Article Text

Abstract
Bullying is the systematic abuse of power and is defined as aggressive behaviour or intentional harm-doing by peers that is carried out repeatedly and involves an imbalance of power. Being bullied is still often wrongly considered as a ‘normal rite of passage’. This review considers the importance of bullying as a major risk factor for poor physical and mental health and reduced adaptation to adult roles including forming lasting relationships, integrating into work and being economically independent. Bullying by peers has been mostly ignored by health professionals but should be considered as a significant risk factor and safeguarding issue.
- Child Abuse
- Psychology
- School Health
- General Paediatrics
- Outcomes research
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Definition and epidemiology
Bullying is the systematic abuse of power and is defined as aggressive behaviour or intentional harm-doing by peers that is carried out repeatedly and involves an imbalance of power, either actual or perceived, between the victim and the bully.1 Bullying can take the form of direct bullying, which includes physical and verbal acts of aggression such as hitting, stealing or name calling, or indirect bullying, which is characterised by social exclusion (eg, you cannot play with us, you are not invited, etc) and rumour spreading.2–4 Children can be involved in bullying as victims and bullies, and also as bully/victims, a subgroup of victims who also display bullying behaviour.5 ,6 Recently there has been much interest in cyberbullying, which can be broadly defined as any bullying which is performed via electronic means, such as mobile phones or the internet. One in three children report having been bullied at some point in their lives, and 10–14% experience chronic bullying lasting for more than 6 months.7 ,8 Between 2% and 5% are bullies and a similar number are bully/victims in childhood/adolescence.9 Rates of cyberbullying are substantially lower at around 4.5% for victims and 2.8% for perpetrators (bullies and bully/victims), with up to 90% of the cyber-bullying victims also being traditionally (face to face) bullied.10 Being bullied by peers is the most frequent form of abuse encountered by children, much higher than abuse by parents or other adult perpetrators11 (box 1).
Bullying screener
Direct bullying refers to harming others by directly getting at them. It is done by one or a group of pupils repeatedly against some children at school. These children:
Are threatened or blackmailed or have their things stolen
Are insulted or get called nasty names
Have nasty tricks played on them/are subject to ridicule
Are hit, shoved around or beaten up
Relational bullying refers to damage relationships between friends and destroy status in groups to hurt or upset someone. Over and over again some children at school:
Get deliberately left out of get-togethers, parties, trips or groups
Have others ignore them, not wanting to be their friend anymore, or not wanting them around in their group
Have nasty lies, rumours or stories told about them
Cyberbullying is when someone tries to upset and harm a person using electronic means (eg, mobile phones, text messages, instant messaging, blogs, websites (eg, Facebook, YouTube) or emails)
Have their private email, instant mail or text messages forwarded to someone else or have them posted where others can see them
Have rumours spread about them online
Get threatening or aggressive emails, instant messages or text messages
Have embarrassing pictures posted online without their permission
(Answered for A, B, and C separately on this 4-point scale)
How often have these things happened to you in the last 6 months?
Never
Not much (1–3 times)
Quite a lot (more than 4 times)
A lot (at least once a week)
How often have you done these things to others in the last 6 months?
Never
Not much (1–3 times)
Quite a lot (more than 4 times)
A lot (at least once a week)
Victims: Happened to them: quite a lot/a lot; did to others: never/not much
Bully/victims: Happened to them: quite a lot/a lot; did to others: quite a lot/a lot
Bullies: Happened to them: never/not much; did to others: quite a lot/a lot
Bullying is not conduct disorder
Bullying is found in all societies, including modern hunter-gatherer societies and ancient civilisations. It is considered an evolutionary adaptation, the purpose of which is to gain high status and dominance,14 get access to resources, secure survival, reduce stress and allow for more mating opportunities.15 Bullies are often bi-strategic, employing both bullying and also acts of aggressive ‘prosocial’ behaviour to enhance their own position by acting in public and making the recipient dependent as they cannot reciprocate.16 Thus, pure bullies (but not bully/victims or victims) have been found to be strong, highly popular and to have good social and emotional understanding.17 Hence, bullies most likely do not have a conduct disorder. Moreover, unlike conduct disorder, bullies are found in all socioeconomic18 and ethnic groups.12 In contrast, victims have been described as withdrawn, unassertive, easily emotionally upset, and as having poor emotional or social understanding,17 ,19 while bully/victims tend to be aggressive, easily angered, low on popularity, frequently bullied by their siblings20 and come from families with lower socioeconomic status (SES),18 similar to children with conduct disorder.
How bullies operate
Bullying occurs in settings where individuals do not have a say concerning the group they want to be in. This is the situation for children in school classrooms or at home with siblings, and has been compared to being ‘caged’ with others. In an effort to establish a social network or hierarchy, bullies will try to exert their power with all children. Those who have an emotional reaction (eg, cry, run away, are upset) and have nobody or few to stand up for them, are the repeated targets of bullies. Bullies may get others to join in (laugh, tease, hit, spread rumours) as bystanders or even as henchmen (bully/victims). It has been shown that conditions that foster higher density and greater hierarchies in classrooms (inegalitarian conditions),21 at home22 or even in nations,23 increase bullying24 and the stability of bullying victimisation over time.25
Adverse consequences of being bullied
Until fairly recently, most studies on the effects of bullying were cross-sectional or just included brief follow-up periods, making it impossible to identify whether bullying is the cause or consequence of health problems. Thus, this review focuses mostly on prospective studies that were able to control for pre-existing health conditions, family situation and other exposures to violence (eg, family violence) in investigating the effects of being involved in bullying on subsequent health, self-harm and suicide, schooling, employment and social relationships.
Childhood and adolescence (6–17 years)
A fully referenced summary of the consequences of bullying during childhood and adolescence on prospectively studied outcomes up to the age of 17 years is shown in table 1. Children who were victims of bullying have been consistently found to be at higher risk for common somatic problems such as colds, or psychosomatic problems such as headaches, stomach aches or sleeping problems, and are more likely to take up smoking.39 ,40 Victims have also been reported to more often develop internalising problems and anxiety disorder or depression disorder.31 Genetically sensitive designs allowed comparison of monozygotic twins who are genetically identical and live in the same households but were discordant for experiences of bullying. Internalising problems was found to have increased over time only in those who were bullied,32 providing strong evidence that bullying rather than other factors explains increases in internalising problems. Furthermore, victims of bullying are at significantly increased risk of self-harm or thinking about suicide in adolescence.43 ,44 Furthermore, being bullied in primary school has been found to both predict borderline personality symptoms30 and psychotic experiences, such as hallucinations or delusions, by adolescence.37 Where investigated, those who were either exposed to several forms of bullying or were bullied over long periods of time (chronic bullying) tended to show more adverse effects.31 ,37 In contrast to the consistently moderate to strong relationships with somatic and mental health outcomes, the association between being bullied and poor academic functioning has not been as strong as expected.51 A meta-analysis only indicated a small negative effect of victimisation on mostly concurrent academic performance and the effects differed whether bullying was self-reported or by peers or teachers.47 Those studies that distinguished between victims and bully/victims usually reported that bully/victims had a slightly higher risk for somatic and mental health problems than pure victims.41 ,52 Furthermore, most studies considered bullies and bully/victims together; however, as outlined above, the two roles are quite different with bullies often highly competent manipulators and ringleaders, while bully/victims are described as impulsive and poor in regulating their emotions.53 We know little about the mental health outcomes of bullies in childhood, but there are some suggestions that they may also be at slightly increased risk of depression or self-harm,33 ,45 however, less so than victims. Similarly, the relationship between being a bully and somatic health is weaker than in bully/victims,39 or bullies have even been found to be healthier and stronger than children not involved in bullying.41 Bullying perpetration has been found to increase the risk of offending in adolescence;54 however, the analysis did not distinguish between bullies and bully/victims and did not include information about poly-victimisation (eg, being maltreated by parents). Bullies were also more likely to display delinquent behaviour and perpetrate dating violence by eighth grade.50
Consequences of involvement in bullying behaviour in childhood and adolescence on outcomes assessed up to 17 years of age
Childhood to adulthood (18–50 years)
Children who were victims of bullying have been consistently found to be at higher risk for internalising problems, in particular diagnoses of anxiety disorder55 and depression9 in young adulthood and middle adulthood (18–50 years of age) (table 2).56 Furthermore, victims were at increased risk for displaying psychotic experiences at age 188 and having suicidal ideation, attempts and completed suicides.56 Victims were also reported to have poor general health,65 including more bodily pain, headaches and slower recovery from illnesses.57 Moreover, victimised children were found to have lower educational qualifications, be worse at financial management57 and to earn less than their peers even at age 50.56 ,69 Victims were also reported to have more trouble making or keeping friends and to be less likely to live with a partner and have social support. No association between substance use, anti-social behaviour and victimisation was found. The studies that distinguished between victims and bully/victims showed that usually bully/victims had a slightly higher risk for anxiety, depression, psychotic experiences, suicide attempts and poor general health than pure victims.9 They also had even lower educational qualifications and trouble keeping a job and honouring financial obligations.57 ,65 In contrast to pure victims, bully/victims were at increased risk for displaying anti-social behaviour and were more likely to become a young parent.62 ,70 ,71 Again, we know less about pure bullies, but where studied, they were not found to be at increased risk for any mental or general health problems. Indeed, they were healthier than their peers, emotionally and physically.9 ,57 However, pure bullies may be more deviant and more likely to be less educated and to be unemployed.65 They have also been reported to be more likely to display anti-social behaviour, and be charged with serious crime, burglary or illegal drug use.58 ,59 ,66 However, many of these effects on delinquency may disappear when other adverse family circumstances are controlled for.57
Consequences of involvement in bullying behaviour in childhood/adolescence on outcomes in young adulthood and adulthood (18–50 years)
The findings from prospective child, adolescent and adult outcome studies are summarised in figure 1.

The impact of being bullied on functioning in teenagers and adulthood.
The carefully controlled prospective studies reviewed here provide a converging picture of the long-term effects of being bullied in childhood. First, the effects of being bullied extend beyond the consequences of other childhood adversity and adult abuse.9 In fact, when compared to the experience of having been placed into care in childhood, the effects of frequent bullying were as detrimental 40 years later56! Second, there is a dose–effect relationship between being victimised by peers and outcomes in adolescence and adulthood. Those who were bullied more frequently,56 more severely (ie, directly and indirectly)31 or more chronically (ie, over a longer period of time8) have worse outcomes. Third, even those who stopped being bullied during school age showed some lingering effects on their health, self-worth and quality of life years later compared to those never bullied72 but significantly less than those who remained victims for years (chronic victims). Fourth, where victims and bully/victims have been considered separately, bully/victims seem to show the poorest outcomes concerning mental health, economic adaptation, social relationships and early parenthood.8 ,9 ,62 ,70 Lastly, studies that distinguished between bullies and bully/victims found few adverse effects of being a pure bully on adult outcomes. This is consistent with a view that bullies are highly sophisticated social manipulators who are callous and show little empathy.73
Processes
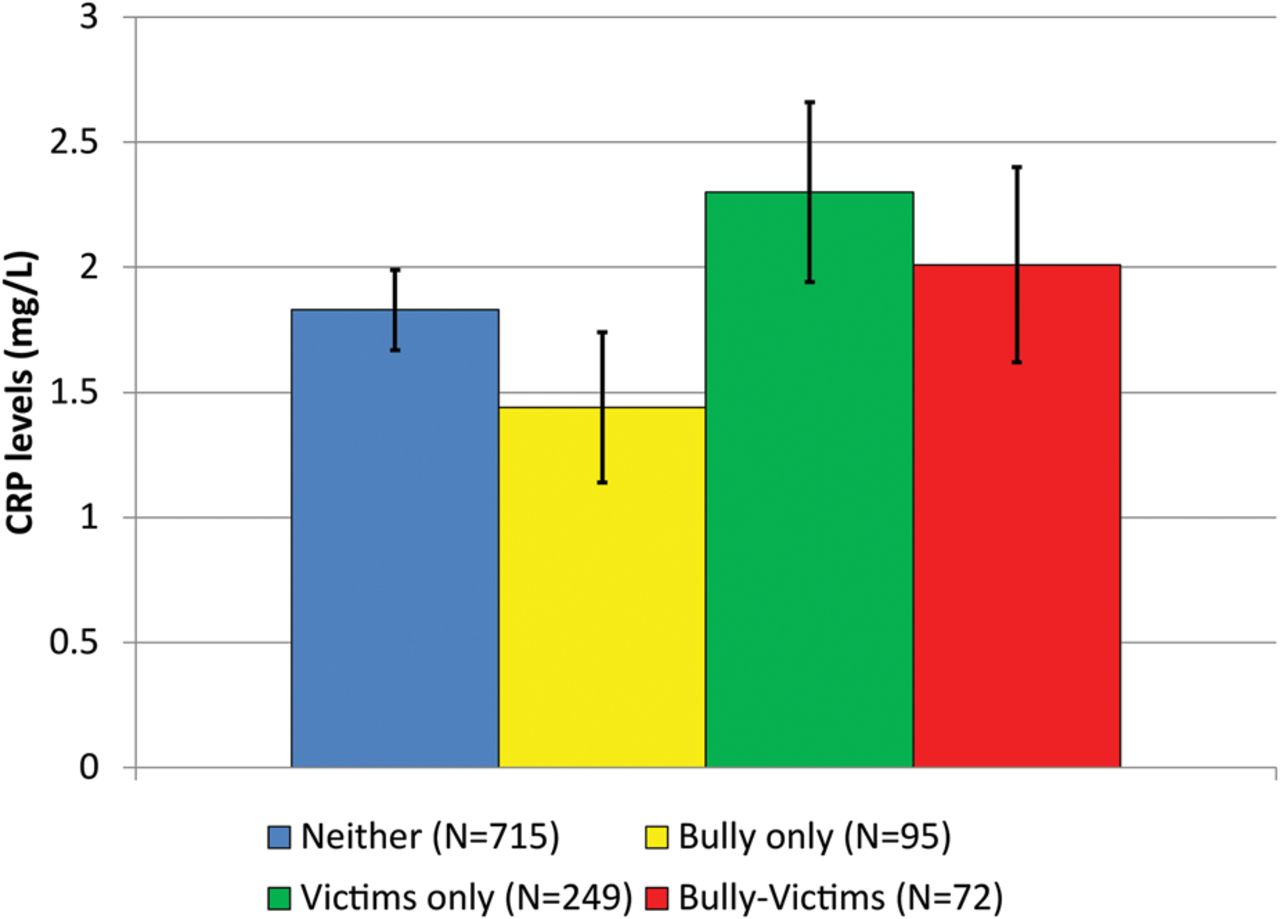
There are a variety of potential routes by which being victimised may affect later life outcomes. Being bullied may alter physiological responses to stress,74 interact with a genetic vulnerability such as variation in the serotonin transporter (5-HTT) gene,75 or affect telomere length (ageing) or the epigenome.76 Altered HPA-axis activity and altered cortisol responses may increase the risk for developing mental health problems77 and also increase susceptibility to illness by interfering with immune responses.78 In contrast, bullying may also differentially affect normal chronic inflammation and associated health problems that can persist into adulthood.64 Chronically raised C-reactive protein (CRP) levels, a marker of low-grade systemic inflammation in the body, increase the risk of cardiovascular diseases, metabolic disorders and mental health problems such as depression.79 Blood tests revealed that CRP levels in the blood of bullied children increased with the number of times they were bullied. Additional blood tests carried out on the children after they had reached 19 and 21 years of age revealed that those who were bullied as children had CRP levels more than twice as high as bullies, while bullies had CRP levels lower than those who were neither bullies nor victims (figure 2). Thus, bullying others appears to have a protective effect consistent with studies showing lower inflammation for individuals with higher socioeconomic status80 and studies with non-human primates showing health benefits for those higher in the social hierarchy.81 The clear implication of these findings is that both ends of the continuum of social status in peer relationships are important for inflammation levels and health status.
{kind=link}
{kind=link}
Adjusted mean young adult C-reactive protein (CRP) levels (mg/L) based on childhood/adolescent bullying status. These values are adjusted for baseline CRP levels as well as other CRP-related covariates. All analyses used robust SEs to account for repeated observations (reproduced from Copeland et al64).
Furthermore, experiences of threat by peers may alter cognitive responses to threatening situations.82 Both altered stress responses and altered social cognition (eg, being hypervigilant to hostile cues38) and neurocircuitry83 related to bullying exposure may affect social relationships with parents, friends and co-workers. Finally, victimisation, in particular of bully/victims, affects schooling and has been found to be associated with school absenteeism. In the UK alone, over 16 000 young people aged 11–15 are estimated to be absent from state school with bullying as the main reason, and 78 000 are absent where bullying is one of the reasons given for absence.84 The risk of failure to complete high school or college in chronic victims or bully/victims increases the risk of poorer income and job performance.57
Summary and implications
Childhood bullying has serious effects on health, resulting in substantial costs for individuals, their families and society at large. In the USA, it has been estimated that preventing high school bullying results in lifetime cost benefits of over $1.4 million per individual.85 In the UK alone, over 16 000 young people aged 11–15 are estimated to be absent from state school with bullying as the main reason, and 78 000 are absent where bullying is one of the reasons given for absence.86 Many bullied children suffer in silence, and are reluctant to tell their parents or teachers about their experiences, for fear of reprisals or because of shame.87 Up to 50% of children say they would rarely, or never, tell their parents, while between 35% and 60% would not tell their teacher.11
Considering this evidence of the ill effects of being bullied and the fact that children will have spent much more time with their peers than their parents by the time they reach 18 years of age, it is more than surprising that childhood bullying is not at the forefront as a major public health concern.88 Children are hardly ever asked about their peer relationships by health professionals. This may be because health professionals are poorly educated about bullying and find it difficult to raise the subject or deal with it.89 However, it is important considering that many children abstain from school due to bullying and related health problems and being bullied throws a long shadow over their lives. To prevent violence against the self (eg, self-harm) and reduce mental and somatic health problems, it is imperative for health practitioners to address bullying.
References
Footnotes
Contributors DW conceived the review, produced the first draft and revised it critically; STL contributed to the literature research and writing, and critically reviewed and approved the final version of the manuscript.
Funding This review was partly supported by the Economic and Social Research Council (ESRC) grant ES/K003593/1.
Competing interests None.
Provenance and peer review Commissioned; externally peer reviewed.