Article Text

Abstract
Objective General Medical Council (GMC) guidance describes an intimate examination as one that may be embarrassing for the patient, for example, breast or genitalia examination. Documentation of consent and use of a trained impartial observer (chaperone) is recommended. Pubertal staging is often necessitated for assessment of growth and puberty. We assessed current practice of pubertal staging by paediatricians and paediatric endocrinology nurse specialists (PENS) in the UK.
Methods An electronic survey was distributed to paediatricians (consultants and trainees) and PENS across the UK. The survey enquired about training received, confidence in and typical practice for pubertal staging examinations.
Results 235 responses were received. Low confidence in pubertal staging was commonly reported by trainees and consultants without an endocrinology interest.
Most respondents consider pubertal staging to be an intimate examination for male (94.9%) and female (93.1%) patients. Consent to examination is always documented by 38.2% of respondents. 62.0% and 54.8% report always using a chaperone for male and female pubertal staging, respectively. However, many respondents use a parent as the chaperone. Few document the name of the chaperone used. Patient objections and availability of chaperones were commonly perceived barriers to chaperone use.
Conclusion Most clinicians consider pubertal staging an intimate examination, but documentation of consent and use of formal chaperones is not standard practice. The use of a parent as a chaperone was common but is not recommended by the GMC. Local chaperone policies should address these issues to protect patients and clinicians.
- adolescent health
- endocrinology
- paediatrics
Data availability statement
Data are available upon reasonable request.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
The General Medical Council (GMC) published guidance on intimate examinations in 2013, which recommends the documentation of informed consent and the use of impartial chaperones familiar with the examination.
WHAT THIS STUDY ADDS
Most clinicians performing pubertal staging examination do consider it an intimate examination, but few document consent and many do not follow GMC guidance on chaperone use. Many clinicians consider a parent to be a suitable chaperone.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Education and local chaperone policies need to highlight the approach to pubertal staging examinations to include routine documentation of consent and use of appropriate chaperones.
Introduction
Puberty is a process that occurs over a period of 3–4 years and marks the physical transition from childhood to adulthood. It usually occurs in a sequence of predictable events, and progress through puberty is typically described using the Tanner staging in which stage 1 represents prepuberty and stage 5 a fully developed adult.1 2 A pubertal staging examination is a key assessment performed for the evaluation of linear growth, puberty and hormonal disorders and may involve examination of the breasts and genitalia. The examination necessitates palpation of the breast area to determine if breast buds are present (to distinguish from fat tissue) and assessment of testicular volumes by comparison to an orchidometer. Children and young people may find these examinations embarrassing, and it is important that an age-appropriate explanation is given to clarify the purpose of the examination and what it will involve such that they and/or their parent/caregiver can give informed consent.
The General Medical Council (GMC) in the UK defines an intimate examination as one that may be embarrassing or distressing to the patient and recommends documentation of consent and the use of a formal medical chaperone.3 The guidance is applicable to all ages. The role of a chaperone is as an impartial observer to provide support and protect the patient from potentially unnecessary and even abusive examinations, and to protect the health professional from false allegations. As such, a parent is not an appropriate chaperone for this examination but could also be present if desired by the patient.
A study of mostly female adolescents in Canada suggested that many would like to have a chaperone present for intimate examinations,4 but there is little data available on the typical use of chaperones for pubertal staging in paediatric practice. We undertook a survey of paediatricians and paediatric endocrinology nurse specialists (PENS) across the UK to establish confidence and training in pubertal staging, and typical practice in consent and chaperone use.
Methods
An electronic survey using Microsoft Forms was disseminated to paediatricians and PENS across the UK by specialist societies/groups (British Society for Paediatric Endocrinology and Diabetes clinical committee, the paediatric endocrinology and diabetes subspecialty training group, PENS group, Wessex Paediatric Endocrine Network), paediatric training schools (deaneries) and personal contact with paediatric endocrinologists. Respondents were asked to additionally disseminate the survey within their workplace to facilitate exposure to as many paediatricians and PENS as possible. Written informed consent to participation was obtained from all respondents and the survey completion was fully anonymous. Data were collected between 24 May and 1 July 2022.
The survey collected information on professional role, training received in pubertal staging, confidence in performing this examination and typical practice in consent and chaperone use for male and female pubertal staging examinations. Self-rated confidence in performing pubertal staging was reported on an integer scale from 0 to 10, with 0 being ‘not at all confident’ and 10 being ‘fully confident’. Respondents’ views on whether pubertal staging is an intimate examination and awareness of the GMC guidance on intimate examinations were also established.
Statistical analysis
Data analysis was performed using SPSS V.27. Confidence in pubertal staging was non-normally distributed and therefore summarised as median (IQR). Correlation with frequency of performing pubertal staging was assessed using Spearman’s rank. Categorical data were compared using χ2 test.
Results
A total of 235 responses were received from 212 paediatricians and 23 PENS; professional role is shown in more detail in table 1. Most respondents were women (74.9%). Responses were received from all training regions within the UK apart from Northern Ireland and Ireland; 31.5% of responses were from respondents working within the Wessex region; responses from other training regions varied between 1.4% and 14.5% of the total responses.
Demographics characteristics and confidence in pubertal staging of survey respondents by professional role
Awareness of GMC guidance on intimate examinations
77.9% of the survey respondents were aware of the GMC guidance on intimate examinations, but only 33.6% had read it. More consultants (44.1%) than trainees (23.1%) had read the guidance (p=0.001). Most respondents consider pubertal staging to be an intimate examination for men (94.9%) and women (93.1%).
Confidence in pubertal staging
The frequency of undertaking pubertal staging examinations varied markedly among respondents, with those in roles related to paediatric endocrinology undertaking these more frequently (table 1). Self-reported confidence in pubertal staging was low to medium in consultants who do not have a subspecialty interest in endocrinology and low in non-subspecialty trainees (table 1). Confidence in pubertal staging was associated with frequency of performing the examination with higher confidence in those who perform the examinations more frequently (male examination r=0.70, p<0.001, female examination r=0.77, p<0.001). Of the 49 respondents who had never performed a pubertal staging examination, 49.0% reported not feeling confident to perform the examination if clinically required.
97.4% of survey respondents had received some form of training in pubertal staging. The most common forms of training were self-directed reading of textbooks or online material (72.8%), observation of a colleague with experience in pubertal staging examination (58.3%) and lecture-based training (55.3%). Online training packages had been used by fewer respondents (1.7%).
Consent and chaperone use
Of the 186 respondents performing pubertal staging, consent to examination is always documented by 38.2% of respondents, usually/occasionally documented by 37.1% and never by 24.7%. More respondents who had read the GMC guidance always documented consent (54.5% vs 29.2%, p<0.001).
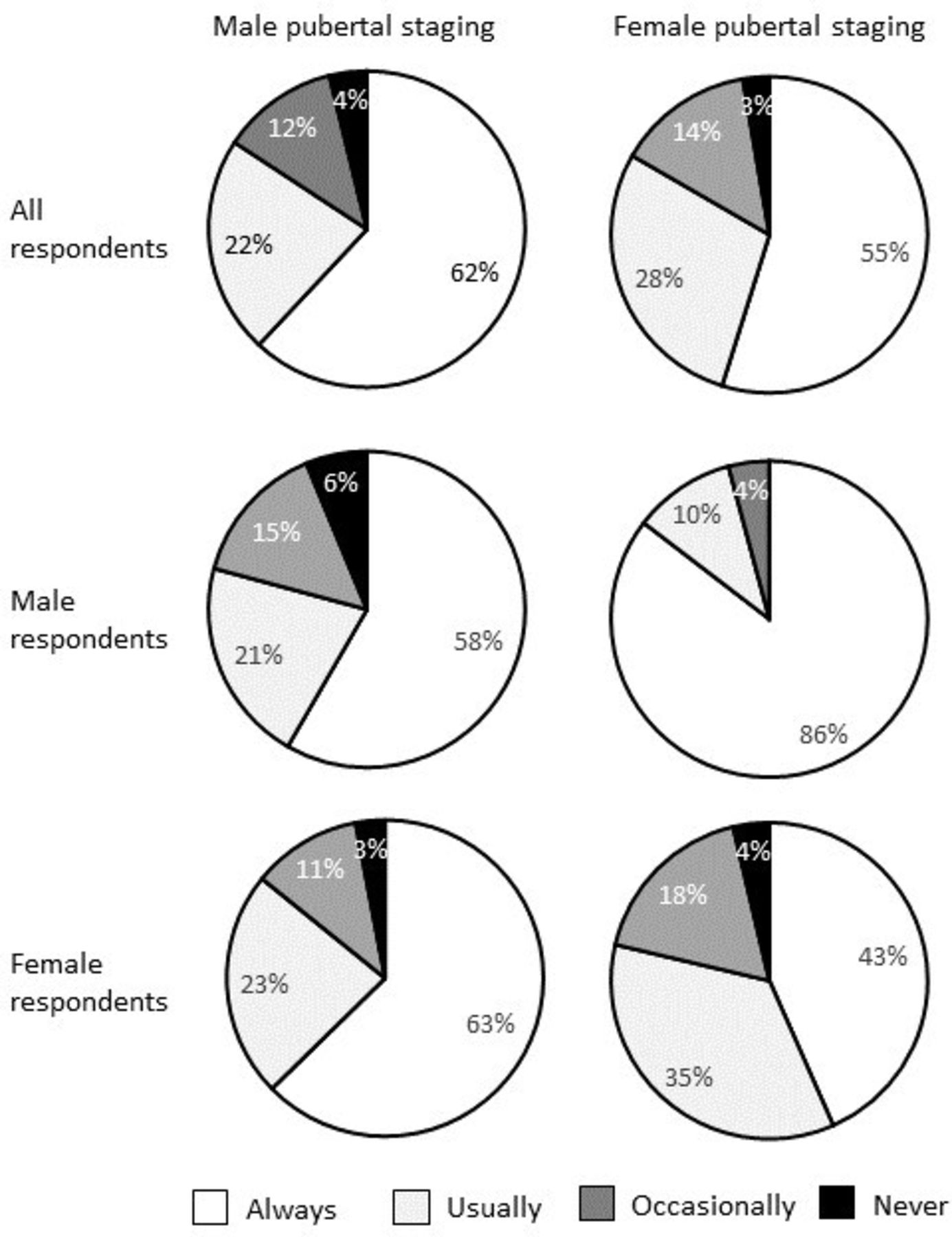
The use of chaperones for pubertal staging is shown in figure 1; 62.0% of respondents reported always using a chaperone for male pubertal staging, and 54.8% always use for female pubertal staging. Respondents are more likely to always use a chaperone when examining a patient of the opposite sex to themself (figure 1, male respondents p=0.003, female respondents p=0.002). Male respondents are more likely than females to always use a chaperone for female pubertal staging (85.4% vs 43.4%, p<0.001), whereas similar proportions of male (58.3%) and female (62.7%) respondents use a chaperone for male pubertal staging. Respondents who had read the GMC guidance were more likely than those who had not to always use a chaperone for female pubertal staging (66.7% vs 48.3%, p=0.016), but the proportion was similar for male pubertal staging (66.7% vs 59.3%, p=0.33).
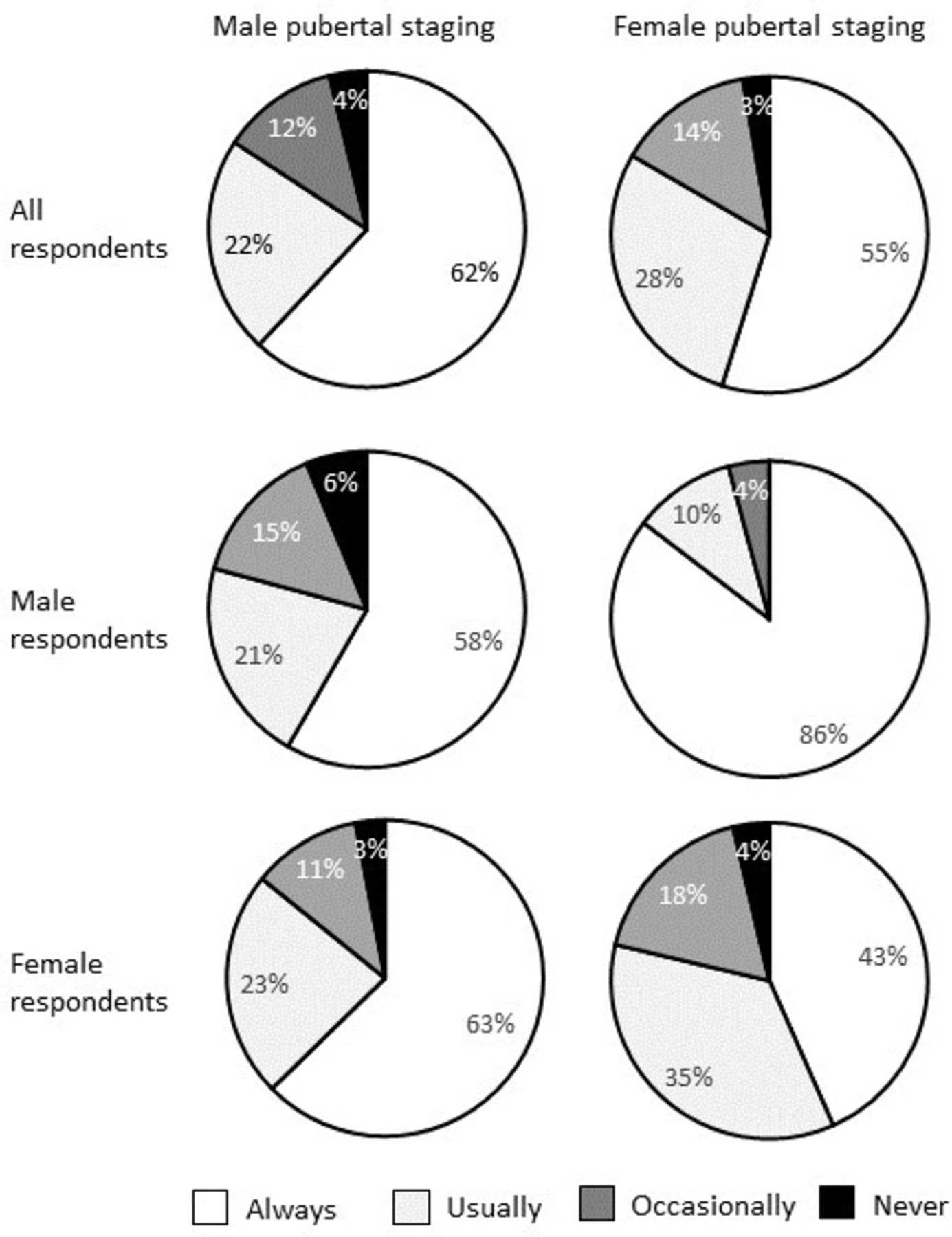
Reported use of chaperones for male and pubertal staging examinations shown for all respondents and by respondent sex.
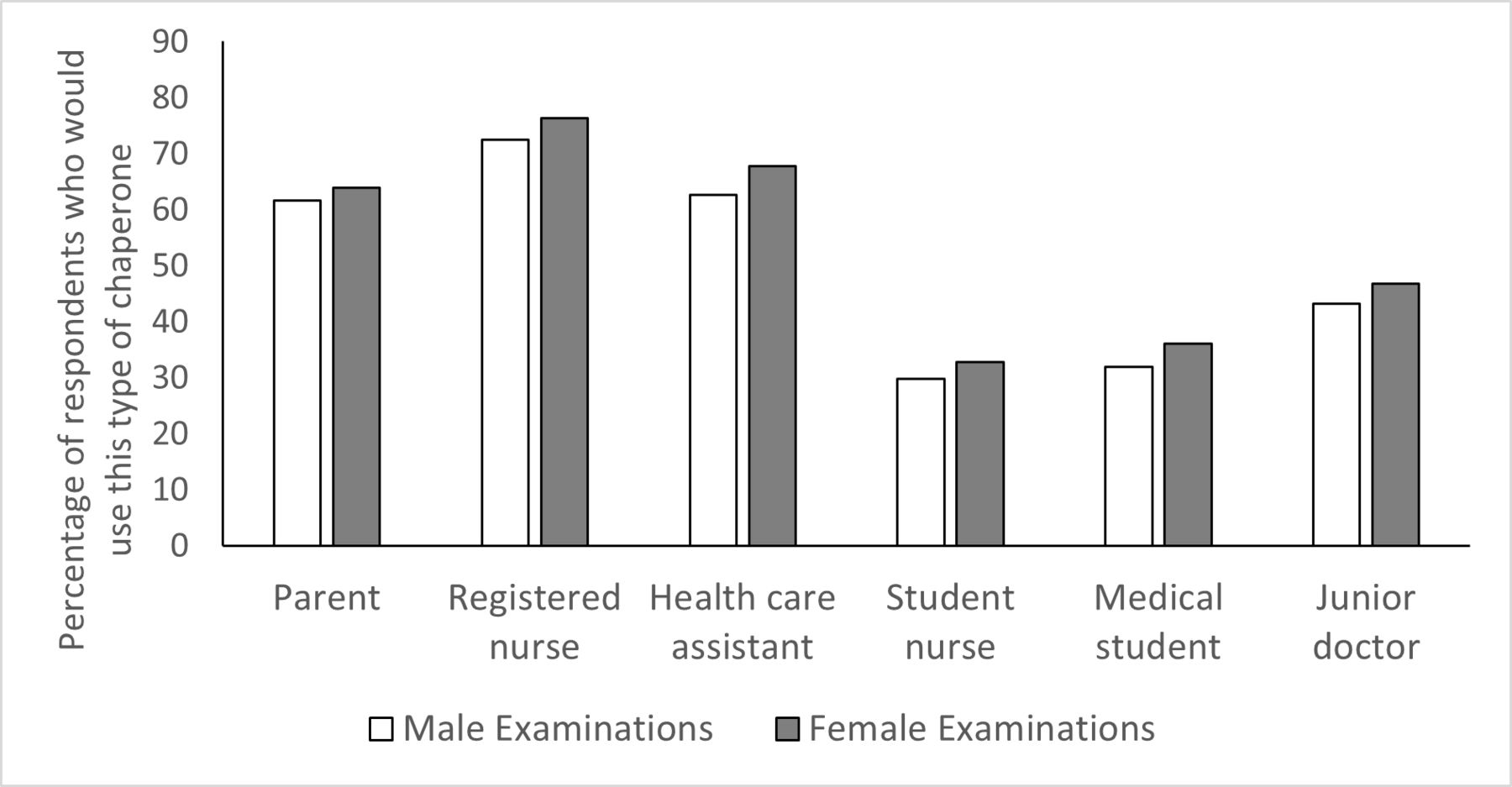
61.6% and 64.0% of respondents would use a parent as chaperone for male and female examinations, respectively (figure 2). Registered nurses were most asked to act as chaperones; 72.4% and 76.3% of respondents use registered nurses for male and female examinations, respectively. Fewer respondents reported using nursing students (male examination 29.7%, female examination 32.8%), medical students (male examination 31.9%, female examination 36.0%) or junior doctors (male examination 42.3%, female examination 46.8%) (figure 2). Perceived barriers to chaperone use are shown in figure 3. Only 29.4% and 32.2% of respondents always documented the name of the chaperone used for male and female pubertal staging, respectively.

Professional roles of chaperones used for male and female pubertal staging examinations. Respondents could select more than one response to this question.

{kind=link}
{kind=link}
{kind=link}
Perceived barriers to chaperone use for pubertal staging examinations by paediatricians and paediatric endocrinology nurse specialists. Respondents could chose more than one response.
Discussion
In this national survey of typical practice in pubertal staging examinations in the UK, only a third of children’s clinicians had read the GMC guidance on intimate examinations despite this having been first published in 2013.3 Most respondents would consider pubertal staging to be an intimate examination. Documentation of consent and use of an impartial formal chaperone, as recommended by the GMC, is not standard practice. Self-reported confidence in pubertal staging was reported to be low among paediatric trainees and consultants who do not have a specialist interest in endocrinology, yet assessment of growth and puberty is relevant to general paediatrics and paediatric specialties.
There are few previous data on the reported or documented use of chaperones for intimate examinations, and most published studies that we identified were in adult patients.5 6 Similar to our findings of reported chaperone use for pubertal staging, a survey of urologists found that 72.5% reported always using a chaperone for an intimate examination of the opposite sex, but much lower use for patients of the same sex.7 This was however much higher than the reported use of chaperones for intimate examinations by general practitioners (GP) in Australia8 and Canada,9 and in a study undertaken in 2006 in adolescent medicine and urology clinics that reported non-parent chaperones were used in very few consultations with adolescent patients (5%–18%).10
Many GPs in Australia, in similarity to respondents to our survey, perceived patient embarrassment/objection as a barrier to chaperone use.8 Studies in adult patients report marked variability in patient preference towards chaperone use,11–14 whereas there are few data in adolescents. A study conducted in 1986 in the USA suggested that few adolescents would want to have a chaperone present for pelvic examination15 and Feldman et al 10 found most (99.6%) adolescent patients and/or their families declined the offer of a chaperone, although no explanation for the role of the chaperone was given to the patients. More recent data from Canada showed that 61% of adolescents wanted the choice of a chaperone for an intimate examination, with only 29% reporting that they would not want a chaperone present at all.4 Qualitative studies report some patients feel more embarrassed by the presence of a chaperone, whereas for other patients a chaperone made them feel more at ease.4 11 Considering this, many of these studies advocate the importance of patient choice.16 However, patient choice fails to recognise the role of the chaperone in protecting both the patient from potentially abusive examinations and the doctor from false allegations. Both of these events are recognised to occur in paediatric clinical care,17 18 and abusive procedures have occurred in the presence of a parent, who had put their trust in the clinician.19 As such, while young people may prefer their parent to act as a chaperone,11 and many of our survey respondents felt a parent was an acceptable chaperone, an impartial chaperone is recommended by the GMC3 in addition to the parent. However, recognising patient preferences such as sex of the chaperone16 is important and should be considered in local chaperone policies. Availability of chaperones was also commonly cited as a barrier to chaperone use in our survey, and it is important that outpatient departments have sufficient staff to be able to support chaperoning in a timely manner. Nursing and medical students and healthcare assistants, as used as chaperones by many of our respondents, may not be fully able to fulfil this role if they are not familiar with the examination and/or do not feel confident to raise concerns about a doctor’s behaviour. Specific training should be offered to staff working clinically in outpatient departments to ensure they are comfortable in the role of a chaperone.
Confidence in pubertal staging was low among paediatricians in training and consultants not routinely working with paediatric endocrinology patients. As would be expected, confidence decreased with lower frequency of performing the examination. This may reflect that those clinicians with fewer opportunities to perform the examination are not able to increase their confidence through experience of undertaking examinations, but also that those who feel underconfident may avoid performing the examination and instead refer the patient to a more experienced colleague. Many trainee paediatricians in their final years of training reported never having performed a pubertal staging examination, highlighting the need for further training in this general paediatric skill. This training should encompass not only the physical examination findings but also the approach to this examination. We recommend highlighting the GMC guidance on intimate examinations and suggest the acronym ‘the 4 C’s’: documented informed Consent, use and documentation of a Chaperone, and patient Choices with Consequences. For the latter, the patient may, for example, be offered choices such as sex of the clinician performing the examination and chaperone, presence or absence of a parent and/or the choice to decline the examination. It is important that the patient understands the consequences of these choices, for example, delays to treatment or investigations if they wish to delay the examination until availability of a clinician of the opposite sex or entirely decline the examination.
There are limitations to this survey. In 2017, there were 8785 paediatricians in the UK,20 therefore 212 responses represent around 2%–3% of all paediatricians. Forty-three per cent of survey respondents have a paediatric endocrinology interest. The exact number of paediatricians with this interest in the UK was not reported in the most recent workforce census,20 but our sample is biased towards those working in this field and is therefore more representative of those frequently undertaking pubertal staging. As the survey was disseminated electronically by email and/or inclusion in a newsletter by several professional societies, networks and training groups, for which we did not have access to the distribution lists, the total distribution and thus overall response rate to the survey are not known. Paediatricians working in the Wessex region are over-represented, reflecting the area in which the researchers work. Our question regarding chaperone use was simply phrased as ‘How often would you use a chaperone?’. We did not define the nature of this chaperone, and therefore, as many clinicians subsequently reported using a parent as a chaperone, the proportion using an impartial medical chaperone is likely to be lower than reported here. Nonetheless, these findings further highlight the need to distinguish between the parent and an impartial chaperone to practising clinicians. The anonymous nature of the survey will have encouraged honest reporting, and indeed, inaccurate reporting would likely tend towards ideal rather than actual practice, yet our findings already highlight the need for additional documentation of consent and chaperone use.
In conclusion, we have demonstrated that documentation of consent and use of formal medical chaperones is not yet standard practice for pubertal staging. Few clinicians had read the GMC guidance that recommends these for intimate examination. Local chaperone policies should address these issues to protect patients and clinicians, and training of paediatricians should focus on the wider approach to pubertal staging including consent and chaperone use in addition to the examination findings.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by University of Southampton, Faculty of Medicine Research Ethics Committee (ERGO #72383). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We thank those who assisted with dissemination of this survey, including (but not limited to) the British Society for Paediatric Endocrinology and Diabetes (BSPED) Clinical Committee, the Wessex Paediatric Endocrinology Network, the trainee representatives for the Paediatric Endocrinology & Diabetes Trainees, and the UK paediatric training schools. We thank the doctors and nurses who completed the survey for their time.
References
Footnotes
Contributors RJM conceived the study, designed the methodology, acquired and analysed the data, interpreted the data, drafted and revised the manuscript. JHD designed the study, acquired the data, interpreted the data and revised the manuscript. Both authors approved the final submitted version of the manuscript. RJM is guarantor and accepts full responsibility for the work and/or the conduct of the study, had access to the data, and controlled the decision to publish.
Funding RJM is funded by an NIHR Academic Clinical Lectureship.
Competing interests JHD has received travel bursaries from Novo Nordisk, honoraria from Kyowa Kirin.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Highlights from this issue