Article Text

Statistics from Altmetric.com
Introduction
In 2007, readers of the British Medical Journal voted that the introduction of clean water and sewerage—the ‘sanitation revolution’ of the Victorian era—was the most important medical milestone since the 1840s,1 over anaesthesia, antibiotics, or vaccines. These improvements led to a dramatic reduction in morbidity and mortality associated with faecal-oral infections, such as typhoid fever and cholera. Today, water, sanitation and hygiene (WSH) measures remain critically important to global public health, especially among children in lower income countries, who are at greatest risk from enteric infections and their associated symptoms, complications and sequelae.
In this article, we review the evidence linking WSH measures to faecal-oral diseases in children. Although continued research is needed, existing evidence from the last 150 years supports extending life-saving WSH measures to at-risk populations worldwide.2 One recent estimate3 held that 95% of diarrhoeal deaths in children under 5 years of age could be prevented by 2025, at a cost of US$6.715 billion, through targeted scale-up of proven, cost-effective, life-saving interventions. These include access to safe and accessible excreta disposal, support for basic hygiene practices such as hand washing with soap, and provision of a safe and reliable water supply. We present estimates of the burden of WSH-related disease followed by brief overviews of water, sanitation and hygiene-related transmission routes and control measures.i We conclude with a summary of current international targets and progress.
Transmission routes and health impact
Human excreta can contain over 50 known bacterial, viral, protozoan and helminthic pathogens. The majority of excreta-related infections are obtained through ingestion, less often through inhalation. Excreta-related infections travel through a variety of routes from one host to the next, either as a result of direct transmission through contaminated hands, or indirect transmission via contamination of drinking water, soil, utensils, food and flies (figure 1). The importance of each transmission route varies between pathogens and settings, and different pathogens are more prevalent in some populations.

The F-diagram, showing the different faecal-oral transmission routes, and possible barriers to prevent excreta-related pathogens from finding a new host.
Diarrhoea, malnutrition and environmental enteropathy
Although great strides have been made in reducing diarrhoea mortality, especially as a result of the increased use of oral rehydration therapy (ORT), diarrhoea remains the second leading cause of death in children under 5 years of age, after pneumonia.4 It is responsible for an estimated 1.7 billion cases of diarrhoea, or on average 2.9 episodes/child/year, and an estimated 1.87 million deaths among children under 5 years of age.5 The highest burden of disease is in children in the age range of 6–11 months: 4.5 episodes/child/year.6 It has been estimated that 50% of diarrhoea deaths can be attributed to persistent diarrhoea,7 and while ORT can prevent many deaths from acute diarrhoeal diseases,8 access to appropriate treatment is often limited in resource-poor settings.
The relationship between diarrhoeal disease and malnutrition is complex, though it is well accepted that malnourished children suffer more frequent episodes of diarrhoeal disease, while a child's nutritional status is affected following a diarrhoeal episode. A multiple country study found that 25% of stunting in children aged 24 months could be attributable to five or more diarrhoeal episodes experienced in the first 2 years of life.9 Malnutrition and stunting can lead to poorer school performance, early school drop-out and, as a result, lower economic well-being in later life.10 Over 440 million school days are missed annually due to WSH-related illnesses.11 Extended exposure to faecal pathogens may, in part, cause environmental enteropathy, a postulated condition (Humphrey, Lancet) characterised by malabsorption, villus atrophy, crypt hyperplasia, T-cell infiltration and general inflammation of the jejunum.12 This chronic infection of the small intestine could explain why sanitation may have a stronger association with gains in growth than with reductions in diarrhoea incidence.13 For example, a study in Peru found that diarrhoea could explain 16% of stunting, while access to sanitation and water services could explain 40%.14 Environmental enteropathy may reduce vaccine efficacy, either though induction of regulatory T cells which dampen the vaccine-specific immune response, or through the destruction of the live attenuated vaccine by an over-vigorous local immune response in the gut.15 This could explain why oral vaccines for the control of rotavirus have shown a lower efficacy in sub-Saharan Africa (39.3%) and Asia (48.3%), in contrast with efficacy in Europe/USA (85–98%).16–19
An estimated 88% of all child deaths as a result of diarrhoeal disease may be prevented through improvements in WSH.20 While there are promising emerging vaccines, including for rotavirus and cholera, there are several dozen pathogens transmitted in faeces, and WSH will remain critical to prevention of diarrhoeal diseases.
Helminths
Soil-transmitted helminths (STH); Ascaris lumbricoides, Trichuris trichiura and the human hookworms (Necator americanus and Ancylostoma duodenale) are our most common parasites and are estimated to infect up to 807 million, 604 million and 576 million people worldwide, respectively.21 Roughly a third of all Ascaris and Trichuris infections and 20% of hookworm infections are in children under the age of 15 years.22 STH ova leave the human body in excreta, and must mature in soil before they become infective. STH infections have shown a strong association with open defecation,23 and the use of fresh excreta or wastewater in agriculture.24 ,25 Consumption of dirt or soil (pica) by children, pregnant women, and others has also been suggested as a risk factor for STH.26 ,27 Schistosomiasis is estimated to infect 207 million people worldwide,21 and is caused by open defecation or anal cleansing28 close to or in water bodies where the miracidia can hatch and find a snail host to complete their lifecycle. The use of surface water sources like lakes, rivers and irrigation canals for domestic water needs, like washing, bathing and water collection have been associated with an increased risk of infection.29 Children are especially at risk as a result of their lower immunity, and because they may have more contact with contaminated water through play or water collection.30 Although direct mortality as a result of a helminth infection is low, morbidity is high. The global burden of disease has been variously estimated (as few as 3 million and as many as 50 million Disability Adjusted Life Year (DALY)31 ,32), and is uncertain but high.33 The burden of disease is attributable to the long-term impacts related to helminth infections, including anaemia, low birth weight, preterm birth, retarded growth, poorer cognitive performance and early school drop-out. Hookworm, in particular, is associated with undernutrition and possibly greater risk of malaria34–36 and HIV.37 ,38 The delivery of anthelminthics through schools has lately been the intervention of choice for reducing STH infections in children. The effectiveness of these programmes, especially with respect to improving cognitive performance, has recently been questioned, however, a large meta-analysis did not find a significant improvement,39 underscoring the need to interrupt transmission via effective sanitation in home and school environments.40
Prevention
Sanitation
Sanitation aims to prevent contamination of the environment by excreta and, therefore, to prevent transmission of pathogens that originate in faeces of an infected person. A wide range of technologies and methods exists to achieve this, which include sophisticated and high-cost methods like waterborne sewage systems and simple low-cost methods like the cat method, which involves the digging of a hole and covering faeces with soil after defecation. The WHO/UNICEF Joint Monitoring Programme (JMP) classifies the following as ‘improved’ sanitation that is more likely to be hygienic: a connection to a sewerage system, septic tanks, pour-flush toilets, ventilated improved pit latrines and pit latrines with a concrete slab. According to the 2010 JMP estimate, 11 countries make up 76% of the 2.5 billion people lacking improved sanitation, with one-third in India. Over one billion people practise open defecation, mostly in rural areas.41 Systematic reviews of the impact of sanitation on health have estimated a mean reduction of 32–36% in diarrhoea,42–44 though a Cochrane systematic review did not calculate a pooled effect due to heterogeneity of studies.45 The number of rigorous studies that have investigated the impact of sanitation on soil-transmitted helminth infections is very limited, as most of the sanitation interventions were conducted in conjunction with improvements in water supply. In Salvador, Brazil, neighbourhoods with storm water drains to prevent seasonal flooding with sewage, or full waterborne sewerage, were compared with neighbourhoods having neither. The study found that, when the level of community sanitation was better, the prevalence of ascariasis declined by up to 40%, and that domestic domain risk factors were more numerous and more significant in areas with better community sanitation.46
Safe child stool disposal
Many cultures consider the stools of infants fed on breast milk harmless, or at least less harmful than those of adults, because they are smaller, their faeces smell less, and contain less visual food residues.47–49 Additionally, most latrines are not designed for use of, and may not be used by, small children. They might be afraid to use them for the risk of falling in, bad smells, or the fear of dark spaces. Because nappies, child-sized potties and washing machines are not available in many poor settings, defecation on the floor is common and potentially seen as the most practical option until the child is potty trained. As a result, latrine use by children is low, as was shown by a study in Lima, Peru, where less than 25% of under five-year-olds used a toilet.49 Because of a much higher prevalence of diarrhoea and higher egg counts for STH in children, child stool often poses a greater health risk than those of adults.50 To date, safe disposal of children's stools has received relatively little attention in sanitation programmes.
Water supply
While all communities have access to water, the quantity and quality available may be insufficient to meet basic needs, and access may not be near to the household. The physically demanding job of water collection is usually allocated to women and children. A study in 25 countries in sub-Saharan Africa estimated that children spent a collective four million hours every day fetching water, and keeping them away from school.41 Carrying water can also lead to injuries and growth stunting.51 When water is available within 1 km, or a 30 min return round trip from the household, water use does not change significantly until water is provided on the plot or very nearby (figure 2). When a tap is available within the household, or shared with a close neighbour, per capita water use can go up from 10–30 L/person/day to 30–100 L/person/day. Greater volumes of water available to a household tend to result in better hygiene, including increased hand washing.
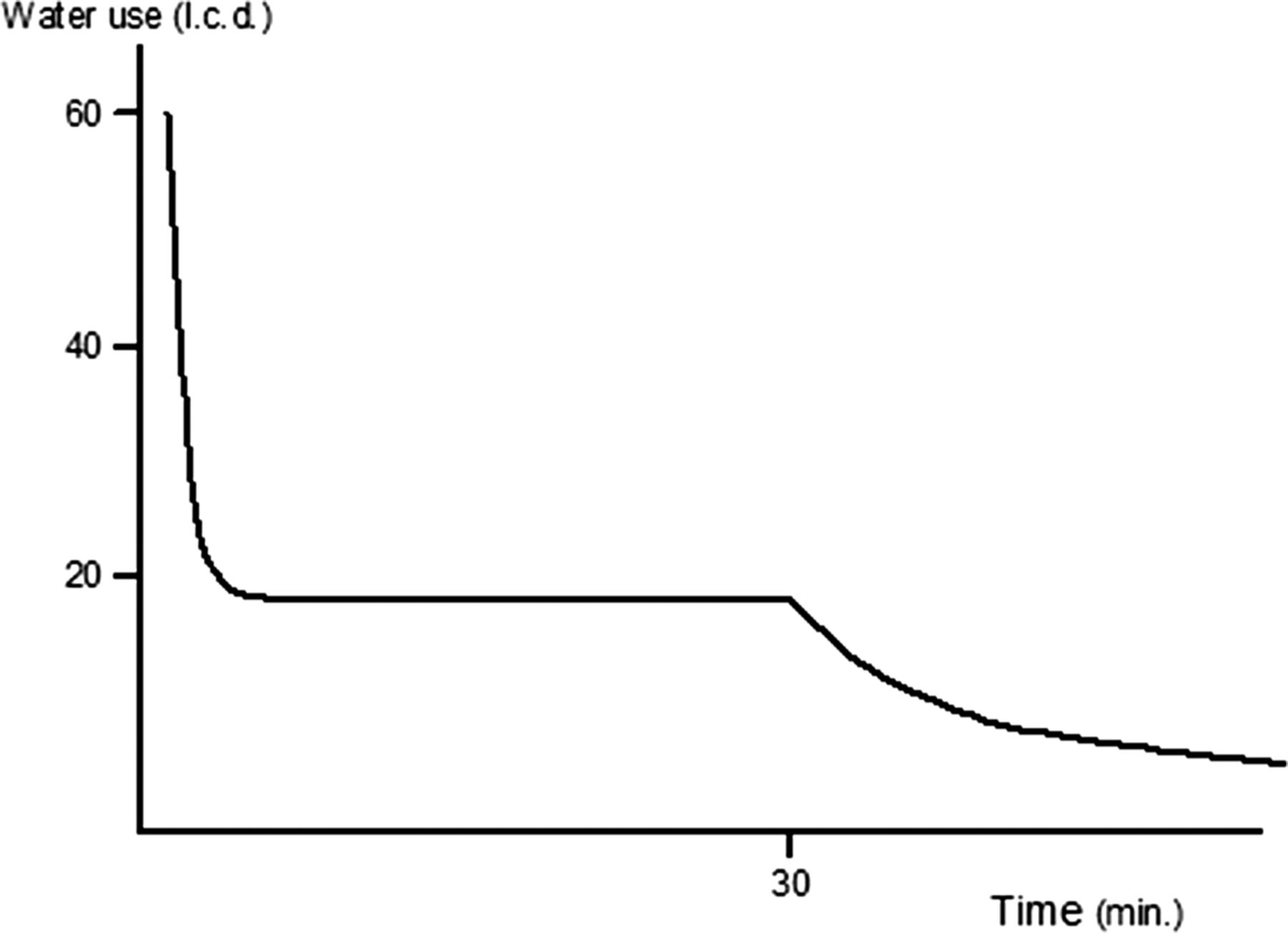
Distance to water source and use.

{kind=link}
{kind=link}
{kind=link}
An improved form of sanitation: a household pit latrine in Tanzania.
Over 780 million people now lack access to an ‘improved’ water source, and one study has estimated the number of people who rely on microbiologically or chemically unsafe water to be 1.8 billion, or about 28% of the global population.52 According to WHO/UNICEF JMP, ‘improved’ water sources include piped water, rainwater, protected springs and protected wells, which are thought to be less likely to be contaminated with pathogenic microbes. Recent research has shown, however, that even such improved water supplies may be subject to faecal contamination (ibid.) and that even occasional exposure to unsafe water—for example, from intermittent service or inadequate treatment—can undermine health benefits.53 Providing safe, reliable, piped-in water to every household is an essential goal, yielding optimal health gains, while contributing to the Millennium Development Goal (MDG) targets for poverty reduction, nutrition, childhood survival, school attendance, gender equity and environmental sustainability.
Food hygiene
Weaning food hygiene may be among the most important determinants of diarrhoeal disease risk in young children,54 ,55 although the current evidence is insufficient to arrive at conclusions about its relative importance in control of infections. It has been shown to be important in some contexts, with estimates of up to 70% of all diarrhoea caused by contaminated foods,54 and microbial counts that may exceed those found in drinking water.54–60 Food hygiene interventions, such as the promotion of reheating foods, preventing contact with flies and hand washing before feeding are the subject of current research, but effects on diarrhoeal disease risk have not been estimated from multiple trials. The sustained effects of behaviour change from food hygiene interventions have not been assessed.
Hand hygiene
Hand washing with soap before feeding children and after cleaning them can interrupt the transmission of faecal-oral microbes in the domestic environment. A review of the literature on hand hygiene suggests that hand washing with soap (HWWS) can reduce micro-organism levels close to zero,61 ,62 mainly through the mechanical action of rubbing and rinsing.62 ,63 Good hand washing practice should include water, a washing agent such as soap and a drying phase.50 ,64–66 Estimates of the impact of HWWS on health from systematic reviews suggest large effects (up to 48% reduction in diarrhoea).42 ,44 ,67–70 Hand washing with soap can also cut the risk of acute respiratory infections by 23%.71–73 Critically, persistent changes in behaviours may be possible following interventions,74 although more research is needed on the longer-term effects of behaviour change campaigns.
Water quality
Because universal safe, reliable, on-plot water supply remains an elusive goal for the majority of the world's population, household-level water treatment (HWT) has been proposed as an interim solution to provide safer drinking water at the point of use.75 ,76 In many settings, both rural and urban, populations may have access to sufficient quantities of water, but that water may be unsafe for consumption as a result of microbial or chemical contamination. Effective HWT, such as boiling, filtration or chlorination, has been shown to improve microbial water quality significantly.77–79 Safe storage of treated water is necessary to prevent recontamination through unsafe water handling.80
Improving water quality at the point of consumption can protect children from waterborne disease. The findings of meta-analyses show a much stronger protective effect for water quality interventions at the household level (rather than at source level) on diarrhoeal disease outcomes (up to 40%42 ,44 ,81: but no blinded trials of household water treatment have shown protective effects. HWT is unique among WSH interventions in that it may, in some forms, be possible to blind with a placebo device, chemical, or method. A review by Cairncross et al67 estimated diarrhoea risk reductions of 17% associated with improved water quality, which is consistent with earlier reviews by Esrey et al,43 ,68 and issues of bias potentially affecting the evidence base for water quality interventions have been articulated.81 ,82
One of the challenges that promoters of HWT have reported is low adherence—consistent, correct and sustained use—which can limit expected health gains.83 ,84 Unlike centrally treated, piped-in water supplies, HWT is normally a batch process that must be undertaken by the end users on a daily basis in order to provide consistent protection against waterborne pathogens. A number of studies of HWT have reported reduced use of interventions over time, suggesting that low adherence may limit the usefulness of HWT as a strategy.77 ,85–88
Progress toward and beyond the MDGs
Improvements in water supply and sanitation, if implemented sustainably, will have an important impact on a wide variety of different infectious diseases, and could improve the quality of life of millions of children worldwide, and provide them a proper start in life. In 2010, the UN General Assembly affirmed that clean drinking water and sanitation are human rights, with the UN Human Rights Council later recognising these rights to be derived from the rights to an adequate standard of living, health, life and dignity.41 These pronouncements cannot by themselves drive progress in expanding services, but do add moral weight to the pursuit of universal coverage. Although great strides have been made in the provision of sanitation and water, it is estimated that if current trends continue, 605 million people will still lack access to an improved water source in 2015, and 2.4 billion people will lack access to basic sanitation.41 Implementing better measures of what constitutes ‘access’ to water and sanitation—currently, monitoring is based primarily on technology types, without regard to key quality or accessibility factors—would paint an even bleaker picture of the global shortfall in coverage.
Households with a so-called ‘improved’ water supply connection that is intermittent and provides microbiologically unsafe water are counted among those with access to water meeting the MDG target for ‘sustainable access to safe drinking water’.89 Similarly, sanitation progress made in some areas have accounted only for construction of latrines, when there are no good options for treatment or disposal of waste after they fill up (figure 3).
In order to consolidate the gains of the last decade, and contribute to lowering the burden of childhood morbidity and mortality, post-MDG goals for water and sanitation should focus on strengthening key WSH institutions, creating demand and ownership, and fostering sustainable behaviour change. This requires an acknowledgment that the motivations for improving access are different for policy makers and intended recipients. The MDGs include language on reducing poverty and disease mortality, but for most of the beneficiaries the advantages and motives for the adoption of WSH measures are not directly health-related, but improvements in quality of life, including factors related to privacy, comfort, status, dignity, protection from harassment and savings in cost and time. Harnessing the power of these motivations to expand access to WSH, by leveraging investment by households—not only by governments and donor agencies—may help increase coverage of these life-saving measures among those who would most benefit from them.
References
Footnotes
-
Contributors All authors wrote and reviewed the paper, JHJE acts as guarantor of the content.
-
Funding SC's and JHJE's time was funded by the DFID research programme consortium on Sanitation and Hygiene (SHARE: grant no. P04990).
-
Competing interests None.
-
Provenance and peer review Commissioned; externally peer reviewed.
-
↵i Although we do cite pooled estimates of effect for WSH interventions on child health from a number of systematic reviews, readers should note that there is a rich emerging literature that attempts comparisons of impact between water supply, water quality, hygiene and sanitation; Waddington et al 2009 provides a good summary that is still current. WSH interventions are not very amenable to randomisation (in the case of infrastructure) and are almost never blinded in trials, with the exception of a minority of water quality intervention trials. Therefore, randomised, controlled trials (RCTs) may be subject to significant bias, and RCTs constitute the majority of studies included in systematic reviews of WSH interventions. We cite these reviews where appropriate as important but potentially flawed estimates that may be considered suggestive only. A broader perspective on the evidence base may be more helpful.