Article Text

Abstract
Introduction The WHO Essential Medicine List for children (EMLc) is used for promoting access to medicines. The age-appropriateness of enteral (oral and rectal) formulations for children depend on their adaptability/flexibility to allow age-related or weight-related doses to be administered/prescribed and the child’s ability to swallow, as appropriate. There is scant information on the age-appropriateness of essential enteral medicines for children.
Objective To evaluate the age-appropriateness of enteral essential medicines.
Materials and methods Age-appropriateness of all enteral formulations indicated and recommended in the EMLc 3rd to 7th (2011–2019) editions were determined by assessing swallowability and/or dose adaptability for children under 12 years, stratified into five age groups.
Results Enteral formulations in the EMLc were more age-appropriate for older children aged 6–11 years than for younger children. In the 3rd edition, for older children, 77%, n=342, of formulations were age-appropriate. For younger children, age-appropriateness decreased with age group: 34% in those aged 3–5 years, 30% in those aged 1–2 years, 22% among those aged 28 days to 11 months and 15% in those aged 0–27 days. Overall, similar proportions were found for the 7th edition. In contrast, the majority of medicines in the 7th list were age-appropriate in targeted diseases like HIV and tuberculosis.
Conclusion Most recommended enteral essential medicines in EMLc 2011 and 2019 were not age-appropriate for children <6 years. Medicines which are not age-appropriate must be manipulated before administration, leading to potential issues of safety and efficacy. Evaluation of the age-appropriateness of formulations for medicines to be included in EMLc could improve access to better medicines for children in the future.
- health services research
- pharmacology
Data availability statement
Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. Data available as supplementary material on request.
Statistics from Altmetric.com
What is already known on this topic?
Children are an heterogenous patient group and formulating medicines for such a heterogenous group is challenging.
The WHO Essential Medicines List for children (EMLc) is aimed at promoting access to medicines for children.
What this study adds?
This study provides a protocol for assessing age-appropriateness of included enteral medicines for children in the EMLc.
It shows for the first time, the age-appropriateness of essential medicines for enteral use included in the EMLc.
The tool it developed can aid the rapid assessment of formulations intended for inclusion in subsequent editions of the EMLc to further promote access.
Introduction
The WHO Essential Medicines List for children (EMLc) guides the rational selection and use of medicines in children aged 0–12 years.1 Essential medicines can be defined as medicines necessary to prevent, treat or manage the most prevalent diseases in a population.2 Essential medicines are divided into two groups: a ‘core’ list meeting needs for a basic healthcare system and a ‘complementary’ list requiring specialist medical facilities, or are more expensive.3 Now in its seventh edition, 2019, the EMLc was first produced in 2007 and is reviewed biennially.4 As a complementary resource to the EMLc, the WHO Model Formulary for children (MFc) was published in 2010 to provide dosing information for the medicines listed in the EMLc, second edition, 2009.5 For most low-income and middle-income countries, the EMLc serves as a template for national formularies, and informs decisions to improve access to medicines for children. In addition, the EMLc supports the Sustainable Development Goals targets for health for women and children.6
However, children are a heterogeneous group with differing abilities to use or administer medicines.7–9 For instance, young children aged under 5 years are generally not capable of safely swallowing conventional solid oral formulations such as tablets and capsules intact. Children can be stratified, based on physiological and developmental milestones, into six age groups: (i) preterm new-born infants, born at under 37 weeks of gestation, (ii) term new-born infants of 0–27 days old, (iii) infants and toddlers, 28 days to 23 months old, (iv) preschool children aged 2–5 years, (v) school children aged 6–11 years and (vi) adolescents aged 12–16/18 years.10 The inherently different abilities of these age groups require that medicines/formulations for children be matched to development (commonly said to be ‘age-appropriate’). If a formulation must be manipulated or handled to obtain the required dose, or to make it easier to administer, there are implications for safety and efficacy.
An age-appropriate medicine has been defined as ‘a medicine whose pharmaceutical design makes it suitable for use in the target age group(s)’.11 The pharmaceutical design (formulation development process) covers aspects such as safety of excipients, patient acceptability and dose adaptability (can deliver variable doses according to body-weight bands; matching to capability or ability).12
Arguably, the primary considerations for inclusion of medicines in the EMLc are disease prevalence, efficacy, safety and cost-effectiveness, with the formulation itself being of secondary consideration. However, recognising that formulations for children have not always been age-appropriate, in 2008 WHO proposed that medicines for children should be made as flexible solid oral dosage (FSOD) forms such as the dispersible tablet. FSODs are formulations that can be given ‘…to patients in more than one manner, for example, may be dispersed (in liquids such as water or breast milk) or taken orally as a whole’.13 FSODs are considered suitable for young children, especially in low-income and middle-income countries, both from a technical (manufacturing, stability and cost) and clinical (ease of swallowing and dosing) perspective. This proposal to produce medicines for young children as FSODs instead of liquids represents a paradigm shift in the development of medicines for children.
Matched by developments in regulations, age-appropriate formulations for children are now recognised as a priority unmet need.14 All formulations included in the EMLc should be assessed for age-appropriateness. If age-appropriate formulations are not available, such assessment can be a guide to development of new products or alternate administration strategies (eg, crushing of tablets and mixing with food) can be recommended, ideally supported with evidence from studies, for the use of existing formulations. This assessment, combined with knowledge of which formulations are commercially available for the various age groups, would help support decisions and strategies intended to improve access to essential medicines.15
The aim of this study, therefore, was to provide a framework for the age-appropriate assessment of enteral (oral and rectal) formulations included in the EMLc. It performed an assessment of the age-appropriateness of all enteral formulations included in the EMLc 2011–2019.16
Methods
A protocol for age-appropriate evaluation was developed. For this evaluation, an age-appropriate formulation was defined as ‘a formulation for which a child of a specified age/age group would have the natural ability to use (either directly or indirectly via a carer), without the product having to be altered from its original or intended presentation prior to administration’. ‘Intended presentation’ referred to all modes by which a solid oral product can be administered as stated on the summary of product characteristics (SmPC); for example, administered whole, crushed, sprinkled or dispersed in a liquid or food before administration.17 If the SmPC did not mention these manipulations, it was assumed that the formulation must be swallowed intact.
The age-appropriateness of all medicines administered by the enteral route listed in the EMLc 2011 to 2019 were evaluated in terms of swallowability of formulation (ability to be swallowed by all in the age groups for which the oral medicine is indicated) and/or dose adaptability (suitability of the recommended formulation strength to deliver the dose recommendations as stated in the MFc).18
The evaluation for age-appropriateness of each recommended enteral medicine in each of the five age groups for children under 12 years (table 1), if indicated, was independently performed by two pharmacists (ESFO and JD) using the protocol. A rank system of 0–3 was used. Active pharmaceutical ingredients (APIs) with no indication, or if contraindicated in any age group, were excluded from the analysis and ranked 0. Outcome results were compared, and any disagreement regarding the outcome was referred to two senior pharmacists (CT and AN) for expert opinion in age-appropriate assessment classification.
Paediatric age groups and body weights used for assessing dose adaptability*
Inclusion and exclusion criteria
All variations on the formulations and strength(s) of the recommended enteral medicines were included in the analysis from the core and complementary sections of EMLc. For any APIs listed in multiple sections of the EMLc, the API and its formulations were only included and assessed once.
Medicines administered by routes other than enteral, and enteral medicines for which no dose information was found in the MFc or, secondarily, in the British National Formulary for Children (BNFc), were excluded.
Swallowability and dose adaptability criteria
In assessing swallowability, certain criteria were assumed to gain consistency in assessment (table 2). Codes were assigned for age-appropriateness of each product: (1) not age-appropriate, (2) may be age-appropriate (where the product may be suitable for only part of the age group or at certain dose levels) and (3) age-appropriate.
Assumptions for assessing swallowability of formulations listed in the EMLc 2011–2019, for children under 5 years of age
Dose adaptability assessment was performed by comparing the recommended doses in mg/kg body weight or mg/m2 body surface area for each essential medicine (as given in the MFc or secondarily in the current edition of the BNFc19 20) to the body weights or body surface areas for each age group as given in BNFc (table 1). Dose rounding (0%–15%) was employed for all APIs except those with a narrow therapeutic index to see if they would match the formulation strength listed in the EMLc. Where the strength of the recommended medicine in the EMLc was found to be either too high or too low to deliver the dose indicated in the MFc (adjusted by rounding), the medicine was classified as not age-appropriate (1). Medicines that could be delivered by the formulation were judged age-appropriate (3). Products that did not fit into these two categories were classified as ‘may be age-appropriate’ (2).
To be evaluated as age-appropriate, both criteria of swallowability and/or dose adaptability had to be met, as applicable for solids or liquids. Oral liquids and rectal products were evaluated only on the basis of ‘dosability’ (the ability of the formulation to accurately deliver the ‘required’ dose that would need to be prescribed).
Data analysis
The percentage of formulations considered age-appropriate was calculated for each age group. Results were further analysed to identify a combination of formulations that would make an API appropriate for all age groups; the number of APIs for which a single formulation could be appropriate for all age groups for which it is indicated; and the number of APIs considered to have no formulation appropriate for any age group. Changes in the percentages of formulations considered age-appropriate between EMLc publications 2011 and 2019 were identified.
Results
There was agreement for majority, 74%, of the evaluations by the two pharmacists using the protocol independently with 26% referred to senior investigators to better understand the medicines, the way in which they would be used and opportunities for dose rounding. Final agreement on all assessments was reached.
For EMLc 2011, there were 1710 separate evaluations, while for the EMLc 2019, there were 2095 evaluations. Examples of the way in which decisions were reached (for amoxicillin and isoniazid) are shown in table 3.
Annotated examples illustrating assessment decisions
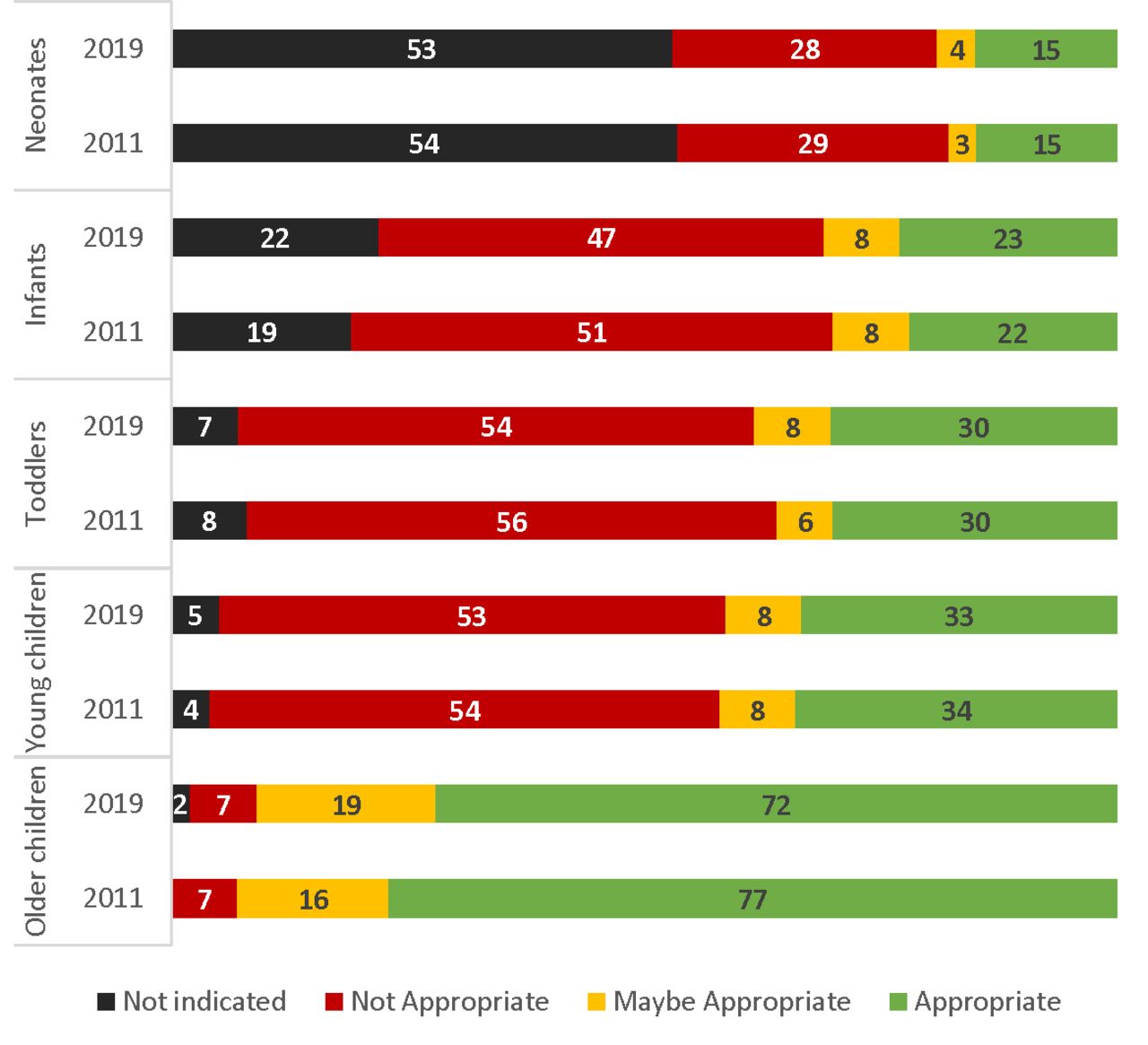
Most (77%, EMLc 2011; 72% EMLc 2019) of the formulations were evaluated as age-appropriate for older children (≥6 years); but not for younger children (<6 years), with <35% age-appropriate in any age subgroup (figure 1).
{kind=link}
The age-appropriateness (%) of enteric medicines included in the Essential Medicine List for children, 2011 and 2019 for each of five age groups in children <12 years old (figure created by the authors/ESFO. Permission to reuse this image is affirmed by the authors).
Slightly over half (55%) of the APIs in the EMLc 2011, the reference, were in a combination of formulations appropriate for all age groups, for example, a liquid for younger children and tablets for older children. About half (47%, 67/143) of the APIs had at least one formulation (usually an oral liquid) that was considered age-appropriate across all age groups for which the API was indicated (table 4 illustrates examples in the EMLc 2019). In practice, though, the whole range of formulations of an API are not readily commercially available and attempts to use tablets when not considered age-appropriate may be made.21 22
Aggregate age-appropriateness for APIs of: (A) antituberculosis medicines, (B) antiretrovirals and (C) Access, Watch, and Reserve (AWARE) classification of antibiotics in the EMLc 2019
Only two preparations were considered to be inappropriate for all of the age groups: phytomenadione tablets (only oral indication in MFc is for neonates) and calcium folinate tablets (no dose in MFc, and BNFc doses do not correspond to tablet strength), in the EMLc 2011; and phytomenadione and vancomycin in 2019.
Overall, changes in proportions between 2011 and 2019 were negligible. However, there were significant changes in formulations deemed age-appropriate with anti-infective agents for HIV and tuberculosis, with seven and eight new/additional FSODs, respectively, in the EMLc 2019.
Discussion
Medicines that are not age-appropriate and, therefore, not immediately acceptable to children must be manipulated before administration (eg, tablets split or crushed) to facilitate swallowing or to deliver the calculated required dose. The evidence for efficacy and safety of such manipulations is limited.23 24 Alternatively, medicines may be prepared extemporaneously by a pharmacist (from API and other excipients, or by crushing tablets and adding a liquid suspending agent). Medicines prepared by extemporaneous dispensing are of variable quality and guidance has recently been issued to improve quality and safety.25 Therefore, wherever possible, medicines in the EMLc should be available in age-appropriate formulations. Information could be provided on the way in which a dose can be safely and effectively delivered if an age-appropriate formulation is not available in the list or locally.
The commercial availability of medicines plays an important part in determining access. EMLc may list appropriate formulations but they may not be commercially available. For example, only 33% of the EMLc 2011 medicines were available in Nigeria as suitable formulations (liquids and FSODs), significantly lower than the 52%–57% for France, Germany, Switzerland, the UK or the USA; indicating the need for more age-appropriate formulations of medicines for children to be made available as one strategy to reduce under-5 mortality.14 26 Medicines for which no suitable formulations exist anywhere can be prioritised for development as FSODs for young children. It would be preferable for the EMLc to clearly indicate when age-appropriate formulations are generally commercially available or when they should be developed.
The EMLc 2019 evidences increases in age-appropriate forms, especially scored, dispersible tablets which have many of the ideal features of a formulation suited to low-income and middle-income countries and as promoted by WHO. These include fixed-dose combination (FDC) antiretrovirals for HIV and FDC antimicrobials for treatment of tuberculosis, both priority conditions with need for formulations approaching the ideal.27 All applications for inclusion in future editions of EMLc could provide sufficient information on dose in relation to age or weight and on the availability of different formulations and strengths to allow an assessment of age-appropriateness.
Evolution is occurring in the field of formulation design and swallowability in young children. For instance, mini-tablets (intact solid oral formulations<4 mm in diameter) have been shown to be acceptable to children as young as 6 months28–30 and even for neonates.31 Dose adjustability can be obtained if the smallest strength of the mini-tablet available corresponds to the usual dose for a young child, allowing several mini-tablets to be taken to achieve the required dose for older children, where necessary. This might thus be a useful modality in drug administration to young children, in addition to the dispersible tablet, providing adequate packaging of administration device.
Standardised methods for assessing age-appropriateness of paediatric formulations are still lacking. When assessing a large list of preparations, certain assumptions must be made about what the ‘average’ child will be capable of; in this work we assumed that children from 6 years of age can swallow conventional sized tablets (≥8 mm) and capsules. Greater sophistication can be added to our simple protocol by introducing tablet size as a criterion for swallowability as the body of evidence is growing; and in terms of overall acceptability, introducing factors such as the safety of excipients (the chemicals added to the API in a formulation to improve qualities such as taste, stability, ease of manufacture) should also be considered, particularly for oral liquids. The current assessment does not include overall acceptability including other formulation qualities such as palatability, stability and portability.32 With excipient safety, particularly important in neonates and infants, the STEP database can provide guidance for selection.33 More tools are becoming available.34–37 This simple protocol, which importantly takes into account the way in which recommended doses are matched to formulation strength (dosability), can be used as a method for rapidly assessing the age-appropriateness of new formulations with an indication for use in children when information is sparse. If there must be a choice between formulations to be available, then the assessment readily shows the implications for certain age groups and warns that alternative administration strategies may have to be investigated and promoted.
As not all considerations that contribute to age-appropriateness were assessed, the proportion of medicines found to be age-appropriate in this study might be overstated. Also, the exclusion of medicines (2%, 7/349, 2011; 12%, 52/419) lacking dose information in the MFc and BNFc, without consideration of other sources of dose information, may have affected the evaluation.
Conclusions
The EMLc does not always list formulations which can be considered age-appropriate at recommended doses noted in the MFc (and BNFc) for all indicated age groups. Using a simple tool, preparations can be classified for age-appropriateness to guide assessment for inclusion in EMLc and local formularies. There is evidence that preparations in the EMLc 2019 are generally age-appropriate in targeted diseases such as HIV and tuberculosis. EMLc could be improved if some indication of age-appropriateness was given and, when preparations are not age-appropriate, how they may be manipulated to improve swallowability and/or dose adaptability.
Data availability statement
Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. Data available as supplementary material on request.
Ethics statements
Patient consent for publication
Acknowledgments
The Niger Delta Development Commission (NDDC) is also gratefully acknowledged for funding this work.
References
Footnotes
ESFO and JD are joint first authors.
ESFO and JD contributed equally.
Contributors All authors contributed equally to this paper.
Funding The research leading to these results received funding from the European Union Seventh Framework Programme FP7/2007-2013 under grant agreement no. 261 060 as part of The Global Research in Paediatrics (GRiP) network.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.