Article Text

Abstract
Objective Clinical outcomes of HIV-infected children on antiretroviral treatment (ART) in a decentralised, nurse/counsellor-led programme.
Design Clinical cohort.
Setting KwaZulu-Natal, South Africa.
Patients HIV-infected children aged ≤15 years on ART, June 2004–2008.
Main outcome measures Survival according to baseline characteristics including age, WHO clinical stage, haemoglobin and CD4%, was assessed in Kaplan–Meier analyses. Hazard ratios for mortality were estimated using Cox proportional hazards regression and changes in laboratory parameters and weight-for-age z scores after 6–12 months' treatment were calculated.
Results 477 HIV-infected children began ART at a median age of 74 months (range 4–180), median CD4 count (CD4%) of 433 cells/mm3 (17%) and median HIV viral load of log 4.2 copies/ml; 105 (22%) were on treatment for tuberculosis and 317 (76.6%) were WHO stage 3/4. There were significant increases after ART initiation in CD4% (17% vs 22%; p<0.001), haemoglobin (9.9 vs 11.7 g/l; p≤0.001) and albumin (30 vs 36 g/l; p≤0.001). 32 (6.7%) children died over 732 child-years of follow-up (43.7 deaths/1000 child-years; 95% CI 32.7 to 58.2), 17 (53.1%) within 90 days of treatment initiation; median age of death was 84 (IQR 10–181) months. Children with baseline haemoglobin ≤8 g/l were more likely to die (adjusted HR 4.5; 95% CI 1.6 to 12.3), as were those aged <18 months compared with >60 months (adjusted HR 3.2; 95% CI 1.2 to 9.1).
Conclusions Good clinical outcomes in HIV-infected children on ART are possible in a rural, decentralised service. Few young children are on ART, highlighting the urgent need to identify HIV-exposed infants.
This paper is freely available online under the BMJ Journals unlocked scheme, see http://adc.bmj.com/info/unlocked.dtl
Statistics from Altmetric.com
Introduction
The mortality and morbidity of HIV-infected children in developed countries has improved considerably with antiretroviral treatment (ART).1 Children in developing countries show similar improvements in health and survival when given ART, despite a restricted choice of drug regimens.2,–,5 However, the proportion of children with access to ART remains unacceptably low.6 7 Of the estimated 780 000 children under 15 years of age eligible for ART globally, only 10% were receiving treatment by the end of 2007, and subsequent progress has been painfully slow.7 Further, early treatment of infants with ART results in substantially improved survival.8 9 This in turn relies critically on early diagnosis of HIV-exposed infants and appropriate referral from well-functioning prevention of mother-to-child transmission (PMTCT) programmes.6 7 10
What is already known on this topic
▶ There has been rapid scale-up of HIV treatment programmes in Africa, home to most HIV-infected children globally.
▶ HIV-infected children in developing countries given antiretroviral therapy (ART) show similar improvements in health and survival to children in the developed world, although experience with paediatric ART in resource-limited settings is limited.
What this study adds
▶ Good clinical and virological outcomes of children on ART are possible in a decentralised, nurse/counsellor-led programme, in a rural resource-limited setting.
Problems in providing wide-scale ART in sub-Saharan Africa, particularly in rural areas, include lack of health personnel, difficulties with transport and delivery of drugs to health facilities, lack of diagnostic facilities, and limited and costly paediatric drug formulations compounded by the production of syrups requiring refrigeration rather than difficult-to-dose tablets, and no affordable fixed-dose paediatric drug combinations.4 11,–,14 Evaluation of the few existing programmes is hindered by a lack of functioning monitoring systems to quantify deaths and attrition due to loss to follow-up, which may be substantial.15
We add to the knowledge base by reporting on the clinical and virological outcomes of children on ART in a decentralised, nurse- and counsellor-led programme in rural South Africa.
Methods
The setting
Hlabisa sub-district, situated in rural northern KwaZulu-Natal, covers 3729 km2, with a population of approximately 220 000. KwaZulu-Natal has one of the highest HIV burdens in the world, with a peak prevalence of 27% in females aged 15–49, and 13.5% in males aged 15–54,13 and a prevalence of around 38% among pregnant women.16 Unemployment is high and families with no income rely on social grants.17
Healthcare
The health infrastructure is typical of many other rural health districts in South Africa, consisting of 16 primary healthcare clinics, two mobile clinic facilities and one 296-bed district hospital. Nurses run the busy clinics, with 95% of pregnant women attending at least one antenatal clinic visit18 and up to 80% of children achieving full primary vaccination.19 Individuals travel an average of 4.72 km to their nearest clinic, with a maximum distance of 13.2 km.20
Hlabisa HIV treatment and care programme
The Hlabisa HIV treatment and care programme, which first started treating patients in June 2004, is a partnership between the Department of Health (DoH) and the Africa Centre for Health and Population Studies (www.africacentre.ac.za), with additional funding provided by PEPFAR. The service is decentralised; patients access free care at their nearest primary healthcare clinic, where nurses and counsellors (lay staff who receive standardised training on issues including HIV counselling and testing, HIV treatment and adherence, and drug side-effects) are based. Physicians visit all clinics to initiate ART and follow up on medical problems. A few patients start ART as in-patients in the local hospital. Access to private medical care is limited.21
Children enter the programme by a number of routes: through the DoH prevention of mother-to-child transmission (PMTCT) programme implemented in 2001, a tuberculosis (TB) programme where HIV testing of all patients is encouraged,22 testing and referral after illness, HIV testing if other family members are already on treatment, or transfer into the programme of children already on ART. Eligibility, using a combination of immunological and clinical criteria, is assessed using provincial DoH paediatric guidelines, first published in 200423 and revised in March 2008,24 in line with WHO guidelines,14 and reflecting evidence that early treatment in infants results in better clinical outcomes8 (table 1).
Clinical criteria for eligibility for antiretroviral therapy in children, KwaZulu-Natal, South Africa24
Children undergo clinical staging, are screened for pulmonary tuberculosis (based on history, examination and chest x-ray), which is highly prevalent in the area,25 and opportunistic infections are treated. Baseline blood samples are taken (CD4, viral load, full blood count, creatinine and liver function tests); samples for viral load measurement are sent to the referral hospital 75 km away, while all other tests are carried out at the local hospital. Children eligible for treatment have a named caregiver who undergoes three educational training sessions, conducted by HIV counsellors, before treatment is started. Children are followed up by nurses and counsellors at monthly visits, with physician appointments when clinically indicated. Laboratory parameters are repeated 6-monthly, including full blood count, liver function tests, CD4 counts and viral loads.
DoH drug regimens24 are followed, with first-line treatment consisting of two nucleoside reverse transcriptase inhibitors (stavudine and lamivudine) plus one non-nucleoside reverse transcriptase inhibitor (efavirenz) for those aged over 3 years, or a protease inhibitor (lopinavir/ritonavir) for those aged under 3 years. Second-line treatment includes zidovudine, didanosine and either nevirapine or efavirenz for children aged less than 3 years, and lopinavir/ritonavir for those over 3 years. The programme does not have access to resistance testing.
Medicine is collected monthly; children failing to collect medicine at scheduled visits are considered to have defaulted treatment and attempts are made to trace the patient by phone or home visit by a nurse tracker. Children who have not collected their medicine for 3 months, despite attempts to trace them, and who are not known to have died or transferred out of the programme, are regarded as lost to follow-up from the last known contact date at the clinic.
A home-based care programme, consisting of three nurses and 470 community volunteers, trained in first aid, nutrition and ART adherence, provide additional care, at home, for children requiring extra support.
Data management
Patient data are stored in paper-based records at clinics. The baseline data of all children initiated on ART, and limited clinic follow-up details, were collected from the clinics monthly by a monitoring and evaluation team, and entered into a secure electronic database with restricted access (C Newell, personal communication, May 2009).
Statistical analysis
Eligibility criteria for inclusion in the analyses included all those aged ≤15 years who were started on ART by the end of June 2008; this cut-off date was chosen to allow at least 6 months of follow-up on ART for all children. Continuous variables were compared using t tests, and categorical variables using Pearson's χ2 tests. Survival by baseline characteristics including age, WHO clinical stage, haemoglobin and CD4%, was assessed in Kaplan–Meier analyses.26 Hazard ratios (HR) for mortality were estimated using Cox proportional hazards regression.27 Weights were plotted against US Centers for Disease Control and Prevention charts,28 using Epi Info 2000 to determine weight-for-age z scores (WAZ). CDC charts were used in preference to the WHO reference 2007 package29 because the latter computed WAZ scores up to age 10 years only, while the former goes up to age 20 years, which included our age limit (<16 years).
We calculated the mortality and lost to follow-up rates of children on ART, before and after 90 days of therapy, with exact 95% confidence limits; time periods were in line with previously published reports.2 30 Reported overall mortality considers active patients only, and excludes children who are lost to follow-up from the programme. However, upper mortality estimates are also presented assuming all children with advanced disease (WHO clinical stage 3 or 4) who were lost to follow-up have died, and also, separately, that all children lost to follow-up have died. For the mortality and attrition analyses, we generated a proportional hazards model for all children because our numbers were too small to allow stratification by different age groups. Factors in the univariate analysis found to be significant at p<0.05 were included in the multivariable proportional hazards regression model.
We dichotomised haemoglobin concentration at <8.0 g/l or ≥8.0 g/l, albumin at ≤27 g/l or >27 g/l, WAZ at >−1, >−2 to −1, and <−2, WHO staging at 1 and 2, or 3 and 4, and CD4% at ≥20, 10 to <20, and <10. All analyses were performed in Stata (v 9.2; Stata Corporation, College Station, Texas, USA).
Ethics
Individual informed written consent was obtained from all participants in the programme to allow use of anonymised routine clinical data for research. Ethics approval was obtained from the Biomedical Research Ethics Committee of the University of KwaZulu-Natal and Research Office of the KwaZulu-Natal DoH.
Results
Between 1 June 2004 and 30 June 2008, 477 HIV-1 infected children were on ART; 68 of these (14.3%) transferred into the programme already on treatment. By 1 July 2008, 415 children (87%) were alive and active in the programme, 12 (2.5%) had transferred out of the programme and 50 (10.5%) had either died or were reported lost to follow-up (32 (6.7%) died, 18 (3.8%) were lost to follow-up).
Cohort characteristics at initiation
Children were relatively old at treatment initiation (median age 74 months) and only 58 (12.2%) children were <18 months of age (table 2A). The majority were in late stage clinical disease, almost half were under-nourished with a weight-for-age (WAZ) of less than −2 z scores, and a quarter had tuberculosis at initiation.
Characteristics of children prior to antiretroviral therapy, rural KwaZulu-Natal (June 2004–June 2008)
Virological and immunological responses to treatment (table 2B)
Laboratory markers of children 12 months after initiation of antiretroviral therapy, rural KwaZulu-Natal (June 2004–June 2008)
Overall, 447 (94%) children were still active in the programme after at least 6 months of treatment. In 310 (65%) children with a CD4% result available at 6–12 months after treatment initiation, the median CD4% increased by 29% of the original, from 17% pre-initiation to 22% 6–12 months post-initiation (p<0.001). Similarly, a substantial increase in absolute CD4 count of 20% was seen among the 315 (66%) children with a result, from 433 cells/µl pre-initiation to 519 cells/µl at 6–12 months post-initiation. Haemoglobin and albumin values significantly increased from 9.9 to 11.7 g/l (p≤0.001) and from 30 to 36 g/l (p≤0.001), respectively (table 2B). In the less than half of the cohort (n=184) for whom this information was available, median viral load at initiation was 153 006 copies/ml; 142 (73.5%) of 193 children who had a viral load after 6–12 months of treatment showed viral load suppression (<25 copies/ml).
Survival outcomes
Of 477 children, 32 (6.7%) died over 732 child-years of follow-up (table 3A). Children died at a median age of 84 (interquartile range (IQR) 10 to 181) months, and compared to those who survived, had a lower median WAZ score (–2.8 (IQR –8.0 to –1.0) vs 1.3 (–7.7 to –1.0); p=0.026) and lower baseline haemoglobin (8.6 (IQR 5.4 to 11.3) g/l vs 10.0 (4.1 to 24.4) g/l; p=0.007), were more likely to be WHO clinical stage 3 or 4 (92% vs 74%; p=0.040) and had greater immunosuppression (CD4% 9% (IQR 2% to 23%) vs 18% (IQR 1% to 58%); p<0.001).
Mortality in children receiving antiretroviral therapy, rural KwaZulu-Natal (June 2004–June 2008)
Most deaths occurred soon after treatment initiation; of the 32 children who died, 17 (53.1%) died within 90 days of starting ART, while the other15 died after the first 3 months. Similar trends were observed across all age groups (table 3A).
Differences in mortality, which persisted for years, were observed by haemoglobin levels, age, WHO clinical stage and CD4% at initiation (figure 1). Allowing for sex, WAZ, CD4%, haemoglobin, albumin, WHO stage, tuberculosis at initiation and age, the risk of dying was significantly increased with a haemoglobin <8 and age <18 months. Risk was also higher for malnourished (WAZ ≤–2) and immunosuppressed (CD4% <10) children, increasing with successively lower WAZ and lower CD4%, but this did not reach statistical significance (table 4; figure 1).
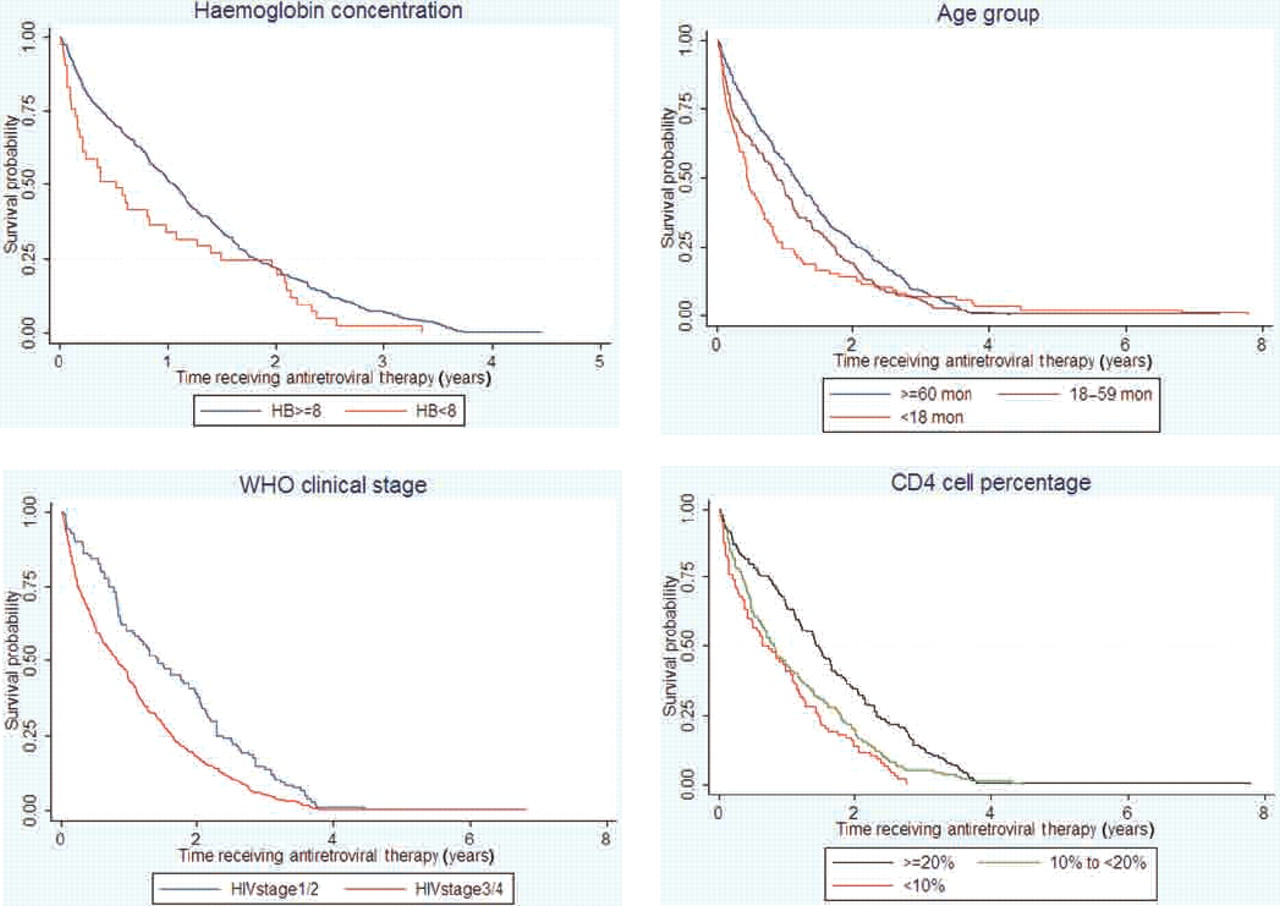
{kind=link}
Mortality in children receiving antiretroviral therapy by (A) haemoglobin concentration, (B) age, (C) WHO clinical stage and (D) CD4 cell percentage.
Factors associated with mortality in children receiving antiretroviral therapy
Loss to follow-up
Of 477 children started on ART, 18 (3.8%) were lost to follow-up (24.6 per 1000 child-years; table 3B). No significant differences in attrition were observed in the first 3 months of treatment compared to later in therapy. Multivariably, allowing for the same factors in table 4, the hazard of loss to follow-up was associated with HIV stage and CD4%: compared with children in clinical stage 1/2, those in stage 3/4 were more likely to be lost to follow-up (adjusted HR 1.40; 95% CI 1.08 to 1.83; p=0.030); compared to children with a CD4% >20%, those with a depleted CD4% were more likely to be lost to follow-up (adjusted HR 1.64; 95% CI 1.17 to 23.1) (data not shown).
Attrition in children receiving antiretroviral therapy in rural KwaZulu-Natal (June 2004–June 2008)
Children with more advanced disease (WHO clinical stage 3/4) had a threefold increased risk of mortality (table 4). Assuming that all children with advanced disease who were lost to follow-up had died, the upper mortality estimate in this rural cohort would have been 60.1 (rather than 43.7) per 1000 child-years; while assuming that all those lost to follow-up had died, the upper mortality estimate would have been 68.3 per 1000 child-years.
Discussion
We report good clinical outcomes and low levels of loss to follow-up in an HIV treatment and care programme in rural South Africa, adding to the emerging literature on ART in children in developing countries. A unique feature of this cohort is the decentralised model of care. The mean distance travelled by any individual in the population to their nearest clinic is 4.72 km (maximum 13.2 km)20 with a median travel time of 81 min.31 Travel time to the local hospital is double this (170 min),31 which is more costly to the patient and a potential barrier to regular clinical follow-up,32 in addition to overburdening the referral centre.
With the scale-up of ART programmes in sub-Saharan Africa, the issue of sustainability of rapidly expanding programmes is of concern.33 Task shifting, with a move away from physician-led diagnosis and management, has been discussed,34 but experience in paediatric ART programmes is limited. Although physicians initiate ART in our programme, follow-up is largely carried out by nurses and counsellors, thus providing information about clinical outcomes in a devolved service.
In line with other reports from sub-Saharan Africa,15 35 children were relatively old at treatment initiation, with only 58 (12.1%) children commencing treatment under the age of 18 months. PCR tests36 using dried blood spots for infants aged 6 weeks are the standard of care in South Africa, with in principle the possibility of HIV diagnosis by age 3 months. However, our results suggest the enormous problems in identifying infected infants, and highlight the urgency of strengthening PMTCT programmes to reduce the cumulative loss of individuals in the PMTCT cascade, from initial counselling of pregnant women to final diagnosis of infants who have ceased all breast feeding.37
Given the late presentation of children for treatment, it is not surprising that the majority were in WHO stage 3/4, a quarter already had tuberculosis, a third demonstrated moderate to severe malnutrition with a weight-for-age z score below −2, and median haemoglobin levels were low. Anaemia, a common complication of paediatric HIV infection, has previously been associated with disease progression and death.15 38 The aetiology is considered to be insufficient erythropoietin, and thus difficult to manage in resource-poor settings where available treatment consists of blood transfusions and iron supplements, for which there is limited evidence of efficacy.38 Severe anaemia (haemoglobin <8 g/l) was associated with an increased mortality risk in our cohort, and underlines the importance of earlier diagnosis while children are clinically well. The large proportion of children presenting with malnutrition and TB also illustrates the need for integration of HIV programmes with other care at primary healthcare level, as opposed to the numerous vertical programmes frequently observed.21 22 In this service children receive integrated disease management, including for malnutrition and TB, with the same counsellors providing adherence support for ART and TB medication. In an attempt to improve services further, a family-based clinic operating once weekly has been established at the busiest primary healthcare centre.
Our best estimate mortality of 43.7 deaths per 1000 child-years compares well with other cohorts from sub-Saharan Africa, including a large Zambian cohort2 with a mortality of 66 deaths per 1000 child-years, which is similar to our upper mortality estimate, and a 2-year risk of death after ART initiation of 6.9% in the KIDS-ART LINC collaboration.15 The high mortality in the early months after treatment initiation, in line with other reports,2 15 39 illustrates the need for increased monitoring and early identification of clinical problems during this phase. Young children were at increased risk of death, again highlighting the need for early diagnosis before infants become clinically unwell, with a system allowing fast-tracking of those eligible for treatment.8
Surprisingly, we had extremely low rates of attrition, despite the decentralised model of care, rural location and high mobility of our population. This is contrary to findings from pooled data from 16 urban African sites, where attrition was high but mortality low.15 Each case lost to follow-up was thoroughly investigated to ascertain further details, in particular whether the child had died. Children who were immunologically depleted or with more advanced disease were more likely to be lost to follow-up. It is possible that some of the 18 children lost to follow-up might have died, thus increasing mortality but decreasing attrition rates, resulting in a very low attrition rate but mortality comparable with other African sites. We suggest that our low attrition rates are due to accessible services, a patient tracking system, an integrated package of care minimising time spent at clinics, and the assumption that some children with difficult social circumstances might not have entered the programme at all.
Emphasis has been placed on increasing numbers of children on treatment globally,21 35 however, with expansion of paediatric ART programmes the quality of, and retention in, care will become increasingly important. One of the weaknesses of our study is the large proportion (approximately one third) of children who do not have a viral load or CD4 count result 6–12 months after treatment initiation. However, of those with a result, three quarters showed viral suppression, similar to other reports,39 but the need for constant monitoring and vigilance remains as cohorts mature and issues of treatment failure arise.
There are many challenges to sustaining a rapidly expanding programme such as this. Priorities for the future include increasing numbers of infants on treatment, improving the proportion of children with documented laboratory results, maintaining low rates of loss to follow-up, and identifying and tracing children with unsuppressed viral loads in a timely manner. Decentralised programmes depend on the dedication of clinic-based staff, who deserve encouragement, regular clinical updates and feedback about the successes, not only the difficulties, of the programme.
Acknowledgments
We thank all children whose data are included in this study, our colleagues within the Department of Health and the Africa Centre for Health and Population Studies who contributed to the data collection and entry, and Colin Newell for data management.
References
Footnotes
-
Patient consent Parental consent obtained.
-
Competing interests None.
-
Funding The Africa Centre is funded by the Wellcome Trust (grant #050534), and the Hlabisa HIV treatment and care programme receives support through the United States Agency for International Development (USAID) and the President's Emergency Plan for AIDS Relief (PEPFAR) under the terms of Award no. 674-A-00-08-00001-00.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Ethics approval This study was conducted with the approval of the Biomedical Research Ethics Committee of the University of KwaZulu-Natal, South Africa and the Research Office of the KwaZulu-Natal Department of Health.