Article Text

Abstract
Objective To examine the association between gestational age at birth and risk of clinically diagnosed intellectual disability (ID) week by week to provide a detailed description of ID risk across the entire range of gestational ages and by severity of ID.
Methods All individuals born alive in Sweden 1974–2017 were prospectively followed up from birth until 2017 using national registers. The HRs for ID according to weekly gestational age and gestational age categories were determined using Cox models. Sibling analyses were conducted to adjust for familial confounding.
Results The study included 3 572 845 live births. During the follow-up, 26 596 ID cases were registered. The adjusted weekly estimates showed a gradual increase in risk of ID from week 40 to week 24 (adjusted HR37weeks=1.80 (1.74 to 1.87), aHR32weeks=3.93 (3.73 to 4.13), aHR28weeks=7.53 (6.95 to 8.16), aHR24weeks=21.58 (18.62 to 25.00)) and from week 41 onwards (aHR42weeks=1.26 (1.19 to 1.32)), with statistically significantly higher risks across the range of gestational age compared with infants born at week 40. The associations were consistent in mild, moderate and severe/profound ID but most prominent for severe/profound ID.
Conclusion The risk of ID increased weekly as the date of delivery moved away from 40 weeks, both preterm and post-term. The results remained robust after detailed adjustment for confounding, including familial confounding.
- Epidemiology
- Child Psychiatry
Data availability statement
Data may be obtained from a third party and are not publicly available. Data cannot be shared publicly owing to restrictions by law. Data are available upon request to the Swedish registers (online via bestalladata.socialstyrelsen.se).
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
What is already known on this topic
Children born preterm have been associated with increased risk of intellectual disability. However, the risk across the entire gestational age has not been sufficiently studied.
What this study adds
We observed a weekly gradual increase in the risk of intellectual disability, as the delivery date moved away from week 40, both preterm and post-term.
How this study might affect research, practice or policy
Our study may help identify groups with elevated likelihood of intellectual disability, thus may allow for earlier detection of cases in the future.
Introduction
Intellectual disability (ID) is a generalised neurodevelopmental disorder characterised by significant restrictions in intellectual functioning and adaptive behaviour, including a range of everyday social and practical skills.1 ID affects approximately 1%–2% of the world’s population2 and is known to be clustered within families, suggesting a genetic or other shared familiar risk. Yet, clear biological mechanisms are not known, and risk factors can be divided based on the timing of exposure: prenatal, perinatal and postnatal.3
Children born preterm, as well as post-term, is known to be associated with an increased risk of ID.4–13 However, beyond categories ‘term’ or ‘preterm’, less is known about the development of ID risk across the entire spectrum of gestational weeks. To date, as we know, there is only one population-based study addressing this question,13 showing that the risk of ID was increased at non-optimal gestational duration and was highest in children born extremely preterm (<28 weeks) and in case of fetal growth restriction. Yet, risks stratified by sex and size for gestational age across the spectrum of gestational ages were not reported. Sex and size for gestational age are important, as ID has a male predominance14 and since size at birth is known to influence risks.15 So far, there are no population-based studies on gestational age-related risks of ID of different severity. Advancement of neonatal intensive care has improved survival of individuals born in the lowest gestational ages, but long-term neurological outcomes have not been sufficiently studied.
The aim of this study was to examine the association between gestational age at birth and risk of clinically diagnosed ID, week by week, to provide a detailed and robust description of ID risk across the entire range of gestational ages and by severity of ID.
Methods
Study population
A birth cohort of all children born alive in Sweden between 1 January 1974 and 31 December 2017 was established using data from Swedish national registers, including the Swedish Medical Birth Register (MBR),16 the Swedish Multi-generation Register,17 the National Patient Register (NPR),18 the Statistics Sweden Total Population Register19 and the Longitudinal Integrated Database for Health Insurance.20 Linkage was done through the personal identification number unique to every citizen. To reduce the potential genetic and cultural confounding and effect of changing immigration patterns, only individuals with parents born in the Nordic countries (Sweden, Denmark, Norway and Finland) were included. Individuals with missing information on gestational age, sex or with implausible death/emigration dates were excluded.
Exposure
Information on gestational age at birth was retrieved from the MBR and determined using ultrasound measurements early in the second trimester (routine practice since the mid-1990s) or the date of the last menstrual period.
Outcome
The primary outcome was the first clinical diagnosis of ID registered in the NPR, including hospitalisation and hospital-based outpatient specialist care. For the analysis on the severity of ID, we further subcategorised ID into mild, moderate, severe/profound according to the specific ICD (International Classification of Diseases) codes (online supplemental table S1).
Supplemental material
Covariates
We considered several factors that might confound or modify the association between gestational age and risk of ID. Birth year was categorised into 5-year intervals from 1974 to 2015 and from 2015 to 2017. Size for gestational age, according to sex-specific birth weight distributions per 5-year birth bracket, was categorised as small for gestational age (SGA; ≤10th percentile of population), appropriate for gestational age (AGA; 11–89th percentile population) and large for gestational age (LGA; ≥90th percentile of population).21 22 Maternal age and paternal age were categorised as <20, 5-year intervals from 20 to 39 and ≥40. Maternal smoking during pregnancy (yes/no)23 was recorded since 1983. Highest attained parental education at birth, available for births post-1990, was categorised as university education, upper secondary education and compulsory education or less (≤9 years of education). Parental history of ID and autism spectrum disorder (ASD) were retrieved through the NPR.
Statistical analysis
Incident rates of ID per 100 000 person-years was calculated. Each child was followed from birth and until first diagnosis of ID, death, emigration or 31 December 2017, whichever came first. The Inverse Kaplan-Meier curves for cumulative incidence of ID by gestational age categories were performed.
We estimated the relative risk of ID from HRs obtained from Cox proportional hazards regression models. We used child’s attained age as primary time scale and adjusted for birth years categorically in all models. We fitted the following sequence of ‘crude’ models: To allow a description of the functional form, we modelled gestational age by restricted cubic splines (five knots (5th, 27th, 50th, 73rd and 95th percentiles of the gestational age distribution)),24 and to allow a comparison of risk estimates in earlier publications, we also modelled gestational age in commonly used categories, that is, <28 weeks (extremely preterm), weeks 28–32 (very preterm), weeks 32–36 (moderate to late preterm), weeks 37–41 term and >41 weeks (post-term).25 Next we adjusted for potential confounding by additional include parameters for maternal age and paternal age. We analysed ID by severity by fitting the previously mentioned models to mild, moderate and severe/profound ID separately. To address potential familial confounding, the sample was restricted to exposure discordant full siblings, and the risk was estimated by fitting stratified Cox model with family identifier as the stratum variable. This approach adjust for unmeasured time-invariant confounding shared by full siblings. Examples of such confounding can be childhood environmental exposures, pregnancy-related factors and lifestyle factors. The proportional hazards assumption was examined using Schoenfeld residuals.26 27 The effect modification was examined by an interaction term between sex and gestational age as well as size for gestational age and gestational age. All statistical tests were performed on the two-sided 5% level of significance. SAS V.9.46 was used for all statistical analyses (Cox regression by PROC PHREG).
Sensitivity analyses
We adjusted for potential confounding by parental history of ID and ASD. We further adjusted for parental education at birth and maternal smoking during pregnancy in a cohort of children born after 1990, where data on these variables were available. To check robustness of ID case definition, we first excluded children with a diagnosis of chromosomal defects and malformations in their first year of age. Second, children were followed from their third birthday and onwards. This is to account for possible outcome misclassification as reliable and validated assessment tools of intellectual function such as the Wechsler scale are only partially available from 2 years and 6 months of age.28 For analysing time trends, the cohort was categorised by birth year, that is, born 1974–1979, 1980–1989, 1990–1999 and 2000–2009, and follow-up time was restricted to 10 years in all groups to avoid biases due to differences in length of follow-up.
Results
Study population
Of 4 406 718 children born alive, we included 3 580 791 born to parents from the Nordic countries. After further exclusion of 5008 with missing gestational age, 3 with missing sex and 2002 with implausible death/emigration date (eg, death date prior to birth), the analytical sample consisted of 3 572 845 live births (online supplemental figure S1). Of the births, 3 078 703 (86.2%) occurred at term, 205 698 (5.8 %) were born preterm and 288 444 (8.1%) were born post-term. Mean age and the highest educational attainment were slightly higher in mothers of children born preterm (table 1).

HR for intellectual disability (ID) according to gestational age (GA). The Cox regression model with child’s age at follow-up as underlying time-scale, adjusted for birth year (5-year intervals from 1974 to 2015 and from 2015 to 2017), maternal age and paternal age (<20, 5-year intervals from 20 to 39, ≥40). Vertical dotted reference lines show very preterm (week 28–31), moderate to late preterm (week 32–37), term (week 37–41) and post-term (week 42–45). Note: GA, gestational age; ID, intellectual disability.
Cohort characteristics by gestational age category (in completed weeks) 3 572 845 live births in Sweden included in this study
Risk of ID
A total of 26 596 incident IDs were recorded during the follow-up. The crude incidence rate was highest among those born extremely preterm (425.6 cases per 100 000 person-years) and lowest among those born post-term (29.5 cases per 100 000 person-years). When adjusted for birth year and parental age at delivery, children born preterm, especially those born extremely preterm, had an increased risk of ID. Shown by Kaplan-Meier curves (online supplemental figure S2), the cumulative incidence of ID was higher for extremely preterm, very preterm and moderate-to-late preterm birth, especially for extremely preterm birth, than that for term and post-term. In the analysis using gestational age in categories, compared with children born at term, the adjusted HR of ID in children born extremely preterm (<28 weeks’ gestation), very preterm (28–31 weeks), moderate-to-late preterm (32–36 weeks), term (37–41 weeks) and post-term (≥42 weeks) were estimated at HR=11.21 (95% CI 10.18 to 12.44), HR=4.79 (95% CI 4.42 to 5.20), HR=2.18 (95% CI 2.09 to 2.27) and HR=1.09 (95% CI 1.05 to 1.14), respectively. For the weekly estimates, the risk gradually decreased with increasing gestational age until week 40. From week 41 onwards, the risk increased again (table 2 and figure 1). Associations between gestational age and risk of ID persisted when we repeated analysis in exposure-discordant siblings (n=677 647) (table 3 and figure 2).

HR for intellectual disability (ID) according to gestational age (GA), in population of full siblings discordant for gestational age. The Cox regression model with child’s age at follow-up as underlying timescale, adjusted for birth year (5-year intervals from 1974 to 2015 and from 2015 to 2017), maternal age, and paternal age (<20, 5-year intervals from 20 to 39 and ≥40). Vertical dotted reference lines show very preterm (week 28–31), moderate to late preterm (week 32–37), term (week 37–41) and post-term (week 42–45). GA, gestational age; ID, intellectual disability.
Rate per 100 000 person-years and HR for the risk of ID in different weeks or categories of gestational age compared with term born children (week 40)
Examination of familial confounding in population of full siblings discordant for gestational age born 1974–2017 in Sweden
ID severity
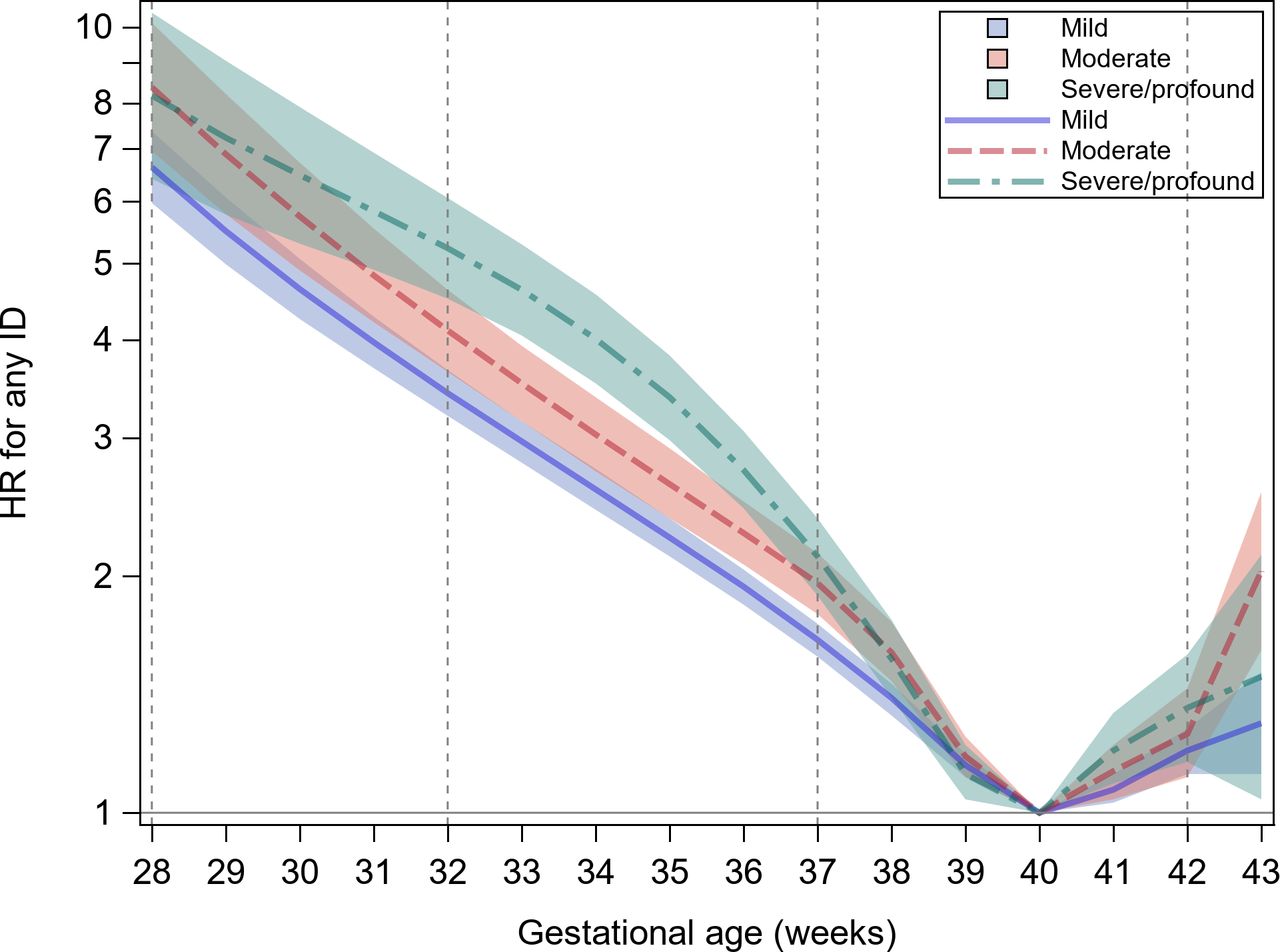
The associations between gestational age and risk of ID were consistent by varying degrees of ID severity at first diagnosis (figure 3). During week 32–37, referenced on week 40, the highest risk was for severe/profound ID, compared with the risks of mild and moderate ID.

{kind=link}
{kind=link}
{kind=link}
HR for mild, moderate and severe/profound intellectual disability (ID) according to gestational age (GA). The Cox regression model with child’s used age at follow-up as underlying timescale, adjusted for birth year (5-year intervals from 1974 to 2015 and from 2015 to 2017), maternal age and paternal age (<20, 5-year intervals from 20 to 39 and ≥40). Vertical dotted reference lines show very preterm (week 28–31), moderate to late preterm (week 32–37), term (week 37–41) and post-term (week 42–45). ID, intellectual disability; GA, estational age.
Subgroup analyses
Male offspring had a higher risk of ID than female offspring across the whole gestational age (online supplemental table S2). When standardised to the risk of ID at week 40, the risk increased for each week away from week 40 in both males and females. Between at week 34 (crude HR for males 2.89, 95% CI 2.76 to 3.02; females 3.23, 95% CI 3.06 to 3.41), 35 (crude HR for males 2.46, 95% CI 2.35 to 2.57; females 2.77, 95% CI 2.64 to 2.92) and 36 (crude HR for males 2.10, 95% CI 2.02 to 2.19; females 2.32, 95% CI 2.22 to 2.43), the risk increase from week 40 was higher in females compared with males, as judged from non-overlapping two-sided 95% CIs of ID risk in each week compared with week 40, for males and females separately (online supplemental figure S3). In subgroups of size for gestational age, compared with AGA infants, children born LGA had higher increased risks for ID for each week away from week 40 during week 33 and 37, whereas children born SGA had higher increased risk at week 37 (crude HR at week 37 for SGA 1.99, 95% CI 1.85 to 2.10; AGA 1.76, 95% CI 1.70 to 1.83; LGA 2.11, 95% CI 1.91 to 2.31) (online supplemental figure S4).
Sensitivity analyses
Estimated risks were slightly attenuated when adjusted for maternal smoking and parental level of education at time of birth (online supplemental table S3). When additionally adjusting for history of parental ID or ASD diagnosis, the results remained essentially unchanged (online supplemental figure S5, table S4). The results remained robust when excluding individuals with chromosomal defects or major malformations (online supplemental figure S6), or when delaying the start of follow-up to 3 years of age (online supplemental figure S7). The risk of ID for preterm children was the lowest among children born <1980 and highest for children born between 2000 and 2009; however, the general trends remained similar within each decade(online supplemental table S5). Inspection of the Schoenfeld residuals did not suggest violation of the proportional hazards assumption (online supplemental figure S8).
Discussion
In this large, nationwide population-based study, which included essentially all children born alive to Nordic mothers in Sweden in 1974–2017, we present weekly estimates on the association between gestational age at birth and risk of ID. We observed a gradual increase in risk of ID from week 40 to week 24, and from week 41 onwards, compared with the infants born week 40. Even within term, we see weekly increases in risk of ID moving away from week 40. These associations were robust in a nested cohort of exposure-discordant siblings. The risk pattern was consistent for mild, moderate and severe/profound ID, most prominent for sever/profound ID and persistent over time.
To our best knowledge, this is the largest population-based study to analyse the association between gestational age and ID risk, with prospectively and independently collected information on exposures and outcome. Including entire birth cohorts with essentially complete follow-up through national health registries minimises risk of selection bias. The large sample size allowed us to detail the risk for every gestational week and to examine severity of ID. Additional sibling comparison analyses allowed to control for unmeasured genetic and environment factors shared by siblings. The study has several limitations. Until approximately 2001, the NPR included only diagnoses from inpatient care increasing the likelihood for under ascertainment of ID in earlier birth cohorts. Information on some confounding variables (ie, parental education and maternal smoking) were only widely available after 1990s. However, analyses in this subsample indicated that these factors were likely not important confounders of the association. We lack information on whether gestational length was determined based on ultrasound or last menstruation that might have introduced measurement errors of gestational age in earlier birth cohorts. Given the observational nature of the study, unmeasured potential confounding, such as maternal alcohol intake, drug abuse, medications during pregnancy and other unknown risk factors, may have influences on our results. Lastly, some misclassification with regards to ID severity cannot be excluded.
Our findings further confirm and expand earlier studies demonstrating higher risks of ID among children born preterm.3 4 13 29–31 Moreover, we described in detail how risk of ID changes across the entire gestational age by week. Beyond preterm and term, we showed that for ID, every gestational week matters. This finding is in line with previous studies on ID13 and cognitive ability,32 which emphasise the varying risk even within the term period. The results from the sibling analysis suggests that the observed increased risks are largely independent of shared familial confounding, in line with previous reports.13 33 However, it is important to keep in mind the limitations in sibling designs, including the possibility of more biased estimates through non-shared confounders.34 With improved survival of extremely and very preterm children, and a thereby growing number of children at higher risk for ID, further investigations are needed to shed light on the underlying mechanisms that most certainly vary over gestational weeks and may affect boys and girls differently.
One known explanation for the increased risk of ID among preterm born children include perturbations in development of the fetal brain due to shortened gestational length.35 Furthermore, preterm born children are often growth restricted leading to decreased glycogen stores in the liver and brain, which can reduce the fetus’ resistance to hypoxia. Underlying mechanisms for the increased risk of ID for post-term may include placental insufficiency leading to a decrease in transfer of oxygen and nutrients to the fetus.36 Furthermore, children born post-term are in general at higher risk for complications resulting from asphyxia.37 Unfortunately, we have no access to placenta examination, biomarkers and other clinical measurements of mother and offspring at the time of delivery to examine the potential underlying mechanism. Further study with biological samples are needed to better understand the pathway associated with this association.
Given the unknown aetiology of ID and the lifelong consequences of the disorder, identifying groups with elevated likelihood of ID is important. Emerging evidence suggest that early detection and intervention of neurocognitive problems in preterm born children may help improve cognitive development.38 Therefore, our finding on the elevated ID risk among children born preterm and post-term may carry important prognostic information that may allow for earlier detection of cases in the future.
Conclusion
The risk of ID increased weekly as the date of delivery moved away from 40 weeks, both preterm and post-term, more pronounced for severe/profound ID compared with mild and moderate ID severity. The results remained robust after detailed adjustment for confounding, including familial confounding, possibly indicating an adverse effect of non-optimal gestational length on ID.
Data availability statement
Data may be obtained from a third party and are not publicly available. Data cannot be shared publicly owing to restrictions by law. Data are available upon request to the Swedish registers (online via bestalladata.socialstyrelsen.se).
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the Swedish Ethical Review Board Stockholm (2017/1875-31/1). Informed consent was not sought as it is assumed that patients do not object to registry-based research provided that the research is deemed ethical by the Ethical Review Board.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
WY and ND contributed equally.
Correction notice This article has been corrected since it first published. The open access licence type has been changed to CC BY. 17th May 2023.
Contributors SS is the principal investigator and guarantor of this study. ND and WY conducted the analysis. ND wrote the draft of the manuscript. WY, MSMP, MP, UA, KT and SS provided substantial scientific input in interpreting the results and drafting the manuscript.
Funding The study was supported by grants from the European Union (H2020-SC1: PM04-2016) and the Seaver Foundation (senior research fellowship for MP).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.