Article Text

Abstract
The past year has produced several new clinical guidelines germane to paediatric dermatology, as well as important work related to rheumatologic overlap disorders, psoriasis comorbidities, pigmented lesions and quality of life impact. This review highlights common diagnoses and treatments useful for the practicing paediatrician.
- Dermatology
- Vascular Disease
- Allergy
- Collagen Disorders
Statistics from Altmetric.com
Introduction
The past year has produced several new clinical guidelines germane to paediatric dermatology, as well as important work related to rheumatologic overlap disorders, psoriasis comorbidities, pigmented lesions and quality of life impact.1 Paediatricians increasingly will encounter skin concerns in office visits, and stand poised to provide early recognition, treatment or referral for multiple skin conditions.
Acne
Considerable evidence has demonstrated discrepant acne-prescribing patterns between paediatricians and dermatologists.2 Motivated, in part, by a desire for greater standardisation, Eichenfield et al3 released evidence-based recommendations for the diagnosis and treatment of paediatric acne endorsed by the American Academy of Pediatrics. Neonates and infants up to a year of age commonly have acne and related papulopustular eruptions; further workup for this age group is not recommended absent other concerning features. Conversely, mid-childhood acne (age 1–7 years) is unusual and warrants further workup by a paediatric endocrinologist for evidence of virilisation, and/or growth abnormalities that could suggest underlying endocrinopathy. Preadolescent acne, at as young as 7 years of age, may be one of the first signs of pubertal maturation. Workup in these patients beyond history and physical is generally unnecessary unless other evidence of hormonal abnormalities or systemic disease is present. For the purposes of stratification and rational treatment, acne is categorised as comedonal, inflammatory, or mixed, and the severity rated as mild, moderate, or severe. (figure 1)

Management of acne.
Mild acne refractory to over-the-counter remedies should first be treated with benzoyl peroxide (BP) or a topical retinoid. BP is more effective than salicylic acid in head-to-head trials, but can be irritating; starting at lower concentrations (2.5%) may improve tolerance. Topical antibiotics are not recommended as monotherapy given concerns for bacterial resistance; this is avoided with concurrent use of BP. Moderate acne may require topical combination therapy with BP and a retinoid, with or without a topical antibiotic. Alternatives include an oral antibiotic with a topical retinoid and BP. Second-generation tetracyclines are preferred due to ease of use, fewer absorption problems, and less frequent dosing. Tetracycline derivatives should not be used in children younger than 8 years old due to risk of dental staining. Alternatives could include different topical agents, systemic antibiotics or hormonal therapy for females. Eichenfield et al advise waiting until 1 year after menstruation to consider hormonal therapies to minimise potential impact on bone accrual. Isotretinoin should be considered if a considerable cystic component or scarring potential exists. Severe acne should prompt a lower threshold for aggressive treatment with this same list of options to prevent potentially permanent scarring. Moderate to severe acne can be associated with low self-esteem, depression and even suicidal ideation.4 If inadequate response is observed, referral to dermatology is appropriate.
Atopic eczema
Ring et al5 ,6 have used existing German evidence-based guidelines, the landmark Health Technology Assessment document,7 and the European Task Force on Atopic Dermatitis/European Academy of Dermatology and Venereology position paper as foundation for revising guidelines of care for atopic dermatitis. They affirm fundamental management principles including the primacy of cutaneous hydration, avoidance of known irritants and allergens, and safe use of topical anti-inflammatory therapy most commonly in the form of topical hydrocortisones. By grading available evidence it becomes abundantly clear that many of our recommendations rely on an incomplete evidence base; recommendations graded level A, or those resting on the strongest form of evidence (randomised controlled trials or meta-analysis of randomised controlled trials) are far outnumbered by those following consensus opinion. With this caveat, they expertly enumerate best clinical practice, and several areas of importance are highlighted (figure 2).
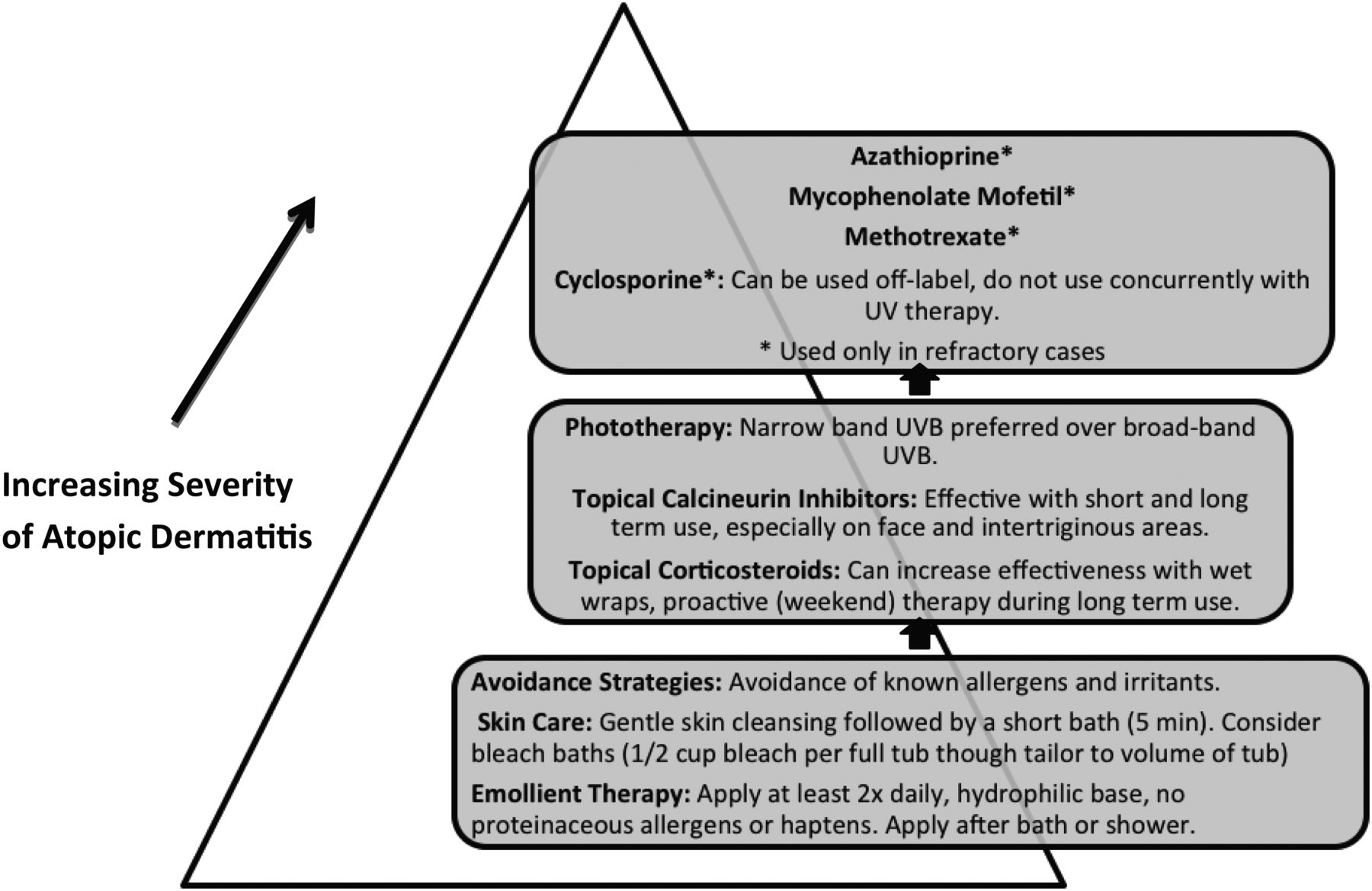
Management of atopic eczema.
The complicated relationship between food allergy and atopic eczema is likewise reviewed. There is a paucity of controlled trials showing effects of dietary intervention on atopic eczema. Recent release of food allergy guidelines crafted jointly by allergists and dermatologists under the auspices of the National Institutes of Health have provided useful instruction.8 Topical corticosteroids are first-line therapy, and ‘pro-active’ use twice weekly to sites of known flaring can help decrease tendency to relapse. Topical calcineurin inhibitors are effective non-steroidal alternatives, though their use has been complicated by theoretical safety concerns summarised by a boxed warning in 2005. There remains no evidence of increased malignancy risk associated with topical calcineurin inhibitor use.9 Adjunctive therapies, such as antihistamines and antibiotics, are used commonly though insufficient evidence exists to support first-generation or second-generation antihistamines for atopic eczema-related pruritus, and oral antibiotics have not been shown helpful absent clinical infection. Phototherapy is an option for atopic eczema patients, and narrow-band ultraviolet B is preferred over broad-band ultraviolet B.6 Topical steroids at the beginning of phototherapy can reduce flares, and patients should be counselled that all ultraviolet treatments pose increased risk of skin cancer. Systemic steroids have an unfavourable risk to benefit ratio in the treatment of atopic eczema. Cyclosporine can be used off-label in children and adolescent patients with severe or refractory atopic eczema, but should not be used concurrently with ultraviolet therapy because the incidence of cutaneous malignancies may increase.6 Other systemic therapies that may be appropriate to consider include mycophenolate mofetil, methotrexate and azathioprine.6 Referral to dermatology should occur prior to initiation of systemic therapies. Complementary and alternative remedies are also discussed, and are uniformly lacking in convincing evidence of efficacy. Finally, multidisciplinary educational programmes and dedicated atopic eczema ‘workshops’ have repeatedly been demonstrated to be both beneficial and cost effective.6 The American Academy of Dermatology will also soon publish revised guidelines for care of atopic eczema further codifying best practice.
Propranolol for infantile haemangioma
Since its serendipitous discovery in 2008,10 propranolol has become first-line therapy for haemangiomas requiring treatment well in advance of clinical trials proving efficacy or defining preferred protocols. Consequently, there exists tremendous variability in its use. The need for inpatient initiation has been one unsettled question with significant medico-economic implications. Many centres have hospitalised all patients for propranolol initiation for 48–72 h, whereas others manage entirely in the ambulatory setting. Drolet et al11 published consensus guidelines aimed at better standardisation. Infants less than 8 weeks of age corrected should be started in the inpatient setting, whereas, older infants may not require this level of care. Other key consensus recommendations include a target dose of 1–3 mg/kg/day, ideally divided three times a day; careful attention to risk of bronchospasm, hypoglycaemia, hypotension and bradycardia; and caution in the setting of PHACE syndrome (PHACE is a cutaneous neurovascular syndrome consisting of posterior fossa abnormalities, haemangioma, arterial lesions, cardiac abnormalities and eye abnormalities). Although PHACE syndrome is not an absolute contraindication, patients with both abnormal cerebrovasculature and aortic arch anomalies are at higher risk for stroke following propranolol initiation due to decreased blood pressure and resultant decreased flow through already compromised vessels. Other important conclusions are highlighted in the box 1.
Consensus meeting key learnings: (table 6, Drolet et al)
-
There are no FDA-approved indications for propranolol in paediatric patients in the USA.
-
There is significant uncertainty and divergence of opinion regarding safety monitoring and dose escalation for use of propranolol in infantile hemangioma.
-
ECG should be part of the pretreatment evaluation in any child when the HR is below normal, arrhythmia is detected on cardiac exam, or there is a family history of arrhythmias or maternal history of connective tissue disease.
-
Cardiac and aortic arch anomalies are commonly seen in PHACE syndrome and require echocardiography to assess intracardiac anatomy and function in at-risk children.
-
It is recommended that the 20 mg/5 mL preparation of propranolol be used.
-
The consensus group advocates that the daily dose of propranolol be divided into three times daily.
-
Regardless of the setting in which propranolol is initiated, it is recommended that the propranolol dose be titrated up to a target dose, starting at 1 mg/kg/day divided three times daily.
-
The peak effect of oral propranolol on HR and benzoyl peroxide (BP) is 1–3 h after administration.
-
Dose response is usually most dramatic after the first dose of propranolol.
-
Bradycardia may be the most reliable measurement of toxicity, because obtaining accurate BPs in infants may be challenging, and normative data for bradycardia are better established.
-
If a major escalation in dosage (>0.5 mg/kg/day) is indicated, the patient's HR should be assessed before, 1 and 2 h after the increased dose is administered.
-
Hypoglycaemia may be the most common serious complication in children treated with propranolol for infantile hemangioma.
-
Propranolol should be discontinued during intercurrent illness, especially in the setting of restricted oral intake, to prevent hypoglycaemia.
Formal US Food and Drug Administration and European Medicines Agency approval is pending recent completion of a large multicenter, multinational blinded trial, but to date, epidemiologic studies including meta-analyses, confirm propranolol's place as gold standard for treatment of endangering or deforming infantile haemangiomas.12
Kaposiform Hemangioendothelioma
Kaposiform Hemangioendothelioma, like infantile haemangioma, is a vascular tumour of infancy albeit far less commonly encountered. Though sometimes mistaken for haemangiomas, Kaposiform Hemangioendothelioma tends to be larger (>5 cm), firmer and darker in colour (figure 3). Kaposiform Hemangioendothelioma can be associated with potentially life-threatening consumptive coagulopathy (Kasabach–Merritt phenomenon) and ideal therapy is not standardised. Accordingly, Drolet et al13 released consensus-derived guidelines for the care of complicated Kaposiform Hemangioendothelioma. Initial work-up should include a complete blood count with platelets, coagulation studies, MRI with and without contrast to delineate deeper muscle and fascial involvement, as well as tissue biopsy. Kaposiform Hemangioendothelioma without Kasabach–Merritt phenomenon should initially be treated with oral prednisolone 2 mg/kg/day. If associated with Kasabach–Merritt phenomenon, vincristine 0.05 mg/kg/day and oral prednisolone or intravenous methylprednisolone 1.6 mg/kg/day is recommended. Surgical resection, while potentially curative, is often not viable due to the infiltrative patterns of the tumours, difficulty of obtaining clear surgical margins, and significant coagulopathy. Surgery is considered when the lesion is life-threatening, and the time required for medical treatment impractical; and as a secondary option after failure of medical treatment. Embolisation and antifibrinolytics, such as aminocaproic acid and tranexamic acid may be helpful in some patients. Radiation therapy, used historically, has an inferior risk–benefit profile. Propranolol has shown mixed results in Kaposiform Hemangioendothelioma, with one report of success and one case series showing little benefit.

Kaposiform Hemangioendothelioma on lower extremity.
Melanoma
Pigmented lesions present unique challenges in the paediatric population. Proportionate growth is expected; atypical variants, such as Spitz nevi and ‘eclipse type’ nevi are common; and congenital nevi are often large and variegated. Multiple cohorts have demonstrated distinct differences including over-representation of amelanotic melanomas.14 This is of growing importance, as the incidence of paediatric melanoma continues to rise, particularly in adolescent females. Cordoro et al described a large cohort study of paediatric melanoma, with the goal of updating the conventional ABCDE criterion to better represent paediatric melanomas.15 These authors propose the paediatric ABCDE criterion should reflect the following: ‘A’ should include amelanotic as well as asymmetric; ‘B’ for bump and bleeding as well as border irregularity; ‘C’ for colour uniformity and variegation; ‘D’ should stand for small diameters (<6 mm) as well as large. ‘E’ remains an important reminder that textural changes or ‘elevation’ can be significant. This is particularly true in giant congenital nevi where malignant transformation may occur in the deeper dermis without telltale change in clinical shape or colour. Vourc'h-Jourdain et al16 reviewed melanoma risk in large congenital melanocytic nevi and found that 2% of their patient cohort developed melanoma at an average age of 12.6 years, 55% of which were fatal. New recommendations of the categorisation of congenital melanocytic nevi were recently proposed,17 and are important in stratifying risk for adverse outcomes, such as melanoma. These criterion and classifications provide a more inclusive clinical toolkit for the evaluation of concerning pigmented lesions in paediatric populations.
Dermatologic manifestations of connective tissue disease
Recent work by Dickey et al reviewed the clinical characteristics of cutaneous lupus erythematosus at a paediatric referral centre.18 All subtypes were represented: acute (eg, malar rash); subacute; and chronic or discoid lupus. In this cohort, there was no evidence of progression from discoid lupus to systemic lupus (SLE). Izmirly et al19 showed that anti-SSA/Ro-positive mothers who were at high risk of having a child with cardiac neonatal lupus reduced recurrence in future pregnancies by use of hydroxychloroquine during the initial pregnancy (21.2–7.5%).
Torok et al found that treatment of localised scleroderma with a corticosteroid taper and parenteral methotrexate was effective without significant adverse effects.20 Zulian et al21 showed that 73.8% of patients responded to methotrexate, and 72.9% maintained complete remission for a mean of 25 months after a 3-month treatment course. Adverse effects were observed in 48.3% of patients, but were usually mild and did not necessitate discontinuation of treatment.
Pouessel et al found that the frequency of lung involvement in children with juvenile dermatomyositis warrants systemic respiratory testing with PFTs and measurements of respiratory muscle strength. If abnormal, a chest CT scan is recommended.22 Kozu et al23 found abnormal lipid profiles in 36% of patients with juvenile dermatomyositis in comparison to 16% of controls suggesting further systemic monitoring in patients with juvenile dermatomyositis.
Psoriasis
There is accumulating evidence that psoriasis is a multisystem inflammatory process. Skin and joint disease have long been recognised, however, newer evidence has linked psoriasis to metabolic syndrome, cardiovascular disease and depression.24 A German study of paediatric psoriasis and comorbidities found over-representation of hyperlipidaemia, obesity and hypertension.25 Kimball found that paediatric psoriasis patients are at significantly greater risk of developing a psychiatric disorder, such as anxiety or depression (5.13 vs 4.07% p<0.001%).26 Paediatricians should monitor for these potential comorbidities and be mindful of the tremendous impact psoriasis can have on quality of life. Varni et al27 found the impact of psoriasis on quality of life greater than that of diabetes and similar to asthma and arthritis. Chronicity, lack of perceived medical severity, and embarrassment may conspire to keep patient concerns unmentioned. Treatment options range from topical therapy, including emollients, topical corticosteroids and calcipotriene, to more aggressive modalities, such as systemic immunomodulators and phototherapy. Though purely paediatric guidelines do not exist, adult guidelines can be instructive.28 In their review of systemic therapy for paediatric psoriasis Marqueling and Cordoro29 suggest acitretin as a first-line choice for generalised pustular, diffuse guttate, or thin-plaque psoriasis. (figure 4)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Systemic treatment of paediatric psoriasis:
On account of teratogenicity concerns extending 3 years beyond exposure to acitretin, it must be used with extreme caution with appropriate contraceptive counselling and control measures in females of child-bearing potential. Acute flares of plaque, pustular, or erythrodermic psoriasis can be treated with methotrexate or cyclosporine. Tumour necrosis factor α inhibitors are recommended for refractory plaque or generalised pustular psoriasis, with etanercept having the most data to support use in children.30
Onychomycosis
Onychomycosis is uncommon in children (0.3%) compared with adults, and few studies exist to guide treatment. Gupta et al found that systemic antifungals resulted in a complete cure rate (defined as 100% visual clearing of the nail or clinical cure with negative fungal culture and potassium hydroxide microscopy) of 70.8% when used alone, and 80.0% when used in combination with a topical treatment.31 Continuous itraconazole (82.7%) was the most effective followed by continuous terbinafine (78.8%), pulsed itraconazole (68.4%), fluconazole (66.7%) and griseofulvin (6.3%). The authors conclude that safety and efficacy are similar to adult literature. This contrasts with the use of topical therapy alone, which results in woeful cure rates in adults (10%). Perhaps on account of anatomical differences, such as thinner nail plates in children, topical monotherapy can be effective. Friedlander et al presented a prospective, randomised, industry-sponsored, double-blinded vehicle-controlled study of treatment of non-matrix onychomycosis with ciclopirox lacquer applied daily for 32 weeks, with weekly removal of the lacquer and mechanical trimming.32 At the end of 32 weeks of treatment, 77% of the treated patients achieved mycologic cure and remained clear at 1 year of follow-up. Twenty percent of vehicle-treated patients cleared indicating that spontaneous improvement can likewise occur. These are useful data to recall when parents are challenged by the prospect of lab work and potential toxicity for an otherwise generally benign but irksome condition.
Coxsackievirus A6 (CVA6) hand foot and mouth disease
Hand foot and mouth disease due to coxsackievirus A16 is a common, easily recognised childhood illness characterised by fever, oral erosions and small, discrete, oval, deep-seated vesicles of the palms, soles and often buttocks. Mathes et al detail an outbreak, first reported in 2012, of an aggressive variant due to coxsackievirus A6 (CVA6).33 These authors describe 80 patients, aged 4 months–16 years (mean=1.5 years), from multiple centres across North America, nearly all of whom had a vesicobullous and erosive eruption. Sixty percent had greater than 10% body surface area involvement; the rash was often accentuated in areas of pre-existing eczema earning the moniker ‘eczema coxsackium’. Although most patients had fever and 1 in 10 were hospitalised, all did well with mean duration of illness 12.2 days. Nearly 1 in 4 patients developed distinctive onychomadesis, or nail shedding, in the convalescent stage. Diagnosis is clinical but can be confirmed with enteroviral PCR testing performed on swabs from vesicle fluid, oropharynx, perirectal skin, stool, or blood. CVA6 is difficult to culture, however, herpes simplex virus should be ruled out with fluorescent antibody and/or culture given clinical similarities to eczema herpeticum. Recognition of this striking presentation can prevent unnecessary antiviral therapy and parental angst.
Summary
This review highlights common diagnoses and treatments useful for the practicing paediatrician. A host of new guidelines and data aid in standardising best practice methods based on evidence-based recommendations. The unique manifestations of many dermatologic disorders in children and the complexities of adapting management plans to the paediatric population warrant continued focus and research.
References
Footnotes
-
Contributors Both authors contributed equally to the conception, research, writing and editing of this manuscript.
-
Competing interests KK: None declared. RS has served as an investigator and on an Advisory Board for Pierre Fabre Dermatology relating to the development of brand name ‘propranolol’ for infantile haemangioma. In the former capacity, he was not compensated; in the latter, he did receive financial compensation. RS has also served on an Advisory Board for Quinnova Pharmaceutical relating to a topical antifungal product not currently on the market. RS has served on an Advisory Board for Galderma Pharmaceutical called the Early Intervention Acne Council designed to identify fertile areas of investigation relating to preadolescent acne. He received financial compensation in this capacity. RS currently serves as an expert witness for Roche Pharmaceutical in a case alleging a causal connection between isotretinoin and inflammatory bowel disease. He is paid an hourly rate for his participation in this case.
-
Provenance and peer review Commissioned; externally peer reviewed.