Article Text

Abstract
Objective To compare the childhood urinary tract infection (UTI) guidelines from the Royal College of Physicians (RCP) in 1991 and from National Institute of Health and Care Excellence (NICE) (CG54) in 2007 by measuring their efficiency at detecting urinary tract abnormalities.
Design Children with UTIs within the Newcastle Primary Care Trust (population 70 800 children) were referred and imaged according to the RCP guidelines during 2008, and these were compared to the activity that would have been undertaken if we had implemented the CG54 guidelines, including following them through 2011 to identify those with recurrent UTIs.
Main outcome measures The numbers of children imaged, the imaging burden and efficiency, and urinary tract abnormalities detected by each guideline.
Results Fewer children would have been imaged by CG54 than RCP (150 vs 427), but its sensitivity was lower, at 44% for detecting scarring, 10% for identifying vesicoureteric reflux and 40% for other abnormalities. Overall, it would have only detected one-quarter of the abnormal cases (8 vs 32) and would have missed five of nine children with scarring, including three with multiple lesions and one with renal impairment. Imposing an age restriction of <8 years to the RCP guidelines would reduce its screening rate by 20% and still detect 90% of the abnormalities.
Interpretation The CG54 guidelines do not alter the imaging efficiency compared to the RCP guidelines, but they are considerably less sensitive.
- urinary tract infection
- vesicoureteric reflux
- renal scarring
- urinary tract imaging
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
What is already known
-
The previous RCP childhood urinary tract infection imaging guidelines result in many children being investigated for each abnormality found.
-
National Institute of Health and Care Excellence (NICE) introduced the CG54 guidelines to improve imaging efficiency by selecting higher risk cases.
-
The CG54 guidelines were not tested against existing guidelines before being introduced.
What this study adds
-
The CG54 guidelines have a similar efficiency to the existing Royal College of Physicians (RCP) guidelines, but their sensitivity for detecting scars, vesicoureteric reflux (VUR) or other renal tract abnormalities are only 0.4, 0.1 and 0.4.
-
The RCP guidelines can be made more efficient by restricting their routine use to children aged <8 years and still detect most children with scarring.
-
The NICE guidance should be reconsidered.
Introduction
From 1991, most UK paediatricians managed urinary tract infections (UTIs) according to recommendations from the Royal College of Physicians (RCP),1 but these generate a high imaging burden (table 1) and were not felt to substantially improve the outcomes for children. Thus, the National Institute of Health and Care Excellence (NICE) drew up new guidelines2 (CG54) in 2007 which were designed to reduce the imaging burden by investigating higher risk children, using the selection criteria summarised in table 2. The Newcastle GPs and the Newcastle upon Tyne Hospitals NICE Guideline Committee undertook a preimplementation audit of CG54 against their existing RCP-based guidelines because CG54 had not been trialled.
The imaging recommended for screening children following a UTI, according to the Newcastle guidelines, modified from the 1991 RCP publication
The imaging recommended for children following a UTI, according to the NICE CG54 guidelines, presented by age categories and clinical features. Atypical features are listed below
Patients and methods
In Newcastle, GPs serving a population of 70 800 children aged <16 years refer those who develop a proven UTI (defined as ≥105/mL colonies of a single uropathogen cultured from their urine) to a nurse-led direct-access service,3 where they are imaged using a protocol based upon the RPC guidelines.2 All children referred appropriately have an ultrasound and delayed dimercaptosuccinic acid (DMSA) scan after their first UTI (table 1). Infants aged <1 year also have a micturating cystogram to look for vesicoureteric reflux (VUR), as may children aged <4 years with recurrences. Children who have normal DMSA scans are not considered to be at risk of developing scars with a future UTI if they are over the age of 4 years or if they are younger but have been shown not to have VUR.
The GP referral information routinely collected by the direct-access service makes it simple to identify how each child would have been managed according to the CG54 guidelines,2 where the algorithm to decide upon renal tract imaging depends upon age, the presence of atypical features and recurrent infections (table 2). We audited all children referred during 2008 and followed them up for between 3 and 4 years, until the end of 2011 to identify cases with recurrent infections. This audit was designed to evaluate a potential service development, so did not require ethics committee approval. We analysed the results in four clinically appropriate age bands: <1, 1–3, 3–8 and 8–16 years.
Results
Five hundred and thirty-two children were referred for a proven UTI during 2008, but of these 53 were not considered to be genuine infections on culture criteria, and 29 patients did not attend any appointments (figure 1). Of the 450 children (80.0% girls) with a proven UTI who participated in the investigation programme, 427 (94.9%) were imaged according to the RCP-based protocol because it was their first recognised UTI, while 23 who had been investigated previously were not retested because their earlier imaging was considered to exclude the risk of future scarring; 150 children would have been imaged according to the CG54 guidelines. Among these, 24 (16%) were aged <6 months with a single typical UTI, 58 (39%) met the CG54 ‘atypical’ criteria (all by culturing non-Escherichia coli uropathogens) and 66 (44%) had a recurrent UTI either at presentation (23) or before the end of 2011. Thirty children had atypical and recurrent UTIs.
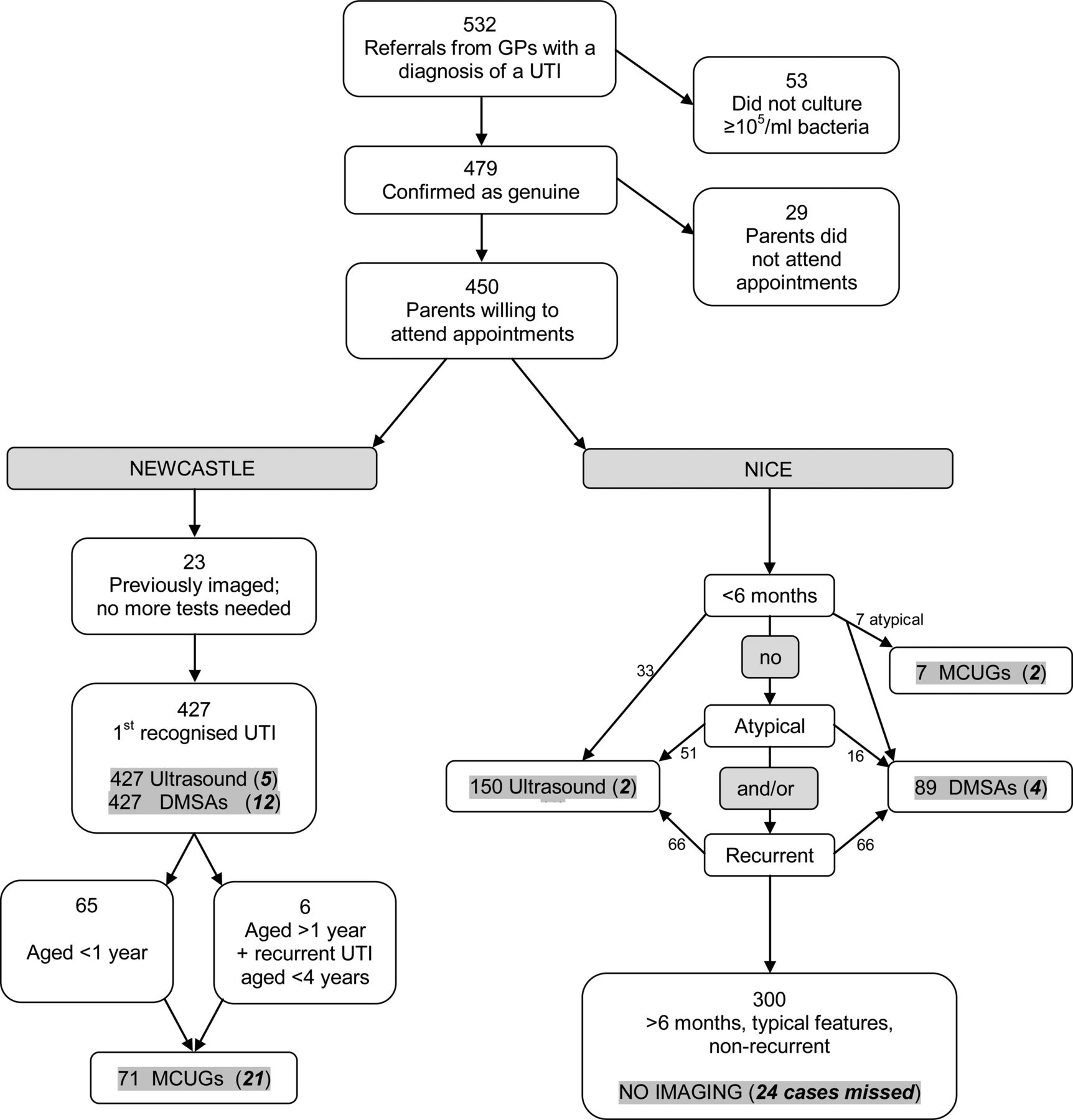
Flow chart showing the imaging that was undertaken on 532 children referred in Newcastle during 2008 with a possible urinary tract infection (UTI) following Royal College of Physicians (RCP)-based guidelines, and the imaging that would have been generated if National Institute of Health and Care Excellence (NICE's) CG54 had been followed. The numbers of imaging tests generated are indicated with shading, and the numbers of abnormal cases identified are shown in brackets.
The imaging outcomes and efficiency (number of children tested per abnormality detected) are shown in table 3 for both guidelines. The efficiencies for each test and for the overall imaging strategy were similar for both guidelines (p≥0.46 for all, Fisher's exact test), but CG54 would only have resulted in 35.1% of the children being tested. The RCP imaging schedule detected nine children with DMSA abnormalities consistent with scarring (6 with multiple lesions, 1 with a reduced kidney function), while CG54 would have detected 4 (3 multiple, none with renal impairment) and missed 5 (figure 2). The RCP-based guidelines detected VUR in 34 ureters in 21 children (grade ≥2 in 90%), while CG54 would have been identified bilateral grade 2 reflux in 2 babies with non-E coli UTIs. Ultrasound detected the fewest number of abnormalities, and only identified one child (with multiple renal cysts) whose other imaging was normal.
Newcastle children imaged after a UTI during 2008, abnormalities detected and imaging efficiency, according to RCP-based and CG54 guidelines

{kind=link}
{kind=link}
Dimercaptosuccinic acid (DMSA) scan pictures from five children whose kidney scars were detected by the Royal College of Physicians (RCP) investigation guideline, but were missed by the National Institute of Health and Care Excellence (NICE) guideline.
The specificity values of the CG54 tests to identify scarring, VUR or other abnormalities were all 1 compared to the RCP guideline results because they did not identify any extra positive findings. However, the sensitivities were generally considerably lower (table 4).
Sensitivity values for CG54 compared to using the RCP guideline, up to 8 years
Discussion
NICE's CG54 case selection criteria did not change the efficiency of their childhood UTI guidelines compared to the RCP-based ones. Following the CG54 guideline would have reduced the numbers of children tested by two-thirds, but would have missed over half of those who had scars, including those with multiple lesions. When following either protocol, approximately one-quarter of the cystograms undertaken demonstrated reflux. The value of detecting VUR is controversial, but we have identified a way in which this information may assist in preventing kidney scarring.4
If we had used the RCP-based guidelines but had restricted their routine use to children aged <8 years, that would have reduced the number of children imaged by about 20%, but would still have identified 90% of the abnormal cases, including eight of the nine children with scars. Reducing the limit to <4 years would have reduced the number of children imaged by about 50%, would still have identified about 80% of the abnormal cases, but would have missed nearly half (4/9) of the children with scars, of whom three had multiple scarring.
Footnotes
-
Contributors MGC and HJL conceived the idea of undertaking the project. All the authors designed the project and collected data. MGC drafted the article and all the authors reviewed the article for important intellectual content and approved the final version for publication. MGC is guarantor.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.