Article Text

Statistics from Altmetric.com
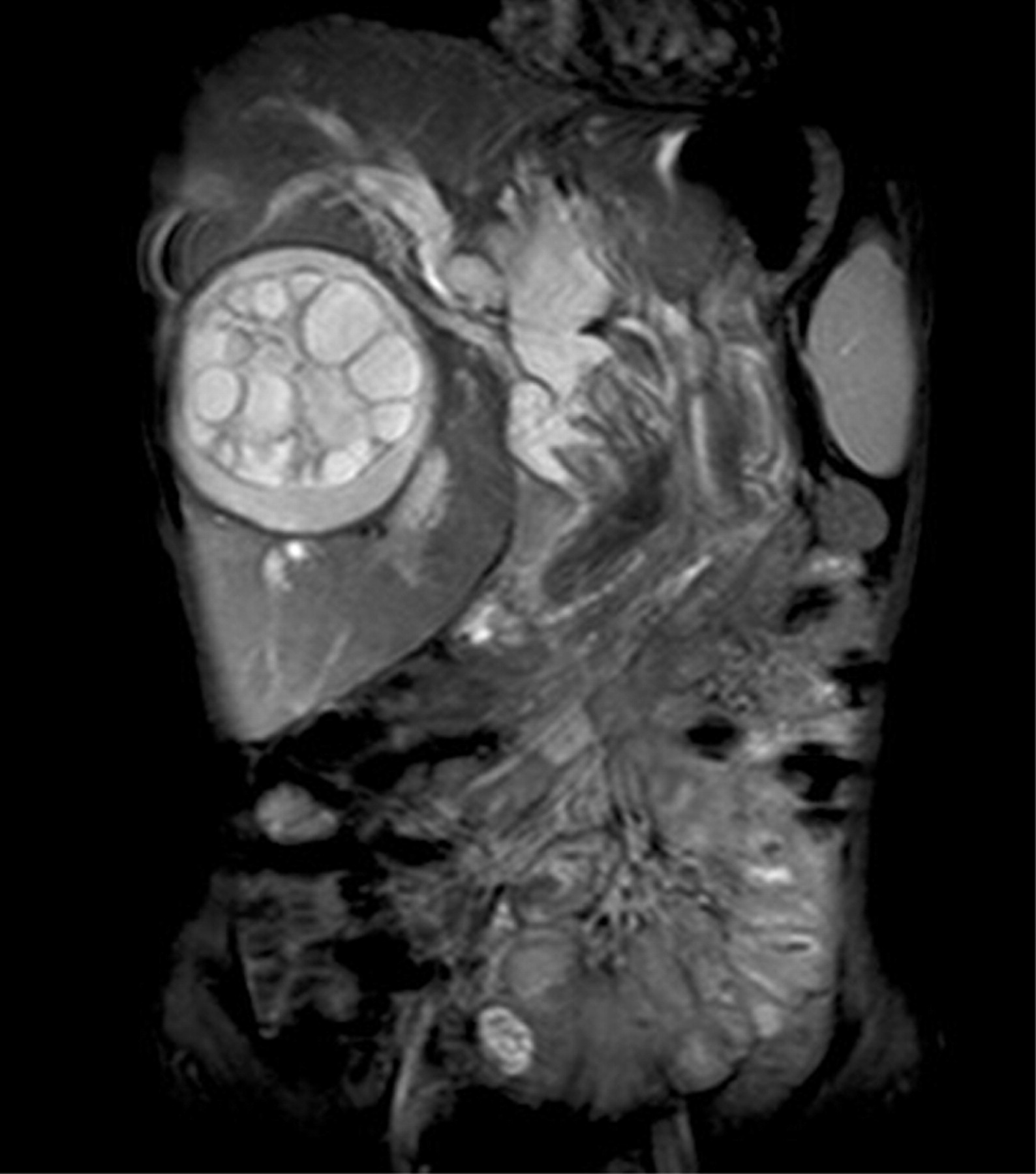
A 13-year-old girl presented with right hypochondriac pain associated with fever, rigors and chills. Physical examination was remarkable for mild icterus, pyrexia (high grade) and tender hepatomegaly. Laboratory investigations revealed leucocytosis with neutrophilia, elevated serum bilirubin levels, mild elevation of transaminase levels and marked elevation of alkaline phosphatase. Ultrasound examination of the abdomen revealed a large cyst in the right lobe of the liver with multiple peripheral daughter cysts, with a smaller left lobe cyst. Intrahepatic biliary radicals were grossly dilated with debris and few membrane fragments in the common hepatic duct; common bile duct (CBD) was not optimally visualised. As such, magnetic resonance imaging with magnetic resonance cholangiopancreatography of the patient was performed. A large hydatid cyst was seen in right lobe of the liver with multiple peripheral daughter cysts and a smaller cyst in left lobe of the liver. The intrahepatic biliary radicals were dilated with gross distention of the gall bladder. Multiple linear hypointense membranes were seen in the intrahepatic biliary radicals (IHBR), common hepatic duct (CHD) and most prominently in dilated CBD. The pancreatic duct was not dilated. The visualisation of cystic membranes in the CBD and CHD was more obvious on the heavily T2 weighted source half acquisition single shot turbo spin echo (HASTE) images, and less obvious on the maximum intensity projection (MIP) images.
Endoscopic retrograde cholangiopancreatography was subsequently performed, with retrieval of multiple membranes from the CBD.


{kind=link}
{kind=link}
{kind=link}
DISCUSSION
Ultrasound is the most frequent technique employed in the diagnosis of hepatic hydatid cysts. The various appearances by ultrasound include a unilocular cyst, a cyst with daughter cysts producing a multiseptate or a cartwheel appearance and a multivesicular cyst with heterogenous echogenic interior.1 A ruptured cyst may show undulating membranes inside. The sensitivity of ultrasound for diagnosis of intrabiliary rupture is 66–94%,2 and the accuracy is increased if CT is also employed.3 4 Contrast enhanced computed tomography reveals hydatids as cysts with wall enhancement as well as enhancement of internal septae; calcification is also easily demonstrated.5 6 Rupture into the biliary channels is suggested by dilation of CBD with low attenuation material inside. Cyst-wall discontinuity, a direct sign of rupture, is seen in three our of four cases.3 The accuracy of CT and ultrasound together is 100% in cases with uncomplicated biliary rupture.7
ERCP not only has a definitive diagnostic role but also has a therapeutic one. The membranes protrude out from the papilla of vater; dilated ducts with debris and daughter cysts appear as radiolucent filling defects.1
Our case emphasises the usefulness of MRI in showing that the membranes in the biliary channels and CBD are a cardinal manifestation of intrabiliary rupture.