Article Text

Abstract
Objectives To describe rates and variation in uptake of pneumococcal and measles, mumps and rubella (MMR) vaccines in children and associated change in vaccine-preventable diseases (VPDs) across the first and second waves of the COVID-19 pandemic.
Methods Retrospective database study of all children aged <19 registered with a general practice in the Oxford Royal College of General Practitioners Research and Surveillance Centre English national sentinel surveillance network between 2 November 2015 and 18 July 2021.
Results Coverage of booster dose of pneumococcal vaccine decreased from 94.5% (95% CI 94.3% to 94.7%) at its height on International Organization for Standardization (ISO) week 47 (2020) to 93.6% (95% CI 93.4% to 93.8%) by the end of the study. Coverage of second dose of MMR decreased from 85.0% (95% CI 84.7% to 85.3%) at its height on ISO week 37 (2020) to 84.1% (95% CI 83.8% to 84.4%) by the end of the study. The break point in trends for MMR was at ISO week 34 (2020) (95% CI weeks 32–37 (2020)), while for pneumococcal vaccine the break point was later at ISO week 3 (2021) (95% CI week 53 (2020) to week 8 (2021)). Vaccination coverage for children of white ethnicity was less likely to decrease than other ethnicities. Rates of consultation for VPDs fell and remained low since August 2020.
Conclusion Childhood vaccination rates started to fall ahead of the onset of the second wave; this fall is accentuating ethnic, socioeconomic and geographical disparities in vaccine uptake and risks widening health disparities. Social distancing and school closures may have contributed to lower rates of associated VPDs, but there may be increased risk as these measures are removed.
- primary health care
- communicable diseases
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known on this topic
During the first wave of the COVID-19 pandemic in the UK, transient declines in preschool vaccinations were observed.
What this study adds
This study covering the impact of the second and third national lockdowns in the UK showed a small but significant decrease in coverage of measles, mumps and rubella and pneumococcal vaccines over the course of the study. This decrease in vaccine coverage varied by ethnicity, socioeconomic status and location.
Consultations for vaccine-preventable diseases in primary care also decreased to negligible rates from August 2020.
How this study might affect research, practice or policy
It is important to continue to monitor trends in childhood vaccination coverage during the pandemic, especially among children from ethnic minorities and lower socioeconomic groups, as reductions in coverage may lead to widening health disparities.
Introduction
The UK national childhood immunisation programme aims to protect against serious diseases.1 The programme has achieved high vaccination coverage in the population. This is important especially for measles, mumps and rubella (MMR) and pneumococcal vaccinations since these infections have high transmission rates in unvaccinated populations, and a wide range of potentially serious effects in those infected including pneumonia, meningitis and death.2–7
Through 2020/2021 there have been three waves of the COVID-19 pandemic in the UK with varying levels of social distancing, school closure and lockdowns in place.8 9 A systematic review of 17 observational studies during 2020 to assess the impact of the pandemic on childhood vaccination coverage found that there was a decline in the total number of vaccines administered and consequent reduction in coverage, with many children missing out on their vaccine doses.10 Results from a study in over 2600 primary care practices and >35 child health providers found that in the first 3 weeks of social distancing in 2020 in the UK, MMR vaccination counts were 19.8% lower (95% CI −20.7% to −18.9%) than for the same period in 2019.11 12 There were signs of a recovery by April 2020.13
We carried out this research to report any impact of the pandemic on vaccine uptake in children, especially MMR and pneumococcal vaccines, exploring any disparities in coverage over the duration of the pandemic, and to see if there was an impact on vaccine-preventable diseases (VPDs). We report on the first two completed waves, with the third wave ongoing.
Methods
Study design, setting and data sources
We undertook a retrospective study nested within the English national influenza sentinel surveillance network run by the Oxford Royal College of General Practitioners Clinical Informatics Digital Hub (ORCHID). Previous studies demonstrated that the age-sex distribution of patients in the network is broadly similar to the English national census distribution.14 ORCHID data have been used for previous childhood vaccine research.15 The VPDs studied have been reported by the network in its weekly and annual reports for over 50 years.16
Participants
The study included data from all children aged <19 who were registered with a general practitioner between 2 November 2015 and 18 July 2021. We compared any change in birth rate with that reported by the Office for National Statistics (ONS).17
Variables
We extracted data on age, gender and ethnicity which were recorded using an ontology to maximise identification,18 socioeconomic status measured using the Index of Multiple Deprivation (IMD)19 20 and rurality using the ONS classification based on individual-level postcode.21 We have used practice postcode to assign IMD and household setting where no valid patient postcode was available (~3%).
We also extracted vaccination status and consultations for VPDs from the pseudonymised vaccination record and computerised medical records of all children <19 within the network using the Systematized Nomenclature of Medicine-Clinical Terms (SNOMED-CT).22
Statistical analysis
Calculation of childhood vaccination rates and rates of VPDs
Weekly vaccination coverage for the first dose of MMR was calculated by dividing the number of children <2 who had been given one dose of MMR by the number of children <2 registered within the ORCHID network that week. Coverage for the second dose of MMR was calculated similarly for children <5 who had been given two doses.
Weekly vaccination coverage for the first dose of pneumococcal vaccine was calculated by dividing the number of children <1 who had been given one dose of pneumococcal vaccine by the number of children <1 registered within the ORCHID network that week. Coverage for the booster dose of pneumococcal vaccine was calculated similarly for children <2 who had been given two doses. To account for the change from a three-dose schedule in 2020,23 our definition of pneumococcal vaccine coverage prior to 1 January 2020 counted children who had had three doses of pneumococcal vaccine. The second/third dose of pneumococcal vaccine will be referred to as booster dose of pneumococcal vaccine henceforth.
Weekly VPD rates were calculated by dividing the total number of consultations for VPDs per week by the number of children registered within the ORCHID network. The list of vaccines, VPDs and their associated SNOMED-CTs used for this study is included in online supplemental appendix 1.
Supplemental material
Data are presented graphically by the International Organization for Standardization (ISO) week.24
Segmental linear regression analysis and examination of inequalities in vaccination trends
Linear regression was used to model trends in vaccination coverage and to identify inequalities by ethnicity, IMD and urban/rural location.
Segmental linear regression analysis was used to identify any break points in the vaccination trends. This regression analysis uses an iterative process to estimate the slopes and break points in generalised linear models which have one or more segmented relationships in the predictor.25
Inequalities in coverage following break points in the vaccination trend were of particular interest, thus an interaction term between ethnicity and break point was added to the regression model. Similar analysis was undertaken to examine the inequalities by IMD and urban/rural location.
Statistical analyses were undertaken using R V.3.5.1.
Ethical considerations
This study was classified as a service evaluation (measuring what standard of care is achieved) by the Medical Research Council/Health Research Authority decision tools26 so did not require formal ethics approval; it was approved by the RCGP Approval Committee (data request ORC_05_2020). This study does not include patients who opted out of record sharing, approximately 2%.
Results
The population
The number of registered children <19 whose data contributed to the analysis reduced from 1 094 150 in 2015 to 1 043 968 in 2021 (see table 1). This fall of 4.6% is smaller than the decrease in the proportion of live births over this period of 11.8% reported by ONS.27 28 There was a 6.3% lower proportion of children of white ethnicity over the course of the study, while the proportion of births of children of white ethnicity decreased by 3.7% between 2015 and 2019.27 29
Cross-sectional profile of population at start and end of the study compared with midyear population estimates from the Office for National Statistics
Trends in childhood vaccinations
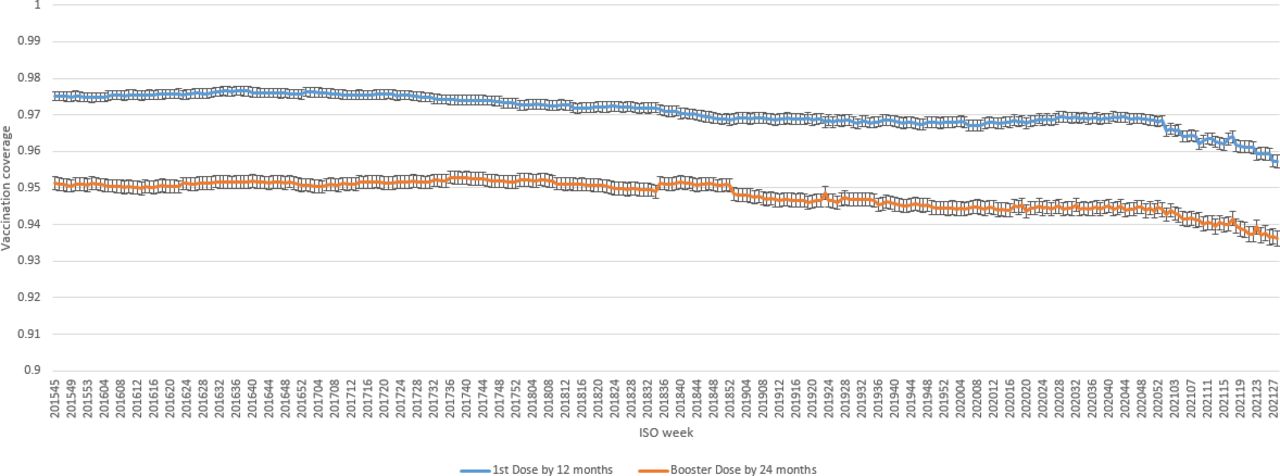
Coverage of pneumococcal booster doses decreased from 94.5% (95% CI 94.3% to 94.7%) on ISO week 47 (2020) to 93.6% (95% CI 93.4% to 93.8%) by the end of the study. In turn, coverage of the second dose of MMR decreased from 85.0% (95% CI 84.7% to 85.3%) on ISO week 37 (2020) to 84.1% (95% CI 83.8% to 84.4%) by the end of the study (see figures 1 and 2).

Trends in weekly pneumococcal vaccination rates (and 95% CI) over the last 5 years. ISO, International Organization for Standardization.

Trends in weekly measles, mumps and rubella (MMR) vaccination rates (and 95% CI) over the last 5 years. ISO, International Organization for Standardization.
Segmental linear regression analysis showed that the break point in trends for booster dose of pneumococcal vaccine was at ISO week 3 (2021) (95% CI ISO week 53 (2020) to week 8 (2021)), while the break point for trends in the second dose of MMR was at ISO week 34 (2020) (95% CI ISO weeks 32–37 (2020)). The segmental regression analysis showed that the break point in trends for the first dose of MMR was at ISO week 21 (2019) (95% CI ISO week 18 (2019) to week 23 (2019)), while the break point in trends for the first dose of pneumococcal vaccine was at ISO week 53 (2020) (95% CI ISO week 49 (2020) to week 4 (2021)).
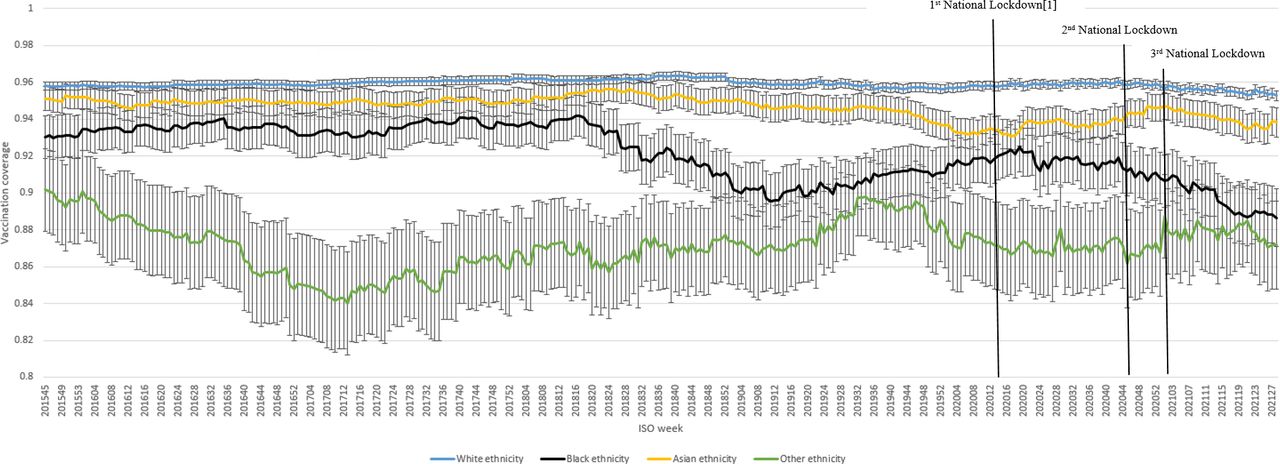
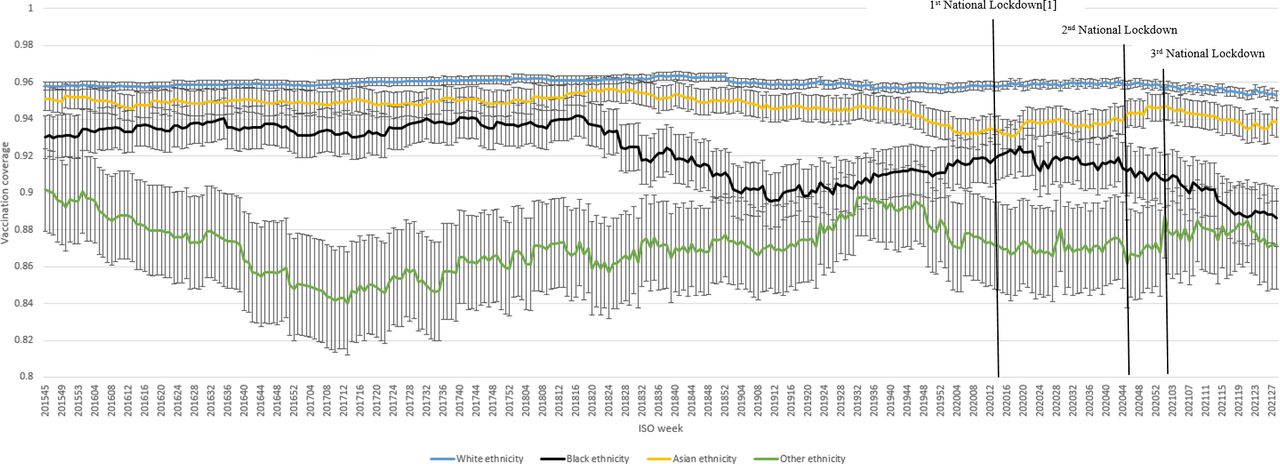
Vaccination coverage had reduced for children of all ethnicities (see figures 3 and 4). Coverage declined less in children of white ethnicity than other ethnic groups following the break point, especially for the second doses of MMR. Compared with children of white ethnicity, coverage of the second dose of MMR following the break point reduced by −0.041 (95% CI −0.045 to −0.038) per week for children of black ethnicity and −0.002 (95% CI −0.005 to −0.0009) per week for children of Asian ethnicity.
Trends in weekly rates of coverage of booster dose of pneumococcal vaccine (and 95% CI) over the last 5 years by ethnicity. ISO, International Organization for Standardization.

Trends in weekly rates of coverage of second dose of measles, mumps and rubella (MMR) (and 95% CI) over the last 5 years by ethnicity. ISO, International Organization for Standardization.
The reduction in coverage of pneumococcal booster doses per week following the break point was −0.0071 (95% CI −0.0097 to −0.0045) for children of black ethnicity compared with children of white ethnicity. In contrast, coverage of pneumococcal booster doses increased by 0.0084 (95% CI 0.0104 to −0.0068) per week for children of Asian ethnicity compared with children of white ethnicity (see table 2). Similar inequalities were observed for coverage by urban/rural location (see table 3 and figures 5 and 6).
Average reduction in vaccine coverage per week following the break point by ethnicity (95% CI)
Average reduction in vaccine coverage per week following the break point by urban/rural location (95% CI)

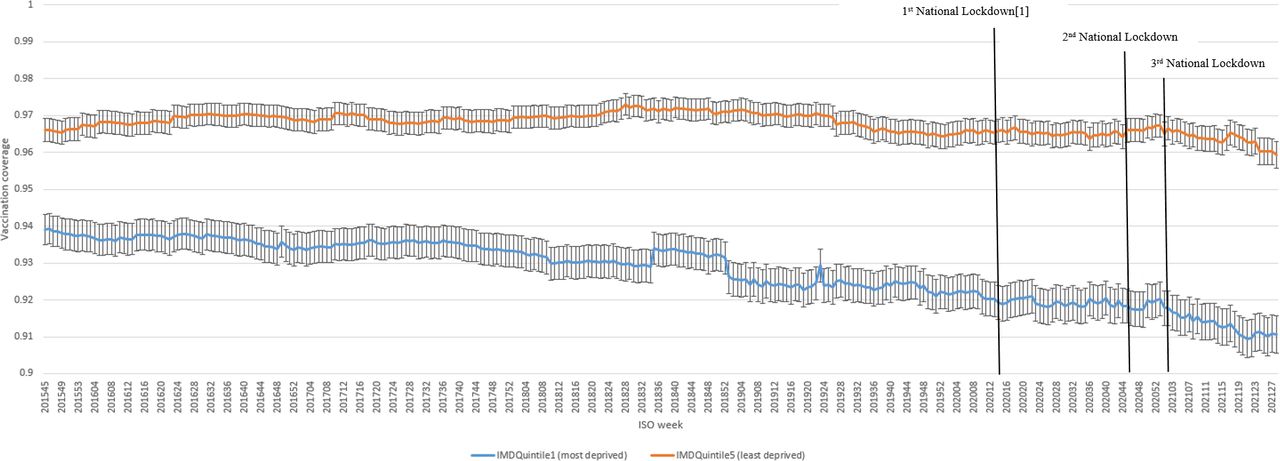
Trends in weekly rates of coverage of booster dose of pneumococcal vaccine (and 95% CI) over the last 5 years by Index of Multiple Deprivation (IMD). ISO, International Organization for Standardization.

Trends in weekly rates of coverage of second dose of measles, mumps and rubella (MMR) (and 95% CI) over the last 5 years by Index of Multiple Deprivation (IMD). ISO, International Organization for Standardization.
For each quintile increase in IMD, the average rate of change in second dose of MMR coverage was 0.0099 (95% CI 0.0092 to 0.0105), while the average change in coverage of pneumococcal booster doses was 0.0014 (95% CI 0.00091 to 0.0018) (see figures 7 and 8).
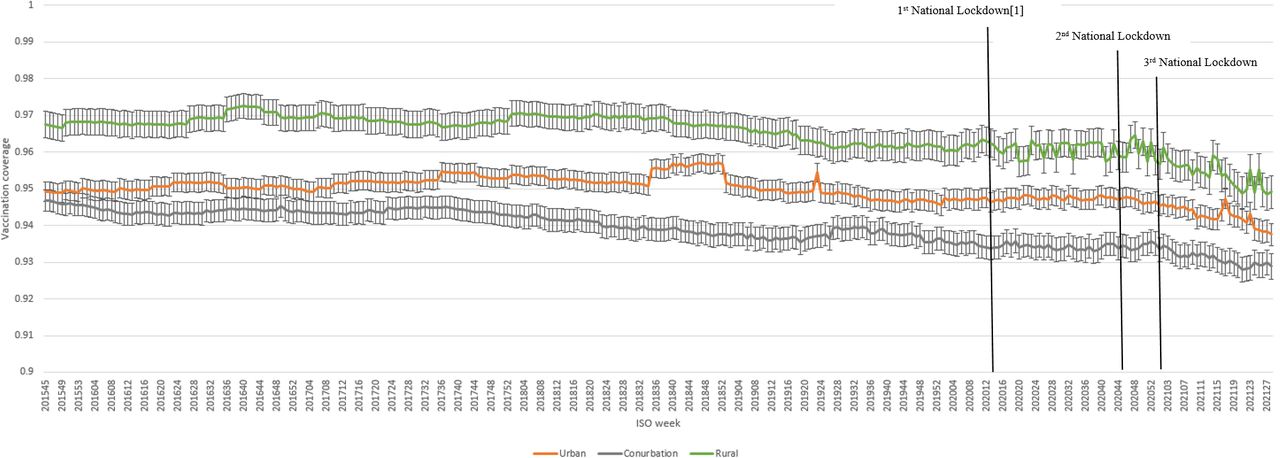
Trends in weekly rates of coverage of booster dose of pneumococcal vaccine (and 95% CI) over the last 5 years by rural/urban location. ISO, International Organization for Standardization.

Trends in weekly rates of coverage of second dose of measles, mumps and rubella (MMR) (and 95% CI) over the last 5 years by rural/urban location. ISO, International Organization for Standardization.
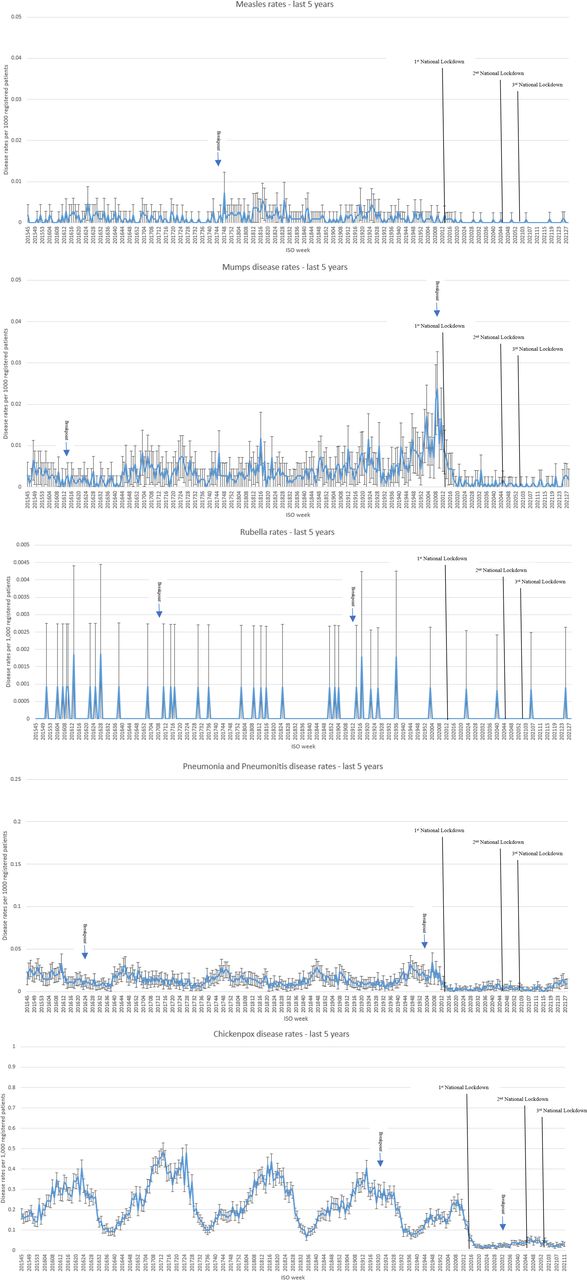
Trends in VPDs over the last 5 years
Presentation of VPDs had reduced to negligible rates by week 32 (2020). Figure 9 showed that the break point in trends for mumps disease rates was within 1 week of the first national lockdown. The break points in trends for VPD rates were less clearly associated with the national lockdowns.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Trends in weekly vaccine-preventable disease (VPD) rates over the last 5 years. ISO, International Organization for Standardization.
Discussion
Principal findings
The COVID-19 pandemic has had a small but significant effect on coverage of childhood pneumococcal and MMR vaccinations.
Coverage for pneumococcal booster doses at the end of our study was 93.6% (95% CI 93.4% to 93.8%). This is comparable to data published by Public Health England (PHE) which showed that pneumococcal conjugate vaccine coverage in children 12 months of age was 93.4% in the first quarter of 2021.30
In turn, the coverage for second dose of MMR at the end of our study was 84.1% (95% CI 83.8% to 4.4%), which is lower than the published data which showed MMR coverage in children 24 months of age was 89.3% in the first quarter of 2021.30
There were significant ethnic, socioeconomic and urban/rural differences in vaccination coverage, especially for MMR.
In our study, so far, there have been no recorded increases in VPDs among children, with negligible consultation rates for most VPDs. This may have been confounded by cases not presenting to healthcare or by cases presenting to parts of the National Health Service (NHS) other than general practice, with a subsequent delay in reporting and recording in the primary care record. Data from the WHO for all four nations of the UK showed that between 2019 and 2020, the number of cases of measles had reduced by 91.3%, mumps by 31.2% and rubella by 100%. In contrast, globally between 2019 and 2020, measles cases reduced by 82.8%, mumps increased by 157.8% and rubella reduced by 79.3%.31
Strengths and weaknesses
The strengths of our study include its large sample size from a nationally representative sentinel network, the long period covered with weekly vaccine coverage rates, including data covering the second and third national lockdowns; and that we covered trends in both vaccine coverage and VPD rates.
A limitation of our study involves the quality of recording in routinely collected data. Our sentinel network has been involved in monitoring respiratory infections and vaccinations for over 50 years and has had regular feedback on data quality.14 16 Another limitation relates to the duration of our study, which covered a number of changes to the childhood vaccination schedule, including the change to a two-dose pneumococcal conjugate vaccine schedule in 2020. Changes to the two-dose pneumococcal vaccine schedule have been taken into account in this study, although the broader changes in the childhood vaccination programme have not been adjusted for in this analysis. Our study only covered two vaccinations as these infections have high transmission rates in unvaccinated populations, and the resulting VPDs associated with low vaccine coverage are likely to be the first to become apparent. However, the trends in these two vaccinations may not reflect the trend in all childhood vaccination rates, especially those provided outside primary care.
It is important to note that changes in coverage associated with marked reductions in vaccine administrations will be delayed.32 For example, most children who turn 2 years of age during the early months of the pandemic will have received the first dose of MMR and the pneumococcal booster well before the start of the pandemic. Therefore, changes in coverage that occur because of decreased vaccine administrations during the pandemic will not be seen until weeks when a substantial proportion of children have turned 2 years old. Our methodology for calculating vaccination coverage has allowed us to compare our results directly with national published statistics.30 However, as our study takes in a larger window of observation than stipulated by the NHS vaccination schedule, it may be less sensitive to secular trends in coverage.32
Finally, our definition of VPDs included pneumonia or pneumonitis, not all of which are vaccine-preventable cases. Conversely, in the setting of COVID-19, care-seeking patterns might be quite different for respiratory illnesses in particular, and some cases of COVID-19 (particularly among adolescents) might be classified as ‘pneumonia or pneumonitis’ under the definition that we have used.
Interpretation, unanswered questions and need for further work
It is reassuring that this large representative data set indicates general practice delivery of childhood immunisations has remained good, especially during the first lockdown. Our study is comparable to data from WHO and PHE,30 31 33 34 although the coverage rates for MMR are lower in our data set than the PHE. This may be the result of some vaccinations being given in community settings not attached to a general practitioner.
Our results show that pneumococcal vaccine coverage has been declining steadily over time and accelerated in the pandemic. In contrast, MMR coverage seemed to be increasing but this plateaued in the pandemic. There are a number of possible explanations for this observed decline in these childhood vaccination rates, including the pivotal role general practice has played in the national COVID-19 vaccine implementation.35 Early studies showed that general practice-led sites delivered two in three of all COVID-19 vaccinations in England between December 2020 and April 2021,36 this may have impacted capacity for routine vaccinations during the period of our study.
There are a number of possible explanations for the differential decline in coverage by ethnicity, socioeconomic status and geographical location. Ethnic and socioeconomic differences in parents’ perception of the importance of immunisations, whether immunisations were permitted or culturally acceptable and their understanding of immunisation schedules have been shown to affect immunisation decisions.37 38 Recent research on COVID-19 vaccines have found a marked difference in vaccine hesitancy by race/ethnicity,39–41 with a much greater proportion of ethnic minority populations expressing concern about side effects and the long-term effects of vaccines on health. Some have capitalised on this lack of trust in vaccines to spread misinformation.42 This differential decline in coverage may also reflect access barriers, including difficulties in accessing vaccination appointments during the pandemic.43–45 Thus, it is important to continue to monitor these trends to record any reduction in coverage from the second and third lockdowns, especially among ethnic minority groups and lower socioeconomic groups which will lead to widening health disparities.38 46
These data show that there may be an increasing risk of preventable serious childhood diseases if the modest reductions in vaccination rates are not rapidly reversed especially in those populations with greater rates of decline.47 48 The drive to offer COVID-19 booster vaccinations in adults and the expansion of COVID-19 vaccinations for children should not be at the expense of routine childhood immunisation rates.
Ethics statements
Patient consent for publication
Ethics approval
This study was classified as a service evaluation (measuring what standard of care this service achieved) by the Medical Research Council/Health Research Authority decision tool so did not require formal ethics approval; it was approved by the Royal College of General Practitioners (RCGP) Approval Committee (data request number: ORC_05_2020). This study does not include patients who opted out of record sharing, approximately 2%.
Acknowledgments
FDRH acknowledges the support from the National Institute for Health Research (NIHR) Oxford and Thames Valley (OTV) Applied Research Collaboration (ARC), and the NIHR Oxford University Health (OUH) Biomedical Research Centre (BRC).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
FDRH and AJP are joint senior authors.
Twitter @Lusignan_S
UH, MJ and JS contributed equally.
Contributors The study was conceived by all authors. The funding was awarded to SdL. UH and MJ carried out the statistical analysis. UH wrote the first draft. All authors contributed to the interpretation of results and revisions of the manuscript. UH is guarantor for the study and accepts full responsibility for the work and/or the conduct of the study, had access to the data, and controlled the decision to publish
Funding This study was funded by the University of Oxford’s Medical Sciences Division (MSD) as part of the COVID-19 Research Response Fund (study reference number: 0009531).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.