Article Text

Abstract
Objective Determine non-invasive ventilation with continuous positive airway pressure (CPAP) outcomes for paediatric respiratory distress in low-income and middle-income countries (LMICs).
Design Systematic review and meta-analysis.
Setting LMIC hospitals.
Patients One month to 15 year olds with respiratory distress.
Interventions We searched Medline, Embase, LILACS, Web of Science and Scopus on 7 April 2020. Included studies assessed CPAP safety, efficacy or effectiveness. All study types were included; neonatal only studies were excluded. Data were extracted by two reviewers and bias was assessed. Certainty of evidence was evaluated, and risk ratios (RR) were produced for meta-analyses. (PROSPERO protocol CRD42018084278).
Results 2174 papers were screened, 20 were included in the systematic review and 3 were included in two separate meta-analyses of mortality and adverse events. Studies suitable for meta-analysis were randomised controlled trials (RCTs) from Bangladesh, Ghana and Malawi. For meta-analyses comparing death or adverse events between CPAP and low-flow oxygen recipients, we found no clear CPAP effect on mortality (RR 0.75, 95% CI 0.33 to 1.72) or adverse events (RR 1.52, CI 0.71 to 3.26). We downgraded the certainty of evidence for both death and adverse events outcomes to ‘low’ due to design issues and results discrepancies across RCTs.
Conclusions Evidence for CPAP efficacy against mortality and adverse events has low certainty and is context dependent. Hospitals introducing CPAP need to have mechanisms in place to optimise safety in the context it is being used; this includes the location (a high dependency or intensive care area), adequate numbers of staff trained in CPAP use, close monitoring and mechanisms for escalation, daily direct physician supervision, equipment that is age appropriate and user-friendly and continuous monitoring of outcomes and quality of care.
- respiratory medicine
- paediatrics
- infectious disease medicine
- global health
- child health
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic?
Lower respiratory infections (LRIs) like pneumonia are the leading infectious cause of paediatric death globally despite antibiotics and oxygen treatment.
Non-invasive ventilation (NIV) with continuous positive airway pressure (CPAP) is an accepted paediatric treatment modality in high-income countries and for severely ill neonates in low-income and middle-income countries (LMICs).
The most up-to-date research evaluating the efficacy, effectiveness and safety of CPAP NIV for severe LRI of non-neonates has been reported but not systematically assessed and evaluated by meta-analysis.
What this study adds?
This systematic review and meta-analysis synthesises the most updated body of evidence for non-neonates treated with CPAP NIV in LMICs.
We provide key evidence-based recommendations for hospitals in LMICs who have already implemented CPAP NIV for the management of non-neonates with severe respiratory illnesses like LRIs.
Introduction
Significant progress has been made in reducing the global mortality burden for children during the last 20 years. Despite this, nearly 5.4 million children worldwide below 5 years old died in 2017.1 Reflecting historical mortality trends, lower respiratory infections (LRIs) are disproportionately represented, accounting for more deaths among 1–59 month olds than any other illness.1 Various efforts, including WHO treatment guidelines and the Millennium and Sustainable Development Goals, have contributed to child mortality reductions from LRIs.1 However, large respiratory mortality disparities persist in low-income and middle-income countries (LMICs).2
Current management of LRIs and respiratory distress include medical therapies in addition to respiratory support. In many LMICs, the highest level of respiratory support is conventional low-flow oxygen. Larger hospitals may have some capacity for more intensive management, including non-invasive ventilation (NIV) with continuous positive airway pressure (CPAP) and intubation with invasive mechanical ventilation (IMV), but the necessary equipment, medications and human resource capacity makes this infrequent.
CPAP NIV provides positive airway pressure to a spontaneously breathing individual to improve lung compliance, ventilation-perfusion mismatch, gas exchange and work of breathing.3 In high-income countries, CPAP is a standard of care for paediatric respiratory patients with respiratory distress and can reduce IMV and mortality. In LMICs, ‘bubble CPAP’ (bCPAP) may particularly benefit neonatal respiratory distress (<28 days old). bCPAP, unlike conventional CPAP, generates pressure according to the depth the circuit’s expiratory limb is submerged below water.3 A systematic review of neonatal bCPAP in LMICs demonstrated a 30%–50% reduction in IMV but without a mortality change.4 Similarly, a systematic review of high flow nasal cannula oxygen found that, when compared with CPAP, CPAP had a lower treatment failure risk among infants with younger age, hypoxemia or respiratory distress.5 No mortality difference was found. CPAP NIV safety concerns include possible excessive oxygen delivery, skin and/or nasal septal damage, aspiration and, rarely, pneumothorax.
While neonatal bCPAP in LMICs is widely considered beneficial and safe, CPAP efficacy, effectiveness and safety for non-neonates in LMICs has been a recent focus. A systematic review of the literature through 2018 concluded bCPAP was safe and effective in LMICs.6 However, recent research has raised new questions regarding CPAP for non-neonates. This study’s main objective was to systematically review the literature to determine through meta-analyses if CPAP is efficacious, effective, and safe for 1 month to 15 years olds with respiratory distress in LMICs.
Methods
The development and reporting of this work are per the Preferred Reporting Items for Systematic Reviews (PRISMA) statement.7 The protocol was registered on PROSPERO (CRD42018084278).
Data sources and search strategies
A search of Medline, Embase, LILACS, Web of Science and Scopus was performed on 7 April 2020 (table 1). There were no language, age, publication date or type restrictions. The World Bank LMIC classification was applied. The search strategy was facilitated by a medical reference librarian (online supplemental appendix 1). The references of included studies were also searched.
Supplemental material
Search strategy
Inclusion and exclusion criteria for systematic review
All studies published in peer-reviewed journals on NIV efficacy, effectiveness or safety in the population of interest were included. We defined NIV as bCPAP or CPAP. Editorials, letters, narratives, systematic reviews and errata were excluded. Included studies assessed hospital CPAP efficacy, effectiveness or safety for 1 month to 15 years old with respiratory distress in LMICs. Studies on neonates (<28 days old) only were excluded.
Data collection and extraction for systematic review
Search keywords are in online supplemental appendix 1. The online Covidence platform for data extraction and quality assessments was used. Two independent reviewers screened each study by title and abstract. Eligible studies underwent a full review. Disagreements at the title and abstract stage were resolved by a third blinded author; disagreements at the manuscript review stage were resolved by consensus. A data extraction tool was created in Covidence to collect author, funding, setting, study design, population, interventions and outcomes data.
Risk of bias assessment for studies included in systematic review
Data extraction and risk of bias assessments were performed by two independent reviewers and discrepancies were adjudicated by consensus. Comparative studies, including all randomised control trails (RCTs), were evaluated using Cochrane recommended criteria.8 Studies with no comparator group were evaluated using criteria proposed by Murad et al to evaluate selection, ascertainment, causality and reporting domains.9
Data synthesis, assessment of reporting biases and assessment of heterogeneity
The feasibility of meta-analyses was assessed using clinical and methodological characteristics for all study designs. Random-effects models summarised study findings using an inverse variance method. For dichotomous outcomes, risk ratios (RR) or ORs and 95% CIs estimated the treatment effect. We used difference in means for continuous outcomes. We created and evaluated a funnel plot to evaluate for reporting biases. We estimated statistical heterogeneity using the χ2 test and the I 2 statistic. The latter describes the proportion of variation across studies due to heterogeneity rather than sampling error. All statistical analyses were done using Stata V.16.1 (Stata, College Station, Texas, USA).
Certainty of evidence assessment
For studies contributing data to meta-analyses, we used GRADEpro GDT software (GRADEpro GDT 2015) to apply the Cochrane-recommended GRADE domains of study limitations, consistency of effect, imprecision, indirectness and publication bias to evaluate evidence quality.10 When appropriate limitations were identified, we downgraded evidence according to guidelines.
Role of the funding source
There was no direct funding. The corresponding author had full access to all study data and final responsibility for submission.
Results
Systematic review
A total of 2174 studies were screened and 20 were included in the systematic review (figure 1). These included 5 RCTs,11–15 1 cluster RCT,16 1 non-randomised comparative study17 and 13 observational studies18–28 (table 2). Most studies evaluated bCPAP or conventional CPAP and were small. Ten studies also included neonates. Sixteen studies were at tertiary referral or provincial hospitals and included intensive care or high acuity units. Four studies, including RCTs in Malawi14 and Ghana,16 were at district hospitals in a general paediatric ward. The Ghana RCT had daily physician oversight while the Malawi RCT did not. Mortality was the primary endpoint in seven studies. In the Bangladesh RCT, bCPAP was delivered in an intensive care unit (ICU) under paediatric intensive care physician supervision.12
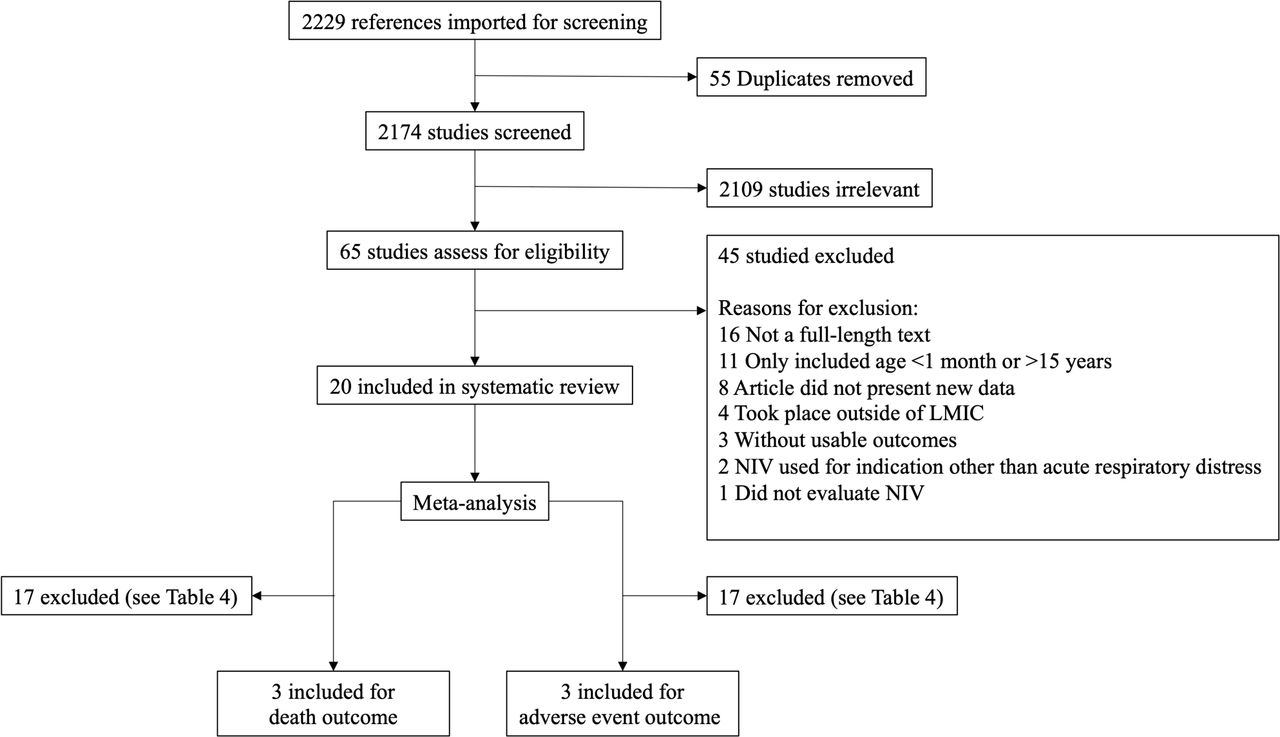
Study selection. LMICs, low-income and middle-income countries; NIV, non-invasive ventilation.
Characteristics of included studies
RCTs and mortality
For the five RCTs, CPAP mortality varied from 0% to 22% (table 3). Mortality or treatment failure served as primary endpoints for all. In the Bangladesh RCT, children on bCPAP compared with low-flow oxygen had lower mortality (4% bCPAP vs 15% oxygen: RR 0.25, 95% CI 0.07 to 0.89; p=0.022).12 The study was stopped early by the data safety monitoring board for benefit. A second RCT in Ghana used a cluster crossover design in which CPAP was available at one hospital at a time, while the other hospital was the control.16 Children at the intervention hospital received CPAP and at both hospitals, supplemental oxygen was provided as needed to maintain oxygenation >92%. The proportion of controls receiving oxygen was not reported. This trial found no difference in all-cause mortality between CPAP (3%) and controls (4%) (RR 0.67, 95% CI 0.42 to 1.08; p=0.11). An exploratory adjusted analysis demonstrated decreased mortality for <1 year olds on CPAP (3%) compared with controls (7%) (RR 0.40, 95% CI 0.19 to 0.82; p=0.01).16 Another RCT in Malawi comparing bCPAP to low-flow oxygen found higher mortality in the bCPAP arm (17% and 11%, RR 1.52; 95% CI 1.02 to 2.27; p=0.036).14 This study was stopped early due to both futility and the possibility of harm from bCPAP. In an open, prospective RCT from Vietnam involving 37 children with respiratory distress from dengue, 18 received CPAP and 19 received oxygen. Mortality was 22% after CPAP compared with 0% for controls (p=0.03).9
Outcomes for randomised control trials
Observational studies and mortality
Among the 11 observational studies, CPAP mortality ranged from 0% to 55% (table 4). Four tertiary hospital studies reported mortality >30%.20 26–28 Mortality was the primary endpoint for five prospective observational studies and was 2%,18 10%,19 29%,25 33%26 and 47%.28 Results from several studies suggested multiple comorbidities may detrimentally influence outcomes. Specifically, two studies with high all-cause mortality among CPAP recipients reported fewer deaths among HIV-uninfected patients with very severe pneumonia and single organ failure.26 28
Outcomes for non-randomised control trials
Non-fatal adverse events (AEs)
Sixteen studies reported non-fatal AEs (table 3A,B). Six of these reported no AEs. AEs in the other seven studies were 3%–22%. One study reported a 79% AE rate including infections.17 When infections were excluded, the AE rate was 22%. Most AEs were mild and included trauma to the nasal septum, skin and eyes, vomiting and abdominal distension.14 16 17 19–21 26 A few serious AEs including the development of heart failure, aspiration and pneumothorax were reported.12 14 16 21
Risk of bias assessment for systematic review
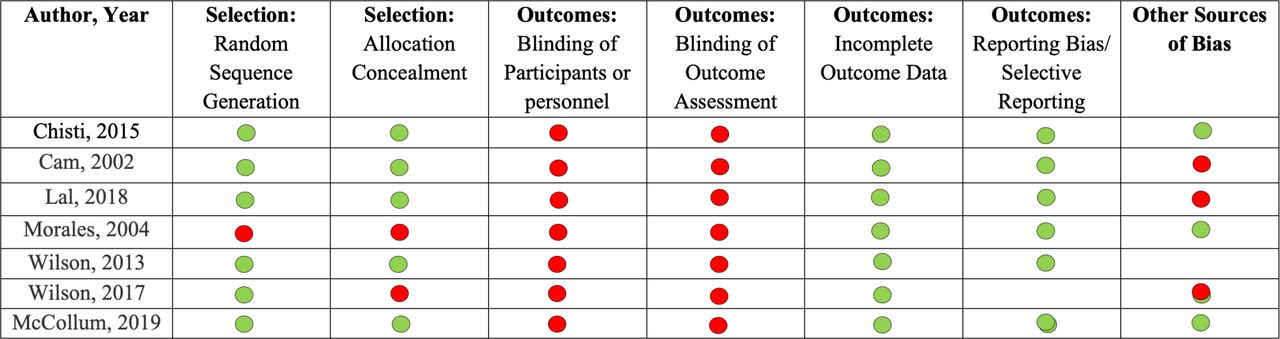
Due to the inability to blind the respiratory therapy intervention, no RCT was blinded from participants, personnel or outcome assessors (figure 2). One study was not randomised17 and another RCT used a cluster crossover design and randomised at the hospital level.15 All seven studies had low risk of incomplete data or reporting bias.

Risk of bias assessment for RCT and prospective comparative studies.
Five observational studies had unclear or high risk of selection bias due to inconclusive reporting (online supplemental file 1).18 25 27 29 30 All studies were considered low risk of ascertainment bias. Due to the observational design, 10/13 studies were considered unclear or high risk of causality bias. Risk of causality bias was assigned based on potential alternate causes, presence of a challenge/rechallenge phenomenon and appropriate follow-up duration.9
Meta-analysis
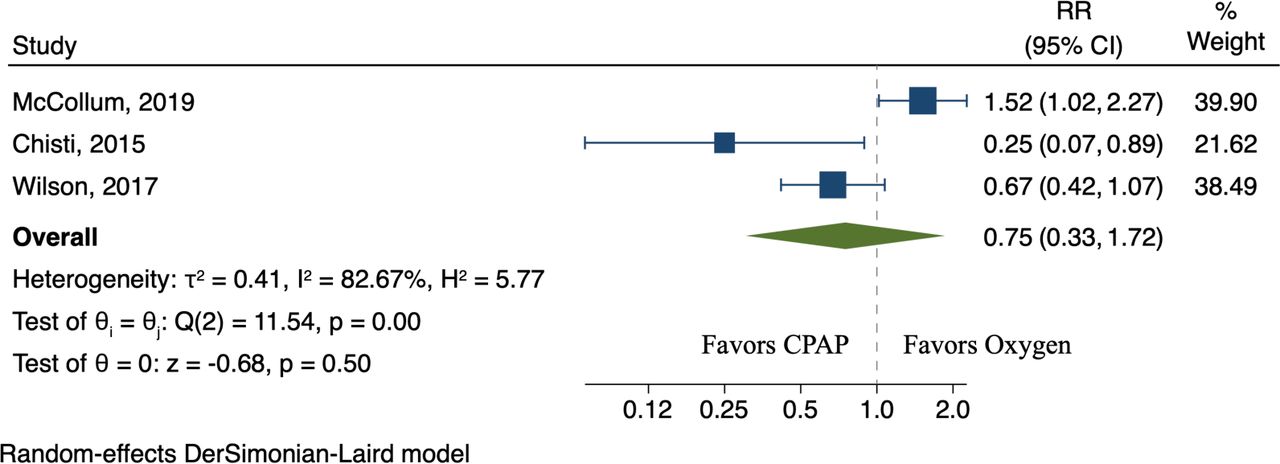
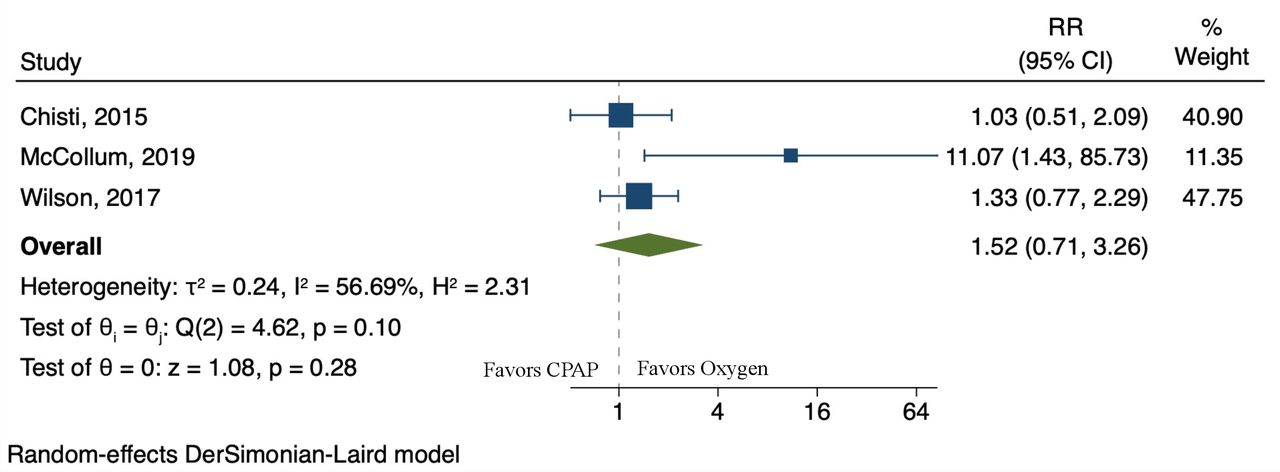
The RCTs in Bangladesh, Ghana and Malawi were found suitable for inclusion in a meta-analyses for the efficacy of CPAP against mortality and adverse events (figure 1). Meta-analyses for other trial endpoints or with observational studies were not suitable due to incomparability of endpoints and populations, and high risk of bias (table 5). The combined RR of CPAP, compared with low-flow oxygen, was 0.75 (95% CI 0.33 to 1.72), indicating no conclusive mortality benefit (figure 3). We measured I 2 to be 82.67%, consistent with considerable heterogeneity (online supplemental appendix 2). For AEs, the combined RR of CPAP, compared with low-flow oxygen, was 1.52 (95% CI 0.71 to 3.26), which is similarly inconclusive for AE risk (figure 4). Heterogeneity was also high (I 2 56.69%) (online supplemental appendix 3).

Meta-analysis of trials assessing CPAP against mortality in children less than 5 years. CPAP, continuous positive airway pressure.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Meta-analysis of trials assessing CPAP against adverse events in children less than 5 years. CPAP, continuous positive airway pressure.
Meta-analysis study selection
Certainty of evidence assessment
The overall certainty of evidence for the outcomes of death and adverse events was low (table 6). Evidence certainty was downgraded two levels for both outcomes due to lack of blinding of participants, personnel or during analysis, as well due to the varying RR estimates of death and also adverse events, little CI overlap and high heterogeneity.
Certainty of evidence (GRADE)
Discussion
We completed a systematic review and meta-analysis of studies on CPAP and its effect on mortality, and adverse events among 1 month to 15 year olds in LMICs. Overall, the summary estimate from the meta-analyses of three RCTs found both inconclusive and low certainty evidence for CPAP efficacy against death and adverse events, compared with oxygen, for 1–59-month-old children with respiratory distress in LMICs. Our findings suggest that facilities in LMICs using CPAP should monitor outcomes closely and pay attention to the context in which CPAP has been most efficacious: this includes the location (a high dependency or intensive care area), adequate numbers of staff trained in CPAP use, close monitoring and mechanisms for escalation, daily direct physician supervision and equipment that is age appropriate and user-friendly.
The different contexts of the three RCTs included in these meta-analyses are important. While the Bangladesh RCT was stopped after an interim analysis showed evidence of a mortality benefit of CPAP in that context, some argued the trial’s closure was premature.31 In Bangladesh, the setting was an ICU with daily physician supervision and trained nurses. The Ghana RCT did not demonstrate any difference in the primary mortality outcome. However, in an exploratory analyses of the outcomes for children less than 1 year of age, the authors observed a mortality benefit for CPAP compared with controls. It was unclear what proportion of controls received oxygen and the low hypoxemia prevalence suggests it is few. Severity of illness and comorbidity is an important case-mix difference in the three RCTs, as in the other two trials oxygen was administered to all controls. The Ghana RCT was also conducted under physician oversight in a district hospital emergency department. Finally, the Malawi RCT was stopped early for both futility and potential harm from CPAP. This trial enrolled sicker children than in Ghana (all participants had at least one comorbidity or hypoxemia), and the trial was conducted in a district paediatric ward hospital with trained staff but without daily physician oversight.
When reviewing all AEs, excluding mortality, we found them to be rare and generally minor, although meta-analysis findings were inconclusive. Significant AEs were even rarer and included aspiration, pneumothorax and development of heart failure. Investigators from the Malawi trial postulate that aspiration or cardiopulmonary interactions leading to reduced cardiac output may have influenced their findings.32 While these results are inconclusive on the effect of CPAP on mortality, they still provide useful guidance for CPAP use in LMICs. We suggest that CPAP is used only with direct physician oversight in an ICU, high dependency or dedicated unit with overall patient to staff ratios no higher than 5:1.
Given this mixed evidence, further research is needed as more paediatric services in LMICs consider whether to implement CPAP. A strong understanding of which patient populations will derive maximum benefit from CPAP in resource-constrained settings is essential. In addition, as intensive care modalities become more common in LMICs, attention must be given to the impact of intensive care on resource utilisation. This is particularly important for a more resource intensive modality like CPAP where evidence remains low certainty and context specific. For example, if oxygen concentrators are used for bCPAP gas flow, then one child occupies one entire oxygen concentrator. Oxygen flow from the same concentrator could in turn simultaneously treat up to five total children requiring oxygen.33 Nevertheless, an understanding of the context in which CPAP safety can be optimised can be derived from the three trials.
In sum, this systematic review demonstrates current data for CPAP has overall low certainty and is inconclusive on a mortality benefit, but adverse events are few. The current literature is helpful in understanding the context in which CPAP can be safe as a part of the overall management of acute respiratory infections in children.
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study.
Ethics statements
Patient consent for publication
Acknowledgments
We would like to thank Ann Farrell, Peggy Murphy and the medical library staff at Mayo Clinic and Lurie Children’s Hospital who helped with search criteria and performed the searches.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @tinylungsglobal
Contributors KLS and EM had full access to data in the study and take full responsibility for the integrity of the data and the accuracy of the data analysis. KLS and EM conceived the study idea and designed the study. KLS and EM with the help of multiple medical librarians created the search terms and conducted the database searches. KLS and PJH extracted and analysed the data. BW conducted the meta-analysis. KLS, AGS, PJH, BW, TM, MJC, RWC and EM drafted and revised the manuscript. EDM is the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.