Article Text

Abstract
Aims: To estimate the annual incidence of hospitalisations due to severe complications of varicella, describe the complications and estimate annual mortality.
Methods: Active surveillance throughout the UK and Ireland for 13 months by paediatricians notifying cases to the British Paediatric Surveillance Unit and completing a questionnaire. The case definition was any child aged <16 years hospitalised with complicated varicella, as defined by a list of conditions, or admitted to ICU/HDU with varicella.
Results: 188 cases were notified for the surveillance period, of which 112 (0.82/100 000 children/year) met the case definition and were not duplicates. Confirmed cases had a median age of 3 years (range 0–14). The complications were: bacteraemia/septic shock (n = 30), pneumonia (n = 30), encephalitis (n = 26), ataxia (n = 25), toxic shock syndrome/toxin-mediated disease (n = 14), necrotising fasciitis (n = 7), purpura fulminans/disseminated coagulopathy (n = 5), fulminant varicella (n = 5) and neonatal varicella (n = 3). 52 children (46%) had additional bacterial infections. Six deaths were due, or possibly due, to varicella, including one intrauterine death. Four of the other five children who died (ages 2–14 years) had a pre-existing medical condition. Sequelae on discharge were reported for 41 cases (40%), most frequently ataxia or skin scarring. The median length of hospital stay was 7 days (range 1–68).
Conclusions: This study provides a minimum estimate of severe complications and death resulting from varicella in children in the UK and Ireland. Most complications, excluding deaths, occur in otherwise healthy children and thus would be preventable only through a universal childhood immunisation programme.
Statistics from Altmetric.com
Varicella-zoster virus causes varicella (chickenpox) on primary infection and herpes zoster upon reactivation. Varicella is generally mild, but there is an increased risk of complications in immunocompromised individuals and neonates if maternal varicella is temporally close to birth. Nevertheless, severe complications can occur even in previously healthy children, including secondary bacterial infections, central nervous system manifestations and death.1 Approximately 90% of UK varicella cases occur in children less than 15 years of age, with the highest incidence in the 1–4-year-old age group.2–4
A safe and effective live-attenuated vaccine against varicella was developed in the 1970s.1 It is universally recommended in several countries, including the United States, Canada, Australia and Finland. The vaccine prevents varicella in 85% of immunised children, with 97% protection against severe disease.1 However, childhood varicella immunisation is not carried out routinely in the UK or Ireland, although two vaccines are licensed and recommended for seronegative healthcare workers, and certain high risk individuals and their seronegative contacts.5 There are few data on complicated varicella in either country and routine hospitalisation records cannot provide sufficiently detailed or accurate information.2 3 6 Therefore, the publication of data on severe complications of varicella will make a valuable contribution to the epidemiological and economic data available and help determine the advisability of current selective, or future universal, immunisation policies. The data also provide a baseline against which any policy change may be evaluated.
METHODS
Cases of severe complications of varicella in hospitalised children were identified using the British Paediatric Surveillance Unit methodology of active surveillance7 for the 13-month period November 2002–November 2003. Each month all consultant paediatricians (average n = 2309) across the UK and Ireland received a card with up to 12 conditions selected for surveillance. Paediatricians are asked to indicate whether they have seen a case or have “nothing to report”. The average card return rate during the study was 92.3%. The case definition was any child <16 years of age hospitalised with complicated varicella, as defined by list of clinical conditions (table 1), or admitted to ICU/HDU with varicella or one of its complications. The list of clinical conditions was determined by literature review and reference group consultations involving infectious disease paediatricians, virologists and public health specialists.
All reported cases were followed up by a questionnaire to the paediatrician. This requested limited patient identifiers (for de-duplication), clinical outcome, and length of stay information. Data were entered into an Access database, with data analysis in SPSS. Ethical approval was received from MREC Scotland.
RESULTS
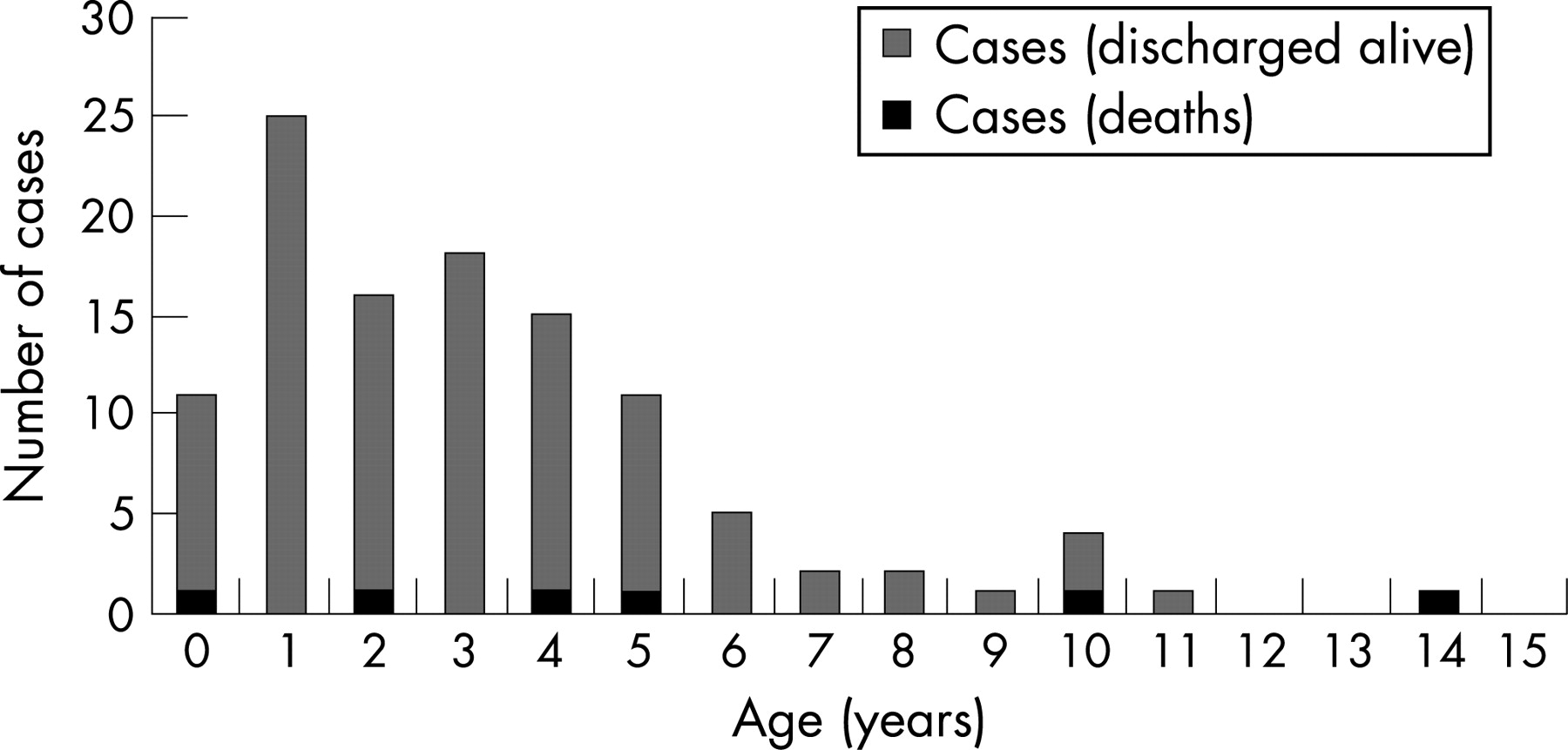
A total of 188 cases were reported, of which 112 (0.82/100 000 children per year) were non-duplicate confirmed cases meeting the case definition during the study period. In addition, there were 22 duplicates, 28 non-cases (did not meet case definition), six non-cases (outside the study period), six errors (eg, wrong box ticked) and 14 losses to follow-up (questionnaire not returned). The incidence of confirmed cases peaked in the spring, correlating with known seasonal varicella distribution, including notifications from Scotland for the same period (fig 1). The ages of confirmed cases ranged from birth to 14 years, with a median of 3 years and a mode of 1 year (fig 2). The annual population rates by age group were 2.32/100 000 (0–4 years), 0.54/100 000 (5–9 years) and 0.12/100 000 (9–15 years).


{kind=link}
{kind=link}
The frequency of case definition criteria for confirmed cases, median age and length of stay are shown in table 1. Of the 112 cases, 97 (87%) were diagnosed only clinically, one by laboratory testing alone (0.9%) and 14 on both clinical and laboratory diagnoses (12%). Laboratory diagnosis was most frequently serology, either alone (n = 6) or with other tests (n = 5), including PCR (n = 2), culture (n = 1), immunofluorescence (n = 1), or in one case, PCR, culture and immunofluorescence. Apart from serology, one case each was diagnosed by immunofluorescence alone, PCR alone, or a combination of PCR and electron microscopy or immunofluorescence and culture.
A concurrent or secondary bacterial infection was reported for 52 cases (46%). A breakdown of the sites and organisms involved is given in table 2.
Underlying medical conditions were reported for 18 cases (16%). Four cases (3%) were immunocompromised (hyposplenia, nephrotic syndrome, HIV, acute lymphatic leukaemia) and 14 had other chronic diseases and were predominantly single cases of different congenital abnormalities, with the exception of two cases each of Down syndrome and cerebral palsy. Only one case of asthma was cited. Only four of the 110 children (4%) for whom paediatricians could give a definite answer, had an underlying skin disorder (eczema n = 3, chronic bullous, disease n = 1).
Among the confirmed cases, six deaths were reported that were due, or possibly due, to varicella, including one intrauterine death (late second trimester). The ages of the other five children were 2, 4, 5, 10 and 14 years. Presentations were: 1) pneumonia; 2) bacteraemia and toxic shock syndrome/toxin-mediated disease; 3) bacteraemia, purpura fulminans/disseminated coagulopathy and pneumonia; 4) bacteraemia, purpura fulminans, pneumonia and fulminant varicella; and 5) multiple organ failure, acute respiratory distress syndrome, acute tubular necrosis and severe hepatic necrosis. Underlying health problems were reported for four of these deaths, including HIV, cerebral palsy (n = 2) and cardiac skeletal myopathy.
The median length of stay for all cases was 7 days (range <1–68 days), with a median ICU/HDU stay of 6 days (range <1–29 days; 27/112 cases; 24%). Time from admission to death was 3 days or less for all fatalities. The presence or absence of sequelae on discharge was reported for 102/112 cases, with 41 cases (37%; 0.30/100 000) having sequelae. These were mainly residual ataxia (n = 15; 13%) and skin scarring (n = 13; 12%).
DISCUSSION
This study confirms that severe complications of varicella, including death, continue to occur in the UK and Ireland.
By using active surveillance among all consultant paediatricians, we should have captured the overwhelming majority of severe varicella cases meeting the case definition among hospitalised children. The use of follow-up questionnaires meant we were able to categorise cases better as severe and capture more information than was previously available through routine records. Nevertheless, the figures obtained are minimum estimates as there may still have been under-ascertainment to an unknown degree, despite an extremely high response rate for cards (92.3%) and questionnaires (92.5%).
This study could not have included data on all varicella hospitalisations, as this would have been unmanageable with the methodology used, for which the BPSU specifies a limit of around 300 cases per year. It was therefore necessary to restrict ascertainment to severe cases. Initially, we considered achieving this limit by restricting the study to ICU/HDU admissions. However, it was decided that, as ICU/HDU admission criteria vary by location and bed availability, this might end up being a marker of management practice rather than severity, and capture only some cases. Indeed, only 27 (24%) of ascertained cases were admitted to ICU/HDU. We therefore decided to specify which clinical presentations would be considered as severe complications. This gave clear inclusion criteria but may have excluded other presentations considered just as severe. Indeed, 28 of the initial reports (15%), while reporting true varicella complications, did not meet the case definition. These included presentations of cellulitis, abscess or osteomyelitis in the absence of bacteraemia, cerebral infarct, acute renal failure, orchitis, idiopathic thrombocytopenic purpura, stroke and ataxia not requiring hospitalisation. It is worth emphasising that most children admitted to hospital in the UK and Ireland as a result of varicella will not have met our case definition. Such children often appear to have secondary bacterial infection of skin lesions, manifest by fever and cellulitis, yet infrequently have positive blood cultures or meet criteria for toxic shock syndrome or necrotising fasciitis.
This was the first active prospective epidemiological study for varicella in either the UK or Ireland. Previous studies in the UK have used retrospective analysis of routine hospital records. The most recent study found overall hospitalisation rates of 16.17 per 100 000 children aged 0–14 years,3 with highest rates among 0–4 year olds (38.7/100 000), decreasing almost 10-fold for children aged 5–14 years (4.6/100 000). This compares with an overall rate of 0.82/100 000 for severe complications in our study for children aged 0–15 years, highlighting the fact that most hospitalisations for varicella would not be captured by our case definition, mainly because they were less severe. UK varicella deaths have been reported previously, from routine statistics, to be an average of 4 (1991–2000),3 4.7 (1995–97),6 or 8.5 (1967–1985)8 deaths per year for children aged 0–14 years. Our figure of six deaths, including one intrauterine death, is within this range. The lower figures are for more recent years, which may reflect the wider use of prophylaxis in high-risk contacts and/or earlier treatment of high-risk cases. Immunosuppression was cited for 23% of the childhood deaths in the early study,8 compared to one (20%) of our post-natal deaths.
Internationally, there have been two recent active, prospective studies using methods similar to ours. A study by the German Paediatric Surveillance Unit found an equivalent rate for severe complications (0.85/100 000 children),9 although the case definition was different as it considered only neurological, bacterial superinfection and haematological complications above certain threshold criteria and excluded immunocompromised children. Strikingly, this study recorded no deaths, despite three fatalities being reported through routine statistics in Germany that year.9 However, these deaths may not have met the study case definition. The authors also reported a much lower rate of sequelae on discharge (4%), but again this may be due to differences in definitions. A similar study was also conducted by the Swiss Paediatric Surveillance Unit and estimated overall varicella hospitalisation as 5.9/100 000 in children aged 0–16 years. However, it was not possible to determine rates of specific complications and deaths, as varicella and herpes zoster figures were not separated.10
In addition to the above, there are many other, primarily retrospective, studies that report varicella complications, chiefly for all hospitalised cases, regardless of severity. The results of our study are generally concordant with these reports, although, as for the above, direct comparison is often difficult due to differing case ascertainment, case definitions, inclusion and exclusion criteria, classification of complication types, and the lack of population rates. However, a literature review shows that our median age of 3 years is within the reported median range of 2.8–4.3 years.11–18 It is difficult to compare the prevalence of risk factors among children with complications, for the reasons stated above, particularly as some studies excluded immunocompromised children. Comparison of specific complication rates is also difficult, as almost every study adopted different classification methods. For example, pneumonia could be classified as either an infectious or respiratory complication. Additionally, some studies reported figures for bacterial, viral and specifically varicella pneumonia separately, while others, like us, did not distinguish these from each other. However, it was possible to compare encephalitis rates directly with those in US retrospective and German prospective studies, for which figures were similar.9 19 Other studies from Turkey and Switzerland reported higher encephalitis rates (0.6/100 000 (95% CI 0.37 to 0.97) and 0.54/100 000 (95% CI 0.29 to 1.0) in children aged less than 16 years, respectively).13 20 We could also compare ataxia rates, which were approximately five to seven times lower in our study compared to those previously reported.13 19 20 This may be because we considered hospitalised cases only, and an exact case definition for ataxia was not specified. Rates for necrotising fasciitis in our study were approximately twice those observed in the recent German prospective study.9 We had a zero rate for Reye’s syndrome, consistent with four other recent studies.9 13 16 18 21 This is in contrast to earlier studies for which cases were reported,8 19 20 22–26 and may well reflect the success of public health strategies in preventing aspirin use in children. Our study identified three cases of neonatal varicella (0.40/100 000 live births; 95% CI 0.12 to 1.13). This figure seems very low compared to a recent study by the Australian Paediatric Surveillance Unit (5.8/100 000; 95% CI 4.3 to 7.8). However, that study considered all cases in infants aged less than 1 month, while our study specified perinatal infection. However, even when only babies whose mothers were infected within 1 week before or after birth were considered, the Australian rate remained much higher (3.9/100 000; 95% CI 2.7 to 5.6).27 The reasons for our lower rates are unclear but could include differing epidemiology and climate, clinical practice and reporting patterns.
One of the deaths reported in our study was in a child with HIV. High varicella mortality rates for HIV patients are not typical, with other studies reporting few deaths.28 29 However, fulminant varicella with concomitant cytomegalovirus presented with HIV in this individual.
Our finding of a high proportion of cases having infectious complications is similar to other studies.9–13 16 18–23 In particular, there has been recent concern over the relatively high number of invasive Group A Streptococcus infections,30 as found in our study.
What is already known on this topic
Severe complications of varicella can occur even in previously healthy children.
Varicella is vaccine preventable, but the UK does not recommend universal immunisation.
What this study adds
Severe complications of varicella, including death, continue to occur in the UK and Ireland
There are an estimated minimum of six deaths and 103 cases with severe complications each year in the UK and Ireland.
Most complications occur in otherwise healthy children and would be preventable only through universal immunisation.
For most of the children in this study, it is unclear why varicella presented so severely. A large majority had no underlying medical conditions. It is possible that strain variation could have played a role, but the study mechanism did not allow for collection of viral material for genetic analysis to test this hypothesis. Studies elsewhere, including in North America, Europe and Australia, have collected, or aim to collect, virological samples to address questions of virus variability and vaccine escape, as related to disease severity.31 32
Most of the cases were potentially preventable by vaccination of the individuals involved, that is, they occurred in immunocompetent children aged over 12 months. Further, studies elsewhere have shown that, even with only partial population uptake of varicella vaccine, substantial herd immunity can be achieved, extending protection to unvaccinated children aged less than 1 year.33 We did not identify any additional high-risk groups that could be candidates for selective immunisation. Universal vaccination would therefore be the only realistic option to prevent severe complications and deaths, as few, if any, could be identified as potentially preventable under the current UK policy. However, decisions around universal varicella vaccination are complex, and two particular theoretical concerns have been expressed in the UK.34 Firstly, there is concern that the introduction of universal varicella vaccination could cause an epidemiological shift with the age of varicella cases increasing, leading to an overall increased rate of complications. Secondly, as virus transmission in the community would decrease following vaccine introduction, this could cause an increase in herpes zoster in the elderly due to waning levels of immunity. Long-term data from countries that have already embarked on universal vaccination are awaited to address these concerns. Some preliminary data from one US study indicate a highly significant increase (90%) in zoster following a vaccine-associated decline in varicella,35 although this is in conflict with another large US study which does not indicate an increase.36 Positive efficacy and safety data on zoster vaccine for the elderly are also emerging.37 Zoster vaccine could potentially ameliorate the above concerns, should they occur, in addition to offering protection against re-activated varicella zoster infection.
Acknowledgments
We would like to thank all paediatricians who reported cases, the British Paediatric Surveillance Unit (BPSU) for allowing us to conduct the study under their auspices, Mr Richard Lynn BPSU Scientific Co-ordinator, and the additional members of the reference group who assisted in the original study design and proposal (Drs J Breuer, J Britto, J Edmunds, R Hague, N Hallam, I Jones, V Pavec and D Shingadia). We are especially grateful to Dr Ian Jones, former Director, SCIEH, who had a key role in study inception.
REFERENCES
Footnotes
Funding: The Scottish Centre for Infection and Environmental Health (now Health Protection Scotland) provided funding for this study.
Competing interests: Health Protection Scotland has received funding for research and conference attendance from pharmaceutical companies. RB and AF are occasionally supported by pharmaceutical companies to attend or present at scientific meetings; any fees offered are directed to a university research account. PTH has received funds from vaccine manufacturers to attend conferences and meetings, and St. George’s, University of London has received research grants from vaccine manufacturers on behalf of PTH.
Linked Articles
- Précis
- Varicella vaccine
- Atoms