Article Text

Abstract
Objectives To estimate the effect of cranial osteopathy on the general health and wellbeing, including physical functioning, of children with cerebral palsy.
Design Pragmatic randomised controlled trial.
Participants 142 children from Greater London and the South West of England, aged 5–12 years with cerebral palsy.
Intervention Participants were randomised to six sessions of cranial osteopathy with a registered osteopath or a waiting list with partial attention control (parents invited to participate in two semistructured interviews).
Primary outcome measures Blind assessment of motor function by physiotherapists using the Gross Motor Function Measure-66 (GMFM-66) and quality of life using the Child Health Questionnaire (CHQ) PF50 at 6 months.
Secondary outcome measures Parents' assessment of global health and sleep at 6 months, pain and sleep diaries at 10 weeks and 6 months, CHQ PF50 at 10 weeks and quality of life of main carer (Short Form 36) at 10 weeks and 6 months.
Results Compared with children in the control group, children in the osteopathy group demonstrated no statistically significant differences in GMFM-66 (mean difference 4.9, 95% CI −4.4 to 14.1), CHQ Physical Summary Score (mean difference 2.2, 95% CI −3.5 to 8.0) or CHQ Psychological Summary Score (mean difference 3.4, 95% CI −0.8 to 7.7). There were no significant differences between groups with respect to pain; sleep (either ‘time asleep’ or ‘time to sleep’); or main carer's quality of life.
Compared with children in the control group, carers of children receiving cranial osteopathy were nearly twice as likely to report that their child's global health had ‘improved’ at 6 months rather than ‘decreased’ or ‘remained the same’ (38% vs 18%; odds ratio 2.8, 95% CI 1.1 to 6.9).
Conclusions This trial found no statistically significant evidence that cranial osteopathy leads to sustained improvement in motor function, pain, sleep or quality of life in children aged 5–12 years with cerebral palsy nor in quality of life of their carers.
Trial Registration ISRCTN45840554 http://www.controlled-trials.com
Statistics from Altmetric.com
Introduction
Cerebral palsy (CP) is one of the commonest causes of neuro-disability in childhood, with a prevalence of around two per 1000 live births.1 The underlying neurological impairment is not susceptible to treatment and the goals of management are to promote function, to prevent secondary impairments and, above all, to increase a child's developmental capabilities.2
What is already known on this topic
▶ Many parents of children with cerebral palsy (CP) try various complementary and alternative medicine (CAM) therapies to try and reduce their child's symptoms and enhance their wellbeing.
▶ The evidence base for many CAM therapies, including osteopathy, is not strong, particularly in children.
What this study adds
There is no strong evidence to suggest cranial osteopathy improves health or quality of life of children aged 5–12 years with CP.
Many parents of children with CP try complementary and alternative medicine (CAM) therapies. In a survey conducted by the Cerebra Foundation,3 a charity for ‘brain injured’ children and young people, the most popular CAM therapies used by families were massage and cranial osteopathy.4 One of the most frequent queries received by the Cerebra Foundation telephone helpline is the extent to which the use of cranial osteopathy benefits children with CP. This led the Foundation to commission our research group to conduct first a systematic review of the evidence and then primary research to address this question.
Osteopathic treatment is described as consisting of the diagnosis of the musculo-skeletal strain patterns within the body, followed by techniques to release those strains.5 The fundamental principle of osteopathy is that the body as a whole is a dynamic interplay between its structure and its function. Osteopaths are trained to assess areas of ‘tension and compression’ as manifestations of disturbed function which they believe affect blood supply nerve function and cerebrospinal fluid flow. By working on these areas of tension, the osteopath aims to improve coordination of structure and function. Cranial osteopathy refers to a group of techniques, rather than a type of osteopathy. Specifically, cranial osteopathic techniques are said to enable osteopaths to palpate and treat using very small movements and the application of small amounts of force. Osteopaths believe that this enables them to treat the whole body including the central nervous system, the skeleton and the viscera. Hence, cranial osteopathy that children receive is highly individualised and is probably best characterised as a group of techniques rather than a specific treatment.
The evidence base for CAM therapies is not strong, particularly in children.6 The authors were able to identify only two trials which examined the effectiveness of cranial osteopathy in children with CP. Duncan et al7 reported that in their study, in which 50 children with CP were randomly allocated to cranial osteopathy, acupuncture or a waiting list, most parents said their children improved with either treatment 6 months postbaseline, compared with very few reporting improvement of those on the waiting list. The same group8 reported a second study with the same treatment comparison over a 6-month period (n=55). They reported the results as showing that cranial osteopathic treatment led to improvement in gross motor function but limitations in the design and approach to analysis make the results difficult to interpret.
As part of the preparation for this study the authors interviewed 12 osteopaths9 who provide treatment to children with CP, to ensure that any study would be considered a ‘fair test’ of the therapy. The key principle suggested was that treatment should be individually designed. There was agreement that a course of around six treatments with the same practitioner, beginning with three treatments at approximately 2-weekly intervals, would be a fairly standard approach for children with CP and that an impact would be expected on overall quality of life motor function, sleep, pain and fits. Parent members of Cerebra were also interviewed to ensure an acceptable trial design and that appropriate outcome measures were included.10
The primary aim of this study was to estimate the effect of individualised treatment by an osteopath on the general health and wellbeing, including physical functioning, of children with CP and on the quality of life of their main carer.
Methods
Between November 2006 and March 2008 the authors recruited children aged 5–12 years with CP with varying levels of function (categories II–V of the parent rated Gross Motor Function Classification System, GMFCS11), living in the South West of England or Greater London area. Children with mild CP, those who had received cranial osteopathy in the previous 12 months and those from non-English speaking families were excluded. The study was publicised through clinicians, physiotherapists, special schools and parents' groups. One of the research team visited potentially interested families at home and obtained written informed consent from parents or legal guardians. At enrolment and before randomisation, children were assigned a GMFCS category on the basis of questions answered by the parents,12 with the opportunity to consult with a clinical member of the research team if the categorisation was in doubt. The GMFCS categories are highly predictive of scores on the Gross Motor Function Measure (GMFM), one of the primary outcome measures.12 Parents also completed baseline data, including a measure of the strength of their belief that cranial osteopathy was likely to be beneficial, the Child Health Questionnaire (CHQ) PF50,13 the paediatric pain profile (PPP),14 a sleep and fit diary and the Short Form 36 (SF-36) for the main carer.15
After enrolment, children were allocated to intervention or waiting list (with partial attention control) using a telephone-based randomisation service provided by an independent statistician at a remote site using the computer programme Minim. Minimisation16 was used to ensure balance on the following factors: centre (London or Devon);
severity – categorised as either ‘less functional’ (GMFCS11 categories IV and V) or ‘more functional’ (GMFCS11 categories II and III);
age – younger (5 years) and older (6–12 years) and
beliefs of efficacy – whether parents had ‘strong’ or ‘not strong’ prior beliefs that cranial osteopathy was likely to help their child.
Children randomised to the intervention arm were invited to have six cranial osteopathy sessions: three in the first 10 weeks and the remaining sessions within the 6-month study period. Treatment took place in one of four practices (London, Exeter, Paignton and Plymouth) and all practitioners were experienced, qualified osteopaths, registered to practice with the General Osteopathic Council. No attempt was made to constrain the form of osteopathic therapy given. Each child was assigned an osteopath who planned the course of therapy based on their assessment of the child's individual needs. A total of 37 osteopaths provided treatment.
In order to provide a partial attention control, parents of children allocated to the 6-month waiting list were invited to take part in two semistructured interviews to ascertain their views of services for their children and their decision making about CAM therapies. After children in the control group had completed the final assessment at 6 months, they were given a voucher entitling them to six prepaid sessions of cranial osteopathy.
Parents were asked that their child not begin any new CAM therapies while in the trial and to continue with their usual management as recommended by the health and education professionals working with the family.
To detect a clinically significant difference between groups of 0.6 SDs in the primary outcome measures, the GMFM-6617 and the CHQ PF50,13 with 90% power and at the 5% significance level, 60 children were needed in each group (120 children in total). The authors planned to recruit a total of 150 children to allow for a possible 20% loss to follow-up. Parents and osteopaths completed forms after each treatment session to monitor compliance.
Outcome measures
The primary outcome measures were the GMFM-6617 and the CHQ PF50,13 at 6 months after study entry. The GMFM-6617 is a validated measure of motor function in children with CP, widely used in clinical trials. Assessments were carried out by a team of four experienced physiotherapists, trained in completing the GMFM-66 assessment and not aware of the child's allocated group, at 6-month follow-up only. Twelve per cent of assessments were double scored to evaluate the reproducibility between raters. Assessors were asked to note whether they had become un-masked to a child's allocated group during the assessment.
The CHQ is a carer-completed questionnaire which provides a generic measure of children's quality of life. This has been widely used in children with CP.18,–,20 Carers completed the CHQ at baseline, 10 weeks and 6 months after allocation.
Secondary outcome measures included the PPP,14 which recorded parents' views of their child's pain. Children's sleeping patterns were recorded using a 7-day diary, adapted from a diary designed for use in a trial of behavioural treatment of sleep problems.21 This allows recording of both time to settle and time spent asleep. Carers were asked to record the number of fits experienced by the child on the same diary. Both the PPP and diaries were completed by carers at baseline, 10 weeks and 6 months after allocation. At 10 weeks and 6 months after allocation, parents were asked to make a simple global assessment of whether they rated their children's overall health and wellbeing as the ‘same’, ‘better’ or ‘worse’ than when they entered the study and the same overall assessment of children's sleeping. For the purposes of the statistical analyses, the Global Health outcomes were categorised as ‘better’ versus ‘same’ or ‘worse’. Quality of life of the primary carer was assessed by completion of the SF-3615 at baseline, 10 weeks and 6 months. Table 1 gives full details of the outcome measures.
Outcome measures
Analyses
All children were analysed in the group to which they were randomised, irrespective of compliance. In the primary analyses, for continuous variables, the mean difference between groups and 95% CIs were calculated. For the few categorical outcome variables (CHQ-FC, global general health, global sleeping), odds ratios (ORs) and 95% CIs were calculated for the main category of interest. The CHQ-FC subscale is a five-point ordinal scale; for both the unadjusted and adjusted analyses CHQ-FC categories 0 and 30 the lowest categories were combined, because of small numbers in each of these categories.
Secondary analyses were carried out to examine the differences between groups after adjustment for potential explanatory variables and baseline values for those outcomes where these were measured. For the continuous outcome variables, a general linear modelling procedure was used to estimate the differences, and corresponding 95% CI. The explanatory variables adjusted for were age, sex, centre, social class, ethnicity, GMFCS category (as a proxy for the GMFM) and parents' beliefs about cranial osteopathy at baseline. Social class was based on the mother's current or most recent occupation and classified as 1, 2 or 3/4, using the Office for National Statistics classification system.22 The child's ethnicity was self-categorised by parents from a defined list and collapsed into three ethnic groups, black, white and other. If the outcome under consideration had been measured at baseline, this was also included within the modelling procedure as a covariate. A similar approach was utilised for the categorical outcome variables, based on either binary or ordinal logistic regression. For these outcomes, the OR (and 95% CI) for the groups was calculated, after adjustment for all explanatory variables.
The fit of each of the linear models and assumptions underlying each model were checked visually. For observations that apparently did not fit well with the derived model, these data points were identified and the analysis repeated with these observations removed. Removing such observations had minimal effects on the statistical models. Therefore, the models presented are based on the maximum data available for each outcome.
Results
Enrolment, follow-up and compliance
One hundred and ninety-three families were referred to, or made contact with, the research team, of whom 51 either did not meet the inclusion criteria or declined to participate; 142 children were randomly assigned to either intervention or control (figure 1). Therefore the total number is eight children fewer than originally planned but the decision to cease recruitment was made on the basis of very low withdrawal rates.

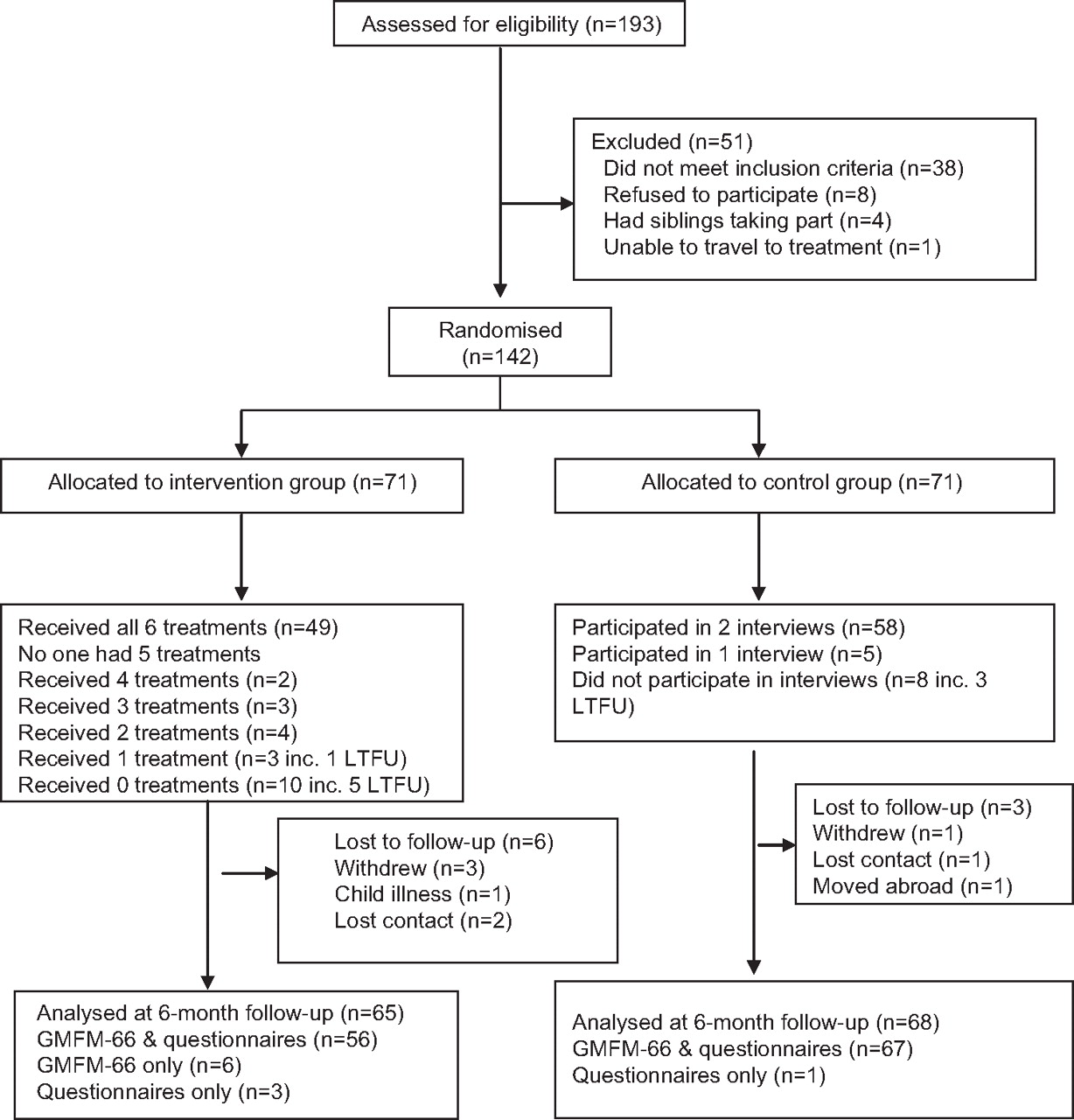{kind=link}
CONSORT flowchart.
Baseline characteristics were similar for both groups, although a higher proportion of children in the control group had communication difficulties (table 2). There were broadly similar categories of CP for both groups (table 2).
Characteristics of trial participants at baseline: number (%)*
Of the nine (6%) children lost to follow-up, four withdrew from the study, one child moved abroad, one became ill and the study team lost contact with three families. One hundred and twenty-nine (91%) children were assessed for the primary outcomes (GMFM-66 and CHQ) at 6 months. Figure 1 shows the follow-up rates for the other outcome measures.
Forty-nine of the 71 children (69%) assigned to the intervention arm had all six sessions of cranial osteopathy, 22 children had four or fewer sessions, and 10 children did not have any sessions. Five of these 10 children withdrew from the study, and the practicalities of taking up the sessions proved insurmountable for the other five children, all of whom had a final assessment (figure 1).
The average length of treatment sessions was 21 min. Osteopaths reported that in these sessions they most commonly used cranial osteopathic techniques in the head, pelvic and thoracic regions but also that they used other techniques, such as joint manipulation and deep tissue massage, in some children where they believed these were indicated.
Six-month assessments
Primary outcome measures
There was no evidence to support statistically significant differences between groups on either of the primary outcome measures, gross motor function or child's quality of life. The mean GMFM-6617 score for children in the intervention group was 4.9 points higher than for those allocated to the control group (95% CI −4.4 to 14.1) and a mean of 2.2 points (95% CI −3.5 to 8.0) and 3.4 points (95% CI −0.8 to 7.7) higher for the CHQ13 Physical Summary Score and Psychological Summary Score, respectively (table 3). The cumulative OR (which estimates the likelihood of a child in the intervention group being in a higher, more advantageous category) for the CHQ Family Cohesion scale was 0.75 (CI 0.39 to 1.43).
Unadjusted outcome measures at 6 months: motor function, child's quality of life, main carer's quality of life, sleep, pain and global measures
Blinding of the GMFM-6617 was maintained in 127 of 129 (98%) assessments. Sixteen (12%) assessments of the GMFM-6617 were double scored to estimate the limits of agreement23 between two of the raters: 95% of the differences between raters were between −1.9% and 2.6%, indicating a high level of agreement.
Secondary outcome measures
No statistically significant differences between groups were found on time to sleep, time spent asleep, parental assessment of child's pain or main carer's quality of life. Parents of 23% of children in the intervention group rated their child's sleep as ‘better’ at 6 months compared with 21% of those in the control group (OR 1.12, 95% CI 0.43 to 2.87). Thirty-eight per cent of parents of children in the intervention group rated their child's global health as ‘better’ than at enrolment compared with 18% in the control group (OR 2.75, 95% CI 1.13 to 6.87).
Adjustment for potential explanatory variables did not materially affect the results of any of these analyses (table 4). The adjusted OR for carers rating their child's global health as ‘better’ rather than the ‘same’ or ‘worse’ was 3.77 (95% CI 1.48 to 9.62) and for rating their child's sleep as ‘better’ was 1.21 (95% CI 0.49 to 2.98). The adjusted OR for the CHQ Family Cohesion scale was 0.84 (CI 0.40 to 1.76).
Adjusted outcome measures at 6 months: motor function, child's quality of life, main carer's quality of life, sleep, pain and global measures*
Ten-week assessments
Follow-up data at 10 weeks were not so easy to obtain, possibly because these were collected by self-return postal questionnaires, with complete outcome data available for only 61% of children. For continuous variables, results of the unadjusted analyses are shown in table 5. Statistically significant differences were found favouring the intervention group in one of four subscales of the CHQ,13 in the Mental Component Score but not the Physical Component Score of the SF-36,15 and in mean time to sleep but not mean time asleep (table 5). The cumulative OR for the likelihood of a child in the intervention group being in a higher, more advantageous category on the CHQ Family Cohesion scale was 0.74 (CI 0.35 to 1.56). Compared with children in the waiting list group, a greater proportion of parents with children in the intervention group rated their child as having better (compared with the ‘same’ or ‘worse’) general health (OR 15.00, 95% CI 3.04 to 140.90) and sleeping (OR 7.03, 95% CI 1.67 to 41.14).
Unadjusted outcome measures at 10 weeks: child's quality of life, main carer's quality of life, sleep and global measures
Adjustment for potential explanatory variables did not materially affect the results (table 6). The adjusted OR for the CHQ Family Cohesion scale was 0.83 (CI 0.35 to 1.97). The adjusted ORs for parents rating their child's general health or sleeping as better in the adjusted models were 26.94 (95% CI 3.61 to 200.95) and 13.65 (95% CI 2.51 to 74.31) respectively.
Adjusted outcome measures at 10 weeks: child's quality of life, main carer's quality of life, sleep and global measures*
Side effects
No serious adverse events were reported and no child withdrew from the study due to side effects of the treatment.
Discussion
This trial provides little evidence that cranial osteopathy leads to sustained improvement in the health or quality of life of children aged 5–12 years with CP. At 6 months, neither the independent assessment of motor function (GMFM-66), nor carer completed measures of their child's or their own quality of life, sleep or pain, suggested any statistically significant difference between children who had a course of cranial osteopathic treatment and those assigned to a waiting list. Carers were asked whether their child's global health was better, the same or worse than at the start of the study. Twice as many carers of children in the intervention group as in the control group said they believed their child's global health was ‘better’ at the end of the study. This result has to be interpreted in the light of the fact that no attempt was made to mask carers to allocation but is an interesting reflection of carers' perceptions. Interestingly, adjustment for potentially important baseline variables, including the strength of carers' prior beliefs in the likelihood of positive effects of cranial osteopathy, did not materially affect the results for any outcome measure.
Statistically significant differences were found on some subscales of measures of quality of life of the children and carers, and on carers' global assessment of health and sleeping at 10 weeks, but unfortunately these results were based on only 61% of participants (55% of those in the intervention group), which seriously hinders interpretation. The intermediate assessments at 10 weeks were conducted as this was felt by the osteopaths to be approximately half way through the osteopathy treatment sessions and hence could detect any initial treatment effects.
Stakeholder involvement
The parental involvement in the design and choice of outcome measures for the study, the authors feel, contributed to the successful recruitment and retention of children in the study. While the use of a ‘placebo’ in the control group might have strengthened the authors' ability to make causal inferences, parents consulted were unanimous that this would effectively rule out high levels of recruitment. Out of the 193 children assessed for eligibility, only eight (4%) refused to participate and follow-up data at 6 months were collected for 133 of 142 (94%) of the children who entered the study.
Experienced paediatric osteopaths were consulted before carrying out the trial and an osteopath was included in the research team to ensure that outcomes were measured that they regarded as being likely to be amenable to change with therapy, and that the therapy children received during the trial would be directly comparable to that which they would normally provide for such children.
Limitations of the study
Some osteopaths have argued that their treatment is likely to be particularly effective in babies and younger children.9 This study included children aged 5–12 years and therefore the extent to which the results can be extrapolated to younger children or indeed to different intensities and frequencies of treatment is unclear. The choice of age range was guided by parents and was determined partly by the relative ease of identification of children within this age group as having CP and partly because the frequency of other interventions in most preschool children with CP is such as to preclude many parents from being able to commit to participation in trials.
The GMFM was not assessed at baseline (due to cost constraints) and therefore the GMFCS scores were used in the adjusted analyses as a proxy measure of the GMFM Although the GMFCS is a different scale, it measures the same underlying functional abilities and has been shown to be highly correlated with GMFM score.12
Comparisons with other studies
This is one of the largest randomised controlled trials of any intervention conducted with children with CP. The authors believe that the relative ease of recruitment and retention reflects the close involvement of parents at all stages in the process. The evaluation of the effectiveness of complementary therapies in this population may not be seen as a priority by some clinicians. However, this study was conducted at the request of a parent-run charity in response to their members' desire for evidence on which to base treatment choices. Families of children with CP sometimes feel their children's needs are not being sufficiently met by health and social care providers24 and parents may have different treatment priorities than healthcare providers.25 It has been reported that parents and carers of children with chronic conditions, including CP, are three times more likely to choose CAM than a typically developing population26 but there is a paucity of evidence regarding the effectiveness of these therapies in children with CP.
Conclusion
Children with CP frequently have lives complicated by being offered multiple appointments and interventions within the health service in addition to any complementary therapies parents or carers choose. The authors believe that the lack of statistically significant differences between intervention and control groups in this study, the first rigorously designed evaluation of the effectiveness of this widely used therapy in children with CP, substantially reduces the uncertainty about its possible effects. It is important that in helping parents and carers to decide which interventions to choose they have access to the best possible information about effectiveness for both mainstream and complementary therapies.
Acknowledgments
The authors thank the children and families involved in the OCP Trial, and the many healthcare professionals and special schools who passed trial information to families, and support groups and charities, including Cerebra, Scope, Hemihelp and Contact a Family who publicised the trial on their behalf. The authors also thank Osteopaths at the Foundation for Paediatric Osteopathy in London, St David's Osteopathic Clinic in Exeter, Bridgetown Dental and Osteopathic Clinic in Paignton and Bodyworks Therapies of Plymouth for administering the osteopathic treatment; Physiotherapists, Jenny Freeman, Pam Ebdon, Sue Joiner and Jo Pearson who carried out the GMFM assessments; Dr Paul Ewings and colleagues at Southwest Research Design Service, Taunton for the telephone randomisation service; Dr Jill Ellis for advice on recruitment and other aspects of trial conduct; Simon Mills for making initial contact with the osteopaths; Dr Chris Morris for comments on the manuscript; Laura Stabb for database design and maintenance and Hannah Parsons for website design. Other members of the OCP Trial team were Claire Lloyd, Camilla McHugh and Belinda Afford.
References
Footnotes
-
Funding The study was funded by Cerebra. The funder monitored the trial progress through a trial steering committee chaired by Professor Alan Emond. Trial data were monitored by a data monitoring committee subgroup chaired by Dr Paul Ewings. The funders had no part in the design of the study; the collection, analysis, and interpretation of the data; the writing of the report; and the decision to submit the article for publication. SL, NB, KW and VE were also partially supported by the National Institute for Health Research (NIHR) PenCLAHRC. The study sponsor was the Royal Devon and Exeter Hospital.
-
Competing interests None.
-
Ethical approval The study was approved by Southwest Research Ethics Committee (06/MRE06/1) in April 2007. The parents/legal guardians of all children enrolled gave their informed consent for their child to participate.
-
Provenance and peer review Not commissioned; externally peer reviewed.