Article Text

Abstract
Background Technological advances in surgery, intensive care and medical support have led to substantial decrease in mortality for children with congenital heart defects (CHDs) over the last 50 years.
Methods Using routinely-collected mortality and population data for England and Wales from 1959 to 2009, the authors investigated age, period and birth cohort trends in child mortality attributable to CHDs.
Results The total number of deaths with CHDs at all ages between 1959 and 2009 was 61 903 (33 929 (55%) males). Absolute numbers of CHD-related deaths in children (under age 15 years) fell from 1460 in 1959 to 154 in 2009. Infants (aged under 1 year) comprised over 60% of all deaths due to CHD during the 5-year period 1959–1963, but this fell to 22% by 2004–2008. Age-standardised death rates have declined for both sexes but, despite narrowing sex differences, males continue to have higher death rates. Successive birth cohorts have experienced improved death rates in the first year of life; however, declining mortality across all age-groups has only been observed for birth cohorts originating after 1989. Poisson regression modelling predicts continuing generational decline in mortality.
Conclusions Death rates attributable to CHDs have fallen dramatically with advances in paediatric cardiac surgery and intensive care, largely due to decreased mortality in infants aged under 1 year. Initially, mortality in later childhood rose as infant deaths fell, suggesting death was delayed beyond infancy. Children born within the last 20 years experienced lower mortality throughout childhood.
Statistics from Altmetric.com
Introduction
Congenital heart defects (CHDs) are one of the most common types of congenital malformation in the UK and, without surgery, often incompatible with long-term survival. The birth prevalence of serious CHDs has remained stable at 6–8 per 1000 live births over several decades, although changes in the ascertainment of mild defects, associated with new technologies such as echocardiography, have been reported.1 ,2
Surgical intervention is usually required within the first year of life for serious CHDs; however, technological advances in paediatric cardiac surgery and medical care have led to marked improvements in survival during the last 50 years.3 Prior to these clinical advances, few children with serious CHDs survived into adulthood.4 ,5 Although early surgical techniques were introduced in the 1940s, more recent achievements have included the palliative Fontan operation, complete anatomical repair of transposition of the great arteries and the Norwood procedure. Intensive care, anaesthetic and medical therapies have also played a crucial role in supporting the development of complex surgical techniques, particularly for neonates. Despite the rising numbers of paediatric cardiac procedures being undertaken, mortality at 30 days after surgery is decreasing,6 and the number of UK adults with CHDs is growing by around 1600 per year.7
What is already known?
▶ Although infants under 1 year of age remain at greatest risk of premature death, CHD-related mortality has declined during the last 30 years.
▶ Survival into adulthood is likely for 80% children with CHDs who survive beyond their first year of life.
▶ Death rates are higher in males as compared with females but sex differences in mortality are decreasing as overall CHD mortality falls.
What this study adds?
▶ Infants comprised 63% of CHD deaths during 1959–63 but were 22% in 2004–08, coincident with 50 years of advances in neonatal and paediatric cardiac technologies.
▶ Death rates have improved for successive birth cohorts and a continuing decline in child and young adult mortality is predicted for future generations.
▶ As paediatric cardiac mortality continues to fall, exploration of the impact on adult cardiovascular mortality and the implications for future service provision is warranted.
Most studies exploring survival with CHDs are surgical case series, thus selectively present outcomes for individuals undergoing cardiac interventions within a single centre; however, retrospective cohort studies8 and smaller regional studies7 ,9 have also reported longer-term survival into adulthood with and without surgery. Some authors10,–,13 have examined longer-term changes in mortality for CHDs, using routine data from US (1979–1997; 1999–2006), UK (1994–2003) and Canadian (1987–2005) populations. While reporting declining overall CHD mortality, they noted significantly higher mortality in groups with severe CHDs,13 non-white ethnicity10 ,11 and males.11 ,12
Important influences on mortality include physiological ageing, secular (period) trends and birth cohort (generational) effects. Acquired heart disease or the physiological transition from fetal to neonatal circulation can increase the risk of death at specific ages. Generational influences are due to early life factors affecting individuals born at a similar time and exert a lasting effect. New technologies to correct CHDs in early life or improve prenatal detection might have a cohort effect. Crucially, no population-based birth cohort analyses have fully encompassed the changing CHD-associated mortality over the last 50 years coincident with advances in paediatric cardiac surgery. Understanding mortality within this context of marked technological change is essential to inform future clinical management and service provision for individuals born with CHDs today.
In this paper, we characterise trends in CHD-associated mortality by age and birth cohort, using routine death registrations for England and Wales between 1959 and 2009.
Methods
Details of deaths in England and Wales between 1959 and 2009, in which ‘congenital heart disease’ was coded as the primary or an underlying cause, were obtained from the Office for National Statistics (ONS). Deaths were recorded in electronic format from 1959. Four versions of the International Classification of Diseases (ICD) were used to code causes of death: ICD-7 (1958-1967), ICD-8 (1968-1978), ICD-9 (1979-2000) and ICD-10 (2001-current).14 ICD codes used are listed in the online supplementary table 1.
Deaths were obtained by year of death with information on calendar year of birth, age at death and sex. To avoid disclosure, data were aggregated into 5-year periods by year of birth and year of death; age at death was aggregated into 5-year intervals except for two age-groups representing death under 1 year (infants) and at 1 to 4 years of age. Children were defined as aged up to, but not including, 15 years. Some deaths (n=392), registered with ONS between January and March 1969, had no record of year of birth, although age at death was known. These cases were included in analyses by year of death but not year of birth, and sensitivity analyses were undertaken to estimate the effect of including these cases in analyses by year of birth.
Age and sex-specific death rates for each 5-year period were calculated using mid-year population estimates15,–,17 and standardised against the European population to facilitate comparison between time periods.18 Trends in age-specific death rates between 1959 and 2008 were examined for each sex by the year of death and 95% CIs for the age-standardised rate ratio for males and females estimated to determine statistically significant rate differences.18 ,19 Trends in age-specific death rates between 1959 and 2008 were examined for each birth cohort and future mortality up to age 44 years was predicted using a Poisson regression model based on the observed mortality data.20 Analyses were undertaken using StataSE V.10 (Timberlake Consulting).
Results
Number of deaths
The total number of deaths attributable to CHDs at all ages between 1959 and 2009 was 61 903 (33 929 (55%) males). Of these, 41 594 (23 124 (56%) boys) deaths occurred in children aged under 15 years (online supplementary table 2). The number of deaths in children (under age 15 years) fell from a total of 1460 (804 (55%) boys) in 1959 to 154 (89 (58%) boys) in 2009.
Most deaths associated with CHDs occurred within the first year of life, although deaths in infants aged under 1 year decreased steadily (figure 1). Deaths among children aged 1 to 9 years rose until 1969–1979 before beginning to decline. Deaths in 10 to 19 year olds remained stable until 1984–1988 and have fallen steadily over the last 30 years. Deaths among adults remained stable throughout, except in the oldest age group (aged 60 years or more) in which deaths increased until the period 1984–1993 before declining. These data suggest that children with CHDs are increasingly surviving into adulthood, yet no appreciable rise in adult deaths has yet been seen.

Number of deaths by age-group and year of death registration during the period 1959–2008, including International Classification of Diseases coding changes (logarithmic scale).
Analysis by period of death
The percentages of CHD-related deaths occurring in different age-groups, by period of death, are shown in figure 2. Infants comprised over 50% of CHD deaths until the period 1979–1983, but now represent 22% of all CHD deaths (online supplementary table 2). Conversely 21% of CHD deaths between 1959 and 1973 were adults, whereas the majority of deaths now occur within this age-range. Notably two periods of declining infant deaths in 1969–1978 and 1984–1993, coincident with new surgical techniques in the UK, were associated with temporary increases in deaths in children aged 1 to 14 years.

Trends in the percentage of all congenital heart defect-related deaths occurring at different ages.
CHDs were recorded as a cause in 9% (n=1860) of 21 673 child deaths (under age 15 years) in 1959 and in 3% (n=128) of 4570 child deaths occurring in 2008.
Age-standardised death rates
Age-standardised death rates at all ages, including adults and children, were estimated for each sex (figure 3). Mortality decreased for both sexes between 1959–1963 and 2004–2008; however, comparison of rate ratios indicated that males had a statistically significant higher death rate compared with females (data table included in figure 3).

Age-standardised death rates with congenital heart defects in England and Wales (1959–2008), by sex and year at death.
During the period 2004–2008, boys continued to have a significantly higher death rate than girls aged under 1 year or 5 to 14 years but no significant sex difference was seen for deaths in children aged 1 to 4 years (online supplementary figure S1).
The age-standardised death rate in infants under 1 year has remained significantly higher than for all older age-groups during the past 50 years. During the period 2004–2008, the death rate per 100 000 children aged 1 to 14 years was 0.53 (0.58, 0.48 for boys and girls respectively) compared with 14.70 (15.44, 13.92 for boys and girls respectively) per 100 000 infants aged under 1 year (rate difference 14.17 (95% CI 12.68 to 15.48), p<0.0001).
Birth cohort mortality
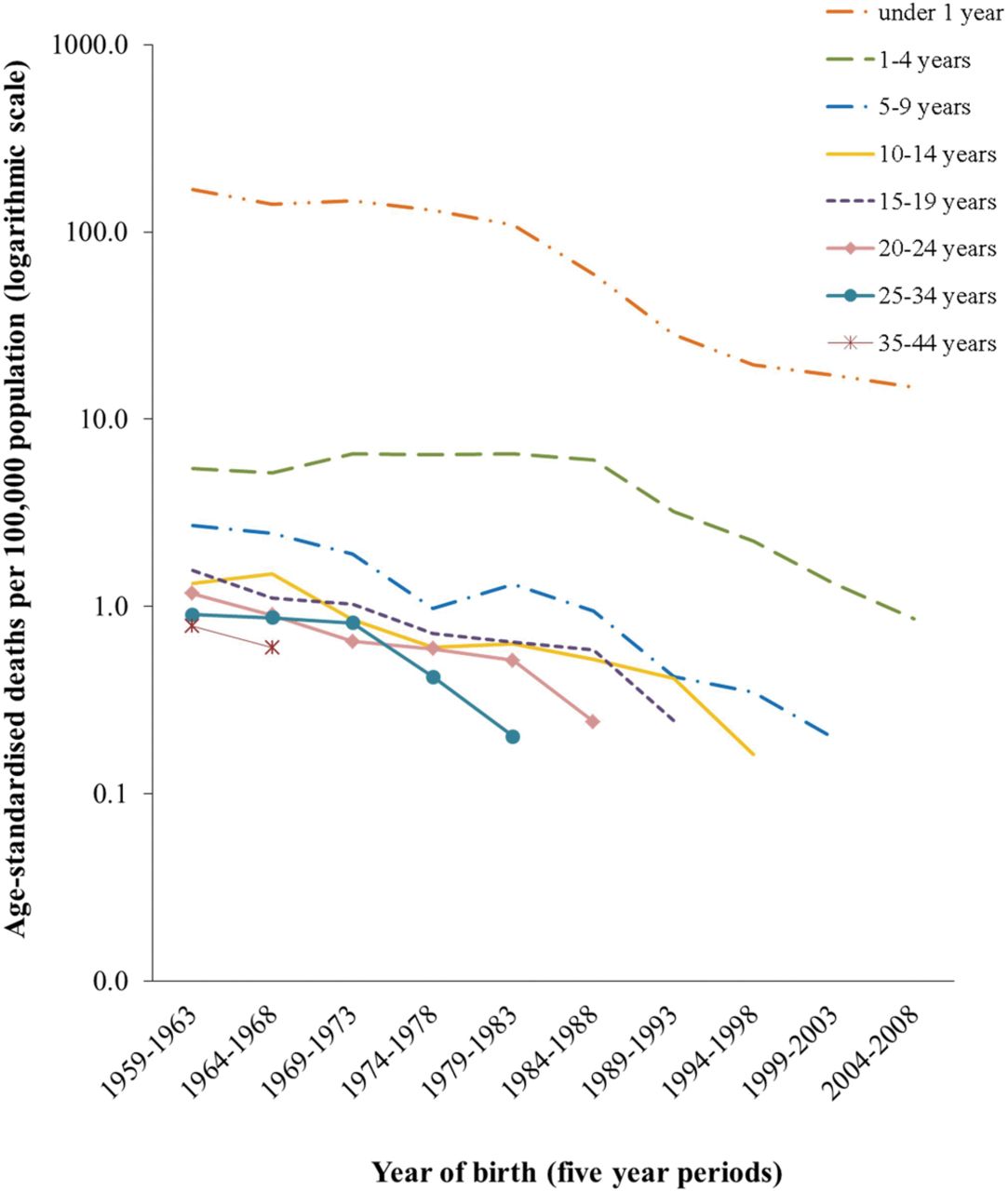
Age-standardised death rates (per 100 000 population) were similar for both sexes in successive 5-year birth cohorts (data not shown), therefore figure 4 includes all individuals. Within all 5-year birth cohorts since 1959, the highest death rates were experienced by infants under 1 year of age. Death rates in children under 1 year and over 5 years of age have improved for successive birth cohorts; however, improvement was greater for cohorts born after 1988. In early birth cohorts, there was no reduction in mortality within the age-group 1 to 4 years, which may be due to advances in neonatal care resulting in prolonged survival beyond infancy but with death occurring in the second to fifth years of life. The most recent birth cohorts, representing children born between 1989 and 2008, demonstrate appreciably lower death rates across all age-groups than previously reported.

Age-standardised death rates by birth cohort (England and Wales).
The uninterrupted lines in figure 4 indicate observed data points; these have been extended by interrupted lines to indicate predicted death rates using a Poisson regression model. These models suggest that improvements in mortality could continue for future generations although further follow-up will be needed to confirm these predictions.
In comparison with the birth cohort from 1959 to 1963, there has been a decline in mortality across all ‘age at death’ groups for individuals born during 2004–2008. Mortality under 1 year decreased for successive birth cohorts (figure 5), more dramatically after the period 1979–1983, whereas mortality at 1 to 4 years old increased in cohorts born before the period 1984–1988 then declined. These changes most likely reflect advances in neonatal management leading to decreased infant mortality in the 1980s but for some children death was only delayed.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Birth cohort analysis: age at death for different birth cohorts.
Discussion
This paper presents the first age-period-cohort analysis to explore long-term trends in population death rates for individuals with CHDs in England and Wales. We describe changes in mortality extending back over five decades during which major advances in paediatric cardiac surgery and intensive care have dramatically altered the survival outlook for affected individuals.
Since 1959–1963, there has been a 91% drop in the absolute number of CHD-related deaths in children under 15 years from 8039 to 722 in 2004–2008. The birth prevalence of serious CHDs remains stable,1 suggesting that this fall in mortality reflects prolonged survival. Whereas the majority (63%) of deaths in 1959–1963 were infants aged under 1 year, 67% of CHD-related deaths during 2004–2008 occurred in adults.
Age-standardised death rates for CHDs have declined steadily for both sexes yet, despite a narrowing of the sex difference, males continue to have significantly higher death rates than females. Analysis of generational influences indicates that death rates have improved for each successive birth cohort, particularly for those born since 1989, and a Poisson regression model based on these observations predicts a continuing decline in mortality.
Temporal trends in population-based mortality with CHDs have previously been reported,10 ,12 ,13 including demonstration of increasing age at death for some individual defects. Death rates estimated in our study, for successive time periods, are largely consistent with the previous findings although, unlike Billett,12 we found statistically significant sex differences persisting after 2004. However, our study data extend over a longer period of changing clinical management, thus permitting analyses of generational effects influencing CHD-related mortality.
Routine death registrations are a reliable source of population-based data, providing sufficient numbers for precise estimation of secular trends. However, birth cohort death rates in our study could not be extrapolated beyond 44 years of age due to the small number of observed deaths after this age. Deaths were aggregated across diagnostic groups and into 5-year age-bands to avoid the risk of identifying individuals, but this prevented comparisons between individual CHDs. Finally in the dataset provided by ONS, the birth year was missing for deaths in the first quarter of 1969. To address this, we undertook sensitivity analyses including these additional deaths, the results of which supported our original findings.
A key concern relating to routine data is the potential for misclassification by the cause of death. The Central Cardiac Audit Database recorded 126 deaths in children within 1 year of surgery performed during 2008–2009 within English and Welsh centres,6 slightly higher than the figure of 97 infant deaths recorded within our routine mortality dataset for 2009. This may reflect under-reporting of CHDs on death certificates for children who die of non-cardiac causes, such as prematurity. Some deaths in older adults may also reflect misclassification of acquired cardiac disease, for example, valve disease or acquired complications of congenital variants, thus inflating the number of deaths attributed to CHDs in these age-groups. However, these reasons for underascertainment do not vary between time periods so should not influence the secular trends reported here.
It is also possible that misclassification occurred during periods of transition between coding systems, as four versions of the ICD were used. Although such effects are known to occur,21 there was no evidence of discontinuity in our data (data not shown) and other authors have similarly failed to find any evidence of coding change influencing CHD death rates.12
Age-standardised death rates were highest for infants under the age of 1 year at all time periods. As children with CHDs survived infancy and into later childhood, our data show that falls in infant mortality in 1964–1973 and 1979–1993 were accompanied by rise in mortality at age 1 to 4 years. This suggests that a proportion of infants survived the first year of life but died before reaching school-age. Notably since 1989, the decline in infant deaths has been accompanied by a sustained decrease in deaths at all ages throughout childhood which may indicate that neonatal interventions now have greater capacity to prolong survival with CHDs and is consistent with reports of a growing adult population with CHDs.7 Interestingly, falls in infant mortality in the 1970s and 1980s appear coincident with the wider use of cardiopulmonary bypass and introduction of prostaglandin infusions to support infants prior to surgery. Continuing reductions in death rates may reflect the increasing preference for primary neonatal surgical repair, such as the arterial switch operation.22
Prenatal detection of CHDs, providing parents with choice about termination of an affected pregnancy, also influences mortality with CHDs as it results in disproportionate termination of fetuses with more severe defects, such as hypoplastic left heart or univentricular hearts.23,–,26 If pregnancies affected by these severe defects are terminated then the spectrum of defects at term will include fewer life-threatening defects for which palliative terminal care (without intervention) is more likely to be chosen by parents. Mortality in the first year of life would therefore appear to be lower because these children would no longer appear within the routine postnatal death data used here. Abortion statistics for England and Wales demonstrate that around 100–150 abortions are undertaken each year because of cardiovascular malformations in the fetus.27 Prenatal screening, though available in the UK for three decades, demonstrates differences in regional detection rates and the probability of detection for different defects.23 ,25
Follow-up of recent birth cohorts are too limited to assess the true impact on adult mortality of contemporary management of CHDs, particularly as those currently reaching older ages are likely to be the ‘healthy survivors’ from early birth cohorts.
This is the first UK study to explore both age and birth cohort trends in CHD-related death rates throughout the five decades during which major innovations in medical, surgical and intensive care have dramatically altered the outlook for affected individuals in Europe and North America. Our data clearly reflect the shift in the burden of CHD mortality from infancy to early childhood but demonstrate that this was initially accompanied by a rise in deaths between 1 and 4 years, It is significant that reduced mortality has only been realised across all child age-groups for births since 1989 and that sex differences in death rates still persist.
Crucially, the decline in CHD-related mortality in children and young adults born in the most recent decade shows no signs of stabilising; however, further observation of more recent birth cohorts is warranted to confirm these trends and to explore the impact on late adult mortality of extended childhood survival with CHDs.
Acknowledgments
The authors are grateful to staff at the Office for National Statistics for providing us with national mortality datasets.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Web Only Data - This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Web Only Data - This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
{kind=link}
Footnotes
-
Funding British Heart Foundation: MRC Special Training Fellowship MRC support to the MRC Centre of Epidemiology for Child Health.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement The data used in this study were obtained from the Office for National Statistics mortality data (public death registrations) and are available from this source.