to over 50 000 acute admissions annually in England alone.2 Acute watery diarrhoea continues to cause significant morbidity in infants and young children both in developing3 and developed4 countries, despite advances in oral rehydration therapy and newly developed vaccines. As a result, this condition remains a substantial financial burden to the NHS at both secondary and tertiary level care.2
Although diseases leading to an acute diarrhoeal illness are often self-limiting, shortening of the illness duration can have significant benefits with regard to hydration and subsequent morbidity. Oral rehydration therapy, although still underused in some areas,5 has become the foundation during an acute diarrhoeal illness although, increasingly, μ-opioid receptor agonists have become more popular in certain situations.6 Racecadotril is an antisecretory agent with a different mechanism of action from existing antidiarrhoeal agents. It functions by selective inhibition of the enzyme neutral endopeptidase (also known as enkephalinase), a cell membrane peptidase enzyme found most commonly on the epithelium of the small intestine.7 The enzyme neutral endopeptidase degrades endogenous enkephalins in the intestinal mucosa which normally exhibit pro-absorptive and antisecretory properties. Racecadotril therefore aims to promote these antisecretory properties by prolonging the presence of the enkephalins through the inhibition of neutral endopeptidase. Ultimately, the hypersecretion of water and electrolytes is reduced without affecting intestinal motility/transit.
The main aim of treatment with racecadotril is to prevent fluid/electrolyte depletion from the bowel as a result of acute diarrhoea. The drug should be used alongside oral rehydration solution (ORS) as recommended by the National Institute of Health and Care Excellence (NICE) clinical guideline CG84 in children aged >3 months, as per licensing regulations. The treatment should be started following three episodes of watery diarrhoea in a 24 h period, until two normal stools have been produced. The product should be used for a maximum of 7 days.
The intervention with racecadotril aims to reduce symptoms of acute diarrhoea within the first 24 h of treatment by reducing stool frequency without affecting intestinal motility. Side effects of abdominal pain, bloating and rebound constipation, which occur with other well-known antidiarrhoeal agents, would not be expected with this treatment.
Racecadotril was first licensed in France in 1992 but has only been licensed and marketed since 2013 for use in children within the UK. Although there have been previously published reviews of the literature regarding racecadotril that included some meta-analysis, there are some clear limitations to this work. A review from 2007 is now significantly out of date with just three studies included.8 A review from 2011 has significant methodological flaws with one of the included studies not a randomised controlled trial (RCT) and a further study written by one of the review authors who would not provide more methodological data when requested.9 Additionally, neither of these reviews aligned themselves with the internationally recognised Cochrane standard for evidence synthesis. An up-to-date systematic review using the Cochrane Collaboration format is therefore indicated to summarise the current evidence on the efficacy and safety of racecadotril for the treatment of acute diarrhoea in children.
Methods
The objectives of this review were to evaluate the efficacy and safety of racecadotril for the treatment of acute diarrhoea in children. A full protocol for the study was completed by the authors prior to commencement of the study and is available on request.
Criteria for considering studies for this review
RCTs were included in this systematic review. Participants were aged 3 months to 18 years with a diagnosis of acute diarrhoea (defined as three or more episodes of watery diarrhoea in a 24 h period within the last 72 h). Studies compared racecadotril with another intervention or placebo, with all preparations and dosing regimens considered. Studies could give ORS to both groups, as this is the recommended administration method for racecadotril. The primary outcome measure for the studies was the total duration of diarrhoeal illness in days, as defined by the initial inclusion criteria. Secondary outcomes included: number of diarrhoeal episodes occurring per day at 48 h following treatment, duration of time taken for resolution of symptoms, stool output in kg per day in first 48 h after treatment, use of concomitant or alternative therapies such as other antidiarrhoeal agents, need for hospital admission, duration of hospital stay if admitted as inpatient and occurrence of any adverse events.
Search methods for identification of studies
Electronic searches (search strategy not limited by language) were completed of MEDLINE (1966 to 23 February 2015; National Library of Medicine, Bethesda, USA), EMBASE (1974 to 23 February 2015; Elsevier Science, New York, USA), Cochrane Central Register of Controlled Trials and Cochrane Inflammatory Bowel Disease and Functional Bowel Disorder Group Specialized Trials Register. The search strategy is shown in online supplementary appendix 1.
Similar search strategies, modified appropriately and using the same keywords, were used to search the other electronic databases listed above. There is some evidence that data from abstracts can be inconsistent with data in published articles.10 Therefore, relevant citations published in abstract form that met the inclusion criteria were only considered if the author could offer sufficient data regarding risk of bias and outcomes.
The references of all identified studies were inspected for more trials. Leaders in the field were contacted to try to identify other studies. Finally, the manufacturers of racecadotril were contacted for additional data. Unpublished studies were considered if they offered appropriate methodological and quality data.
Data collection and analysis
All identified abstracts and results from searches were reviewed by the authors. If the reference appeared relevant, a full copy of the study was obtained. After reading the full texts, each author independently assessed the eligibility of all trials identified based on the inclusion criteria above. Disagreement among authors was discussed and agreement reached by consensus. If the data to judge inclusion were unclear, attempts were made to contact the authors.
A data extraction form was developed and piloted to extract information on relevant features and results of all primary and secondary outcomes of included studies. The two reviewers separately extracted and recorded data on the predefined checklist, with disagreement discussed and consensus reached.
The risk of bias of selected trials was assessed independently by the authors using the Cochrane risk of bias tool,11 with disagreement once again resolved by reaching consensus. Study authors were contacted for further information when insufficient information was offered to judge risk of bias or data were missing for primary outcomes.
Analysis was completed using Revman (Review Manager 5.2, V.5.2.9, The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, 2012). The primary outcome—total duration of diarrhoeal illness—was assessed using the mean difference (MD) with 95% CI. The secondary outcomes were assessed by calculating the risk ratio (RR) and 95% CI or the MD with 95% CI, as indicated. The authors of included studies were again contacted to supply any missing data.
Heterogeneity among trial results was assessed by inspection of graphical presentations and by calculating the χ2 test of heterogeneity (a p value of 0.10 was regarded as statistically significant). We also used the I2 statistic to quantity the effect of heterogeneity.12 A random-effects model was used, with a sensitivity analysis with the fixed-effects model, to identify differences in results that would suggest heterogeneity.
Results
Description of studies
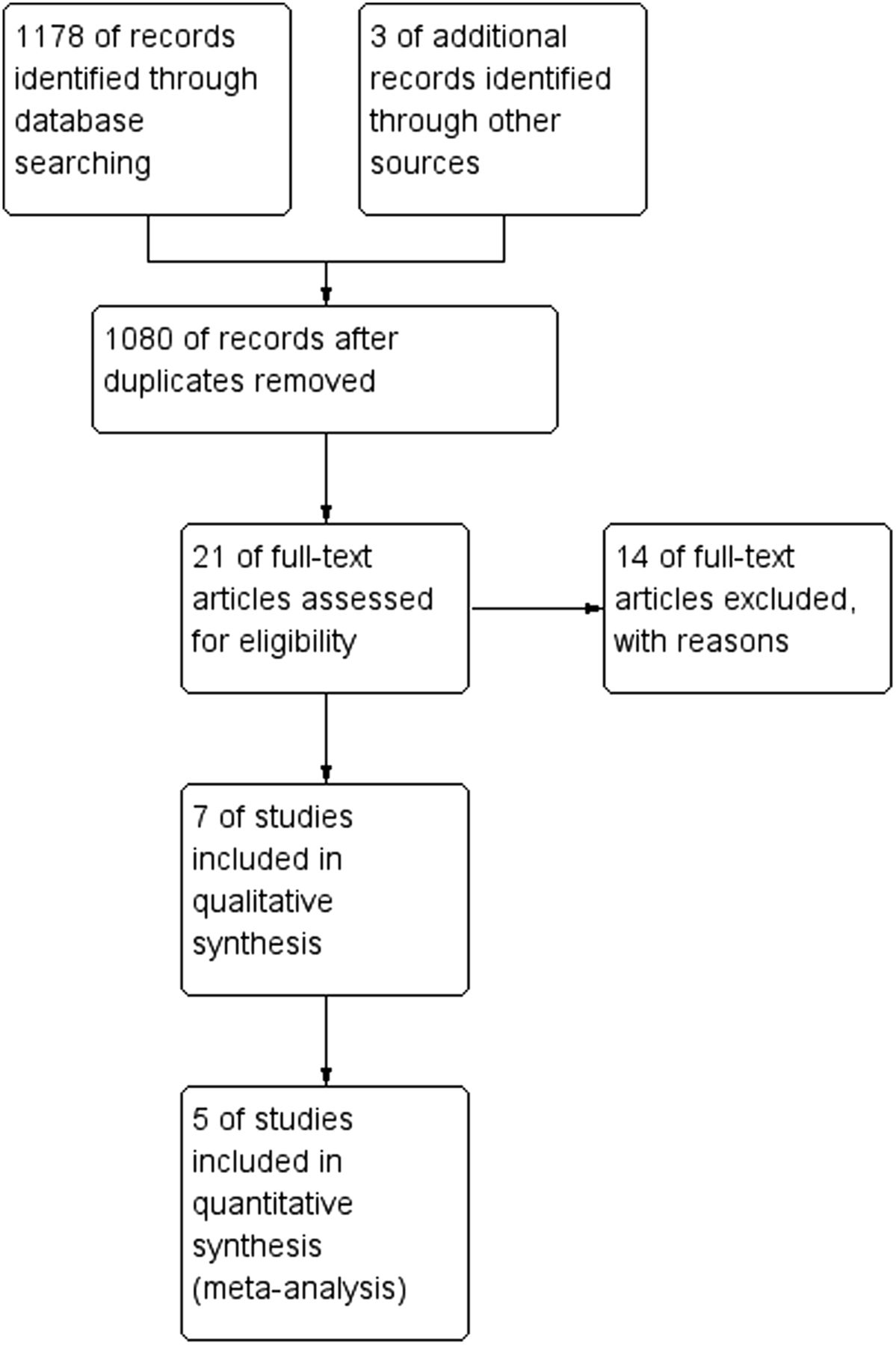
The electronic database search identified 1178 studies that were screened for inclusion. Of these, 21 studies were judged to be potentially relevant and subjected to full text review (figure 1). Experts were contacted, but no extra reports were received and no further studies were identified from drug companies.

Flow diagram for search.
Fourteen reports were excluded for failing to meet the inclusion criteria (table 1). One was an abstract with insufficient data to judge inclusion, one was an adult RCT, five were studies that were not RCTs and seven were review articles or opinion pieces. Of particular note, three of these 14 studies were included in a previously published meta-analysis.9 One study was only published in this existing meta-analysis and did not offer appropriate information to judge inclusion.24 The author was contacted but was not able to offer further information so the study was excluded. Two further studies were not randomised14 ,15 (one was published in Spanish and when translated was not random and one used alternate assignment into each group, an inappropriate method of randomisation).
Excluded papers with reasons
Six reports of seven studies satisfied the inclusion criteria and were included in the review (table 2). Five studies compared racecadotril with placebo. One of these reports described two studies, an inpatient and an outpatient study.26 The author was contacted and was able to offer sufficient data to allow the studies to be analysed separately. One study compared racecadotril with loperamide and one study compared racecadotril with kaolin. The total number of participants in the seven studies was 1112. All participants were children between 1 month and 10 years of age with acute diarrhoea.
Characteristics of included studies and risk of bias
Risk of bias of included studies
Three studies were rated as low risk for random sequence generation (selection bias) because these studies employed computer-generated randomisation. The remaining studies described themselves as randomised but, with no further details given or available from authors, were rated as unclear risk of bias.
Two studies were rated as low risk of bias for allocation concealment (selection bias). Four studies were rated as unclear risk of bias for allocation concealment as the methods were not clearly described in the manuscripts. One study described a method that did not ensure allocation concealment and so was rated as high risk of bias.29
Five studies were double-blinded and were judged to be at low risk of bias for blinding of participants and personnel (performance bias). One study described itself as blinded, but gave no further details so was rated as unclear risk of bias. One study was open-label and judged to be at high risk of bias for blinding of participants and personnel.
Five studies reported full and appropriate data and satisfactorily documented withdrawals and dropouts and were therefore judged to be at low risk of bias for incomplete outcome data (attrition bias) and six were judged as low risk for selective reporting (reporting bias). Two studies did not record full data for all patients and were judged high risk of bias for attrition bias. One study did not offer outcome data regarding side effects and so was judged at high risk for reporting bias.
Finally, all but one study were judged to be at low risk for other sources of bias. This study had an affiliation with a pharmaceutical company, but details of the extent of involvement were unavailable and so it was judged to be at unclear risk of bias. Details are summarised in table 2.
Racecadotril versus placebo
Efficacy
Three studies with 642 participants presented data on the primary outcome, duration of diarrhoeal symptoms. Meta-analysis showed significantly shorter duration of diarrhoeal symptoms in patients in the racecadotril group compared with patients receiving placebo or no intervention (MD −53.48 h, 95% CI −65.64 to −41.33, figure 2). A sensitivity analysis with the fixed-effects model did not change the result. In the other studies the data were not reported in a manner that allowed inclusion within this meta-analysis.

Forest plot of duration of diarrhoeal symptoms, racecadotril versus placebo.
For secondary outcomes, studies reported differently based on the setting of patients. Meta-analysis of two studies with 405 inpatient participants showed significantly less stool output in the first 48 h of treatment in the racecadotril group compared with placebo or no intervention (MD −150 g/kg, 95% CI −291 to −8.9, figure 3). This result showed significant heterogeneity, but was still significant using a fixed-effects model. Meta-analysis of three studies with 422 outpatient participants showed less stool output per day at 48 h in the racecadotril group, although this was not significant (MD −2.59 stools per day, 95% CI −5.26 to 0.08, figure 4). There was significant heterogeneity, with the result showing a significantly significant difference favouring racecadotril when using the fixed-effects model (MD −2.57 stools per day, 95% CI −3.03 to −2.30).

Forest plot of stool output in the first 48 h, racecadotril versus placebo.

Forest plot of stool output per day at 48 h, racecadotril versus placebo.
Further subgroup analyses were planned but could not be performed due to limited data within the included studies.
Safety
Meta-analysis of five studies with 949 participants showed no significant difference in reported adverse events between racecadotril and placebo (OR 0.99, 95% CI 0.73 to 1.34, figure 5). Studies totalled events, but did not give a specific breakdown of specific events. Events reported included vomiting, abdominal distension, abdominal pain, rashes and one case of transient raised transaminases (racecadotril).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot of total reported adverse events, racecadotril versus placebo.
No serious adverse events were reported in any study. Funnel plots of these analyses were symmetrical.
Racecadotril versus loperamide
As there was only one study, no meta-analysis was performed.
Efficacy
The duration of diarrhoeal symptoms was reported as similar between the two groups (mean (SE) 10.7 (1.7) h with racecadotril vs 8.8 (2.3) h with loperamide).
Safety
The incidence of adverse events was lower with racecadotril than with loperamide and significantly more patients on loperamide had constipation.
Racecadotril versus kaolin/pectin
As there was only one study, no meta-analysis was performed.
Efficacy
The number of diarrhoeal episodes was reported as significantly less in the racecadotril group (mean total of 18.96 episodes with kaolin/pectin vs 8.88 with racecadotril).
Safety
Adverse events data were not presented.
Discussion
With the new licence for racecadotril in the UK allowing use in children under 4 years of age, it is important to clearly establish the evidence base regarding its efficacy and safety. The evidence synthesised suggests that the addition of racecadotril to ORS can reduce the duration of symptoms as well as the number and volume of stools passed during the illness. When these results are considered in a clinical context they do appear significant, with a reduction of symptoms of >2 days and 130 mL/kg of stool loss per day likely to have a significant impact for both the child and parent. Adverse events in children receiving racecadotril were not statistically significantly different from placebo, suggesting appropriate safety. Heterogeneity in reporting did not allow any other outcomes to be analysed.
It must be noted that the quality of the evidence base was less than optimum, with several studies having significant areas where risk of bias was of concern. Clinical heterogeneity in terms of the context and countries of studies, as well as methodological heterogeneity in the outcomes measured, age of participants and time and setting of recruitment, further weaken the evidence base, so it is suggested that these are considered when judging the strength of the findings. Additionally, it is worth noting that there have been no studies completed in the UK.
In examining the introduction of a new treatment such as this within the UK, there is more to consider than simply efficacy and safety. Clarifying the evidence base allows those considering the use of this agent to begin to evaluate these other aspects. A recent study has sought to complete a UK-centred cost analysis which suggests that racecadotril is less costly than ORS alone for the treatment of children with acute diarrhoea.21 However, such analysis does not consider the context-specific issues that will be key to consider when making local decisions about the introduction of such an agent, including the time of use within a diarrhoeal illness and whether initiation takes place in primary or secondary care. Additionally, there are no studies that consider qualitative outcomes that may be key in deciding whether to employ such an adjunct agent. Considering how the use of racecadotril changes the impact of such illness on patients, parents and families would further inform commissioning bodies and wider stakeholders in the role of this agent.
Conclusions
There is evidence from this review that racecadotril is more effective than placebo or no intervention in reducing the duration of illness and stool output in children with acute diarrhoea and appears to be safe. The overall quality of the evidence and strength of these conclusions is limited due to sparse data, heterogeneity and risk of bias in the studies. Further work is suggested to consider the qualitative impact on patients and families within the UK of the use of such an agent as an adjunct therapy for acute diarrhoeal illness.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Contributors MG conceived the study and led the study and writing of the manuscript. AA contributed and reviewed the protocol and writing of the manuscript and finalised the final draft, as well as co-searching and extracting the data.
Competing interests MG has received travel and educational grants from various companies including Danone, Abbott, Warner Chilcott, Casen Fleet, Norgine, Ferring and Vifor. These companies had no involvement in the carrying out or reporting of this or any other research works. Abbott gave a travel grant to present these results at DDW in 2014 in USA but had no involvement in the planning, execution or writing of this or any studies. AA has nothing to declare.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement For the study protocol and any further data, please email morris@betterprescribing.com.