Article Text

Abstract
Objective Anaphylaxis is a severe, potentially fatal allergic reaction best treated with intramuscular epinephrine via epinephrine auto-injectors (AAIs). Our published concerns over laceration injuries to young children associated with AAIs led to this service evaluation of the two administration methods: swing and jab (S&J) and place and press (P&P), to determine potential laceration risk.
Design A trainer EpiPen was used with facepaint placed in the needle indentation which would record the length of movement of the AAI. The two different methods ‘administered’ were alternated. Children were asked to move their leg to simulate a withdrawal reaction. Age, whether they moved, and length of paint mark were recorded.
Setting Outpatients waiting area in Noah’s Ark Children’s Hospital, Cardiff.
Participants Children aged 5–11 with no prior knowledge of AAI use.
Intervention No intervention was implemented.
Results 135 children (mean age 8 years; range 5–11 years) were asked to participate; measurements were taken from 100 children. 50 children moved for one or both methods. For those that moved, S&J mean paint length=8.3 mm (SD 17.4, 95% CI 3.4 to 13.3), P&P mean=3.5 mm (SD 11.0, 95% CI 0.4 to 6.6). Mean difference between methods was 4.8 mm (SD 10.1, 95% CI 1.9 to 7.7). Slightly more children moved for S&J (44) compared with 38 for P&P.
Conclusions S&J produces more movement and longer paint marks than P&P. The risk of laceration when administering an EpiPen to young children may be lower by using the more controlled P&P. We feel it is advisable to teach P&P instead in children below 11 years of age.
- allergy
- injury prevention
Statistics from Altmetric.com
What is already known on this topic?
Epinephrine auto-injectors can be administered using the swing and jab method or place and press method.
Significant lacerations can be caused in children from using epinephrine auto-injectors.
Swing and jab technique may be more likely to cause lacerations due to generating excess activation force with increased pain and movement of the child.
What this study adds?
Children are more likely to move and have longer paint-mark lengths representing higher laceration risk with the swing and jab technique.
There is a risk of laceration with both methods but place and press offers a lower risk with a smaller laceration length.
We feel it is advisable to routinely advise the place and press method for children under 11 years.
Introduction
Anaphylaxis is a severe, potentially fatal, systemic allergic reaction that occurs suddenly after contact with an allergen.1 In children, these are normally precipitated by foods, particularly peanuts, tree nuts, fish and milk. Other antigens may also cause it including latex, insect venom and drugs. In the UK, the rate of hospital admissions for anaphylaxis increased between 1992 and 2012 by 615% from 1.0 to 7.0 cases per 100 000 per year.2 Thankfully, fatality is rare at 1–5.5 per million population of all ages.3 The recommended treatment for anaphylaxis is intramuscular epinephrine, usually in the form of an auto-injector3; EpiPen, Emerade and Jext are commercially available in the UK.4 The two main recognised methods of administering epinephrine auto-injectors (AAIs)5 are swing and jab, which is the recommended method by EpiPen,6 and place and press, recommended by Jext7 and Emerade.8 In Australasia,9 allergists in the Australasian Society for Clinical Immunology and Allergy recommend the place and press method for EpiPen. The British Society for Allergy and Clinical Immunology now encourages the place and press method in their updated 2019 Paediatric Allergy Action Plans for all three types of AAIs: EpiPen, Jext and Emerade.10–12 Inadvertent harm can come from administering these devices including severe lacerations and subsequent scarring.13 14 All children recorded with lacerations in the literature we have reviewed were under 11 years of age (ie, primary school-age children).13 14 We routinely train families in the use of EpiPens: both by the licensed swing and jab approach and also the alternative place and press method. Concerns over the potential risk of laceration led to the development of this service evaluation completed in May 2017 to identify if one method of administering AAIs is more likely to cause lacerations than the other. Our aim was to evaluate the potential risk of laceration after standard training in using the two methods of administering an AAI in children (swing and jab and place and press).
Method
We evaluated the risk of laceration by using a trainer EpiPen to measure the potential distance an AAI moves using each method. A trainer EpiPen was used so no actual needles or injections were involved. Initially paints, ink pads and felt tips were trialled in order to find a material which would give accurate results when measuring the EpiPen’s lateral movement across the skin, which would not smudge and would leave a mark at least 90 mm long (the largest laceration length seen in publications13 14). Water-based paint from a squeezable tube was found to fulfil these criteria and was also easy to set up and clean away. The paint was placed in the centre of the trainer pen where the needle would be in a real AAI, all excess paint around the ‘needle’ indentation was removed by scraping, leaving it flush with the orange base of the trainer pen.
Families with children aged 5–11 years were asked to take part when attending routine outpatient appointments; they did not need to have an allergy in order to participate. The process was explained and agreement to participate obtained. We excluded those with any prior knowledge of auto-injector use to reduce bias. The two methods of administration were used in each child sequentially, with the first method alternating between each child. The child’s age was recorded, plus the administering method and whether swing and jab or place and press was the first or second method tried. When the trainer pen clicked, which indicates the AAI firing in a real-life situation, the child was asked to pretend they felt a pinch/sting and move their leg accordingly. The pen was used on the lateral outer thigh on bare skin. Whether the child moved for each method was recorded. The length of each paint mark was measured in mm by a micrometre (Katsu Electronic Digital Caliper) to the nearest ±0.1 mm.
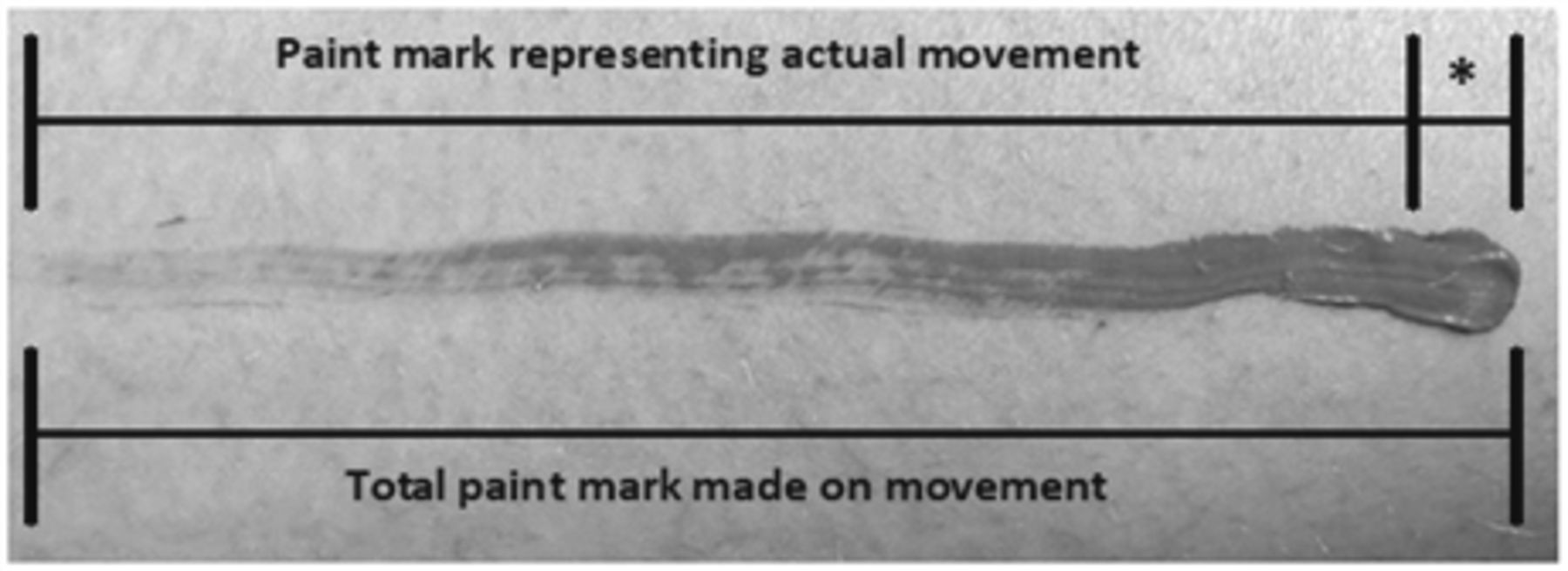
Prior to commencement, an average measurement of the mark size made by the paint simply applying the EpiPen to the thigh was recorded in an adult (LP) to represent no movement. This mean was done as a non-method specific control to be used for both place and press and swing and jab data. Both methods were administered three times with the participant not moving. The mean of these ‘no-movement’ readings was 3.2 mm and represents the size of the ‘paint needle’ itself. This no-movement ‘length’ was subtracted from all measurements taken to leave the ‘actual movement’ of the AAI (figure 1). This was deemed to represent the distance a possible laceration injury could occur over. Analysis was by paired samples T-test using IBM SPSS Statistics V.23.

Explanation of the calculation of the actual mark made by movement of the epinephrine auto-injector (AAI) shown by paint mark, with the mean of ‘no movement’ represented by asterisk (*). Mean of ‘no movement’ is subtracted from the total paint mark to leave the actual distance the adrenaline auto-injector moves, that is, the laceration length.
Results
We asked the families of 135 children between 5 and 11 years of age (mean age 8 years) to take part. Measurements were taken from 100 children, 10 agreed to take part but were called away before measurements could be taken and 25 declined.
Fifty children (50%) did not move when the EpiPen was administered. Thirty-two children (32%) moved for both methods, 18 children (18%) moved for only one method; 12 children for swing and jab and 6 children while place and press was administered. In total, there were no significant differences for movement using swing and jab (44 children) recorded compared with 38 children for place and press (p=0.47).
For all 100 children, regardless of movement, the mean measurement for swing and jab was 4.6 mm (SD 12.9; 95% CI 2.1 to 7.2), and 2.1 mm for place and press (SD 8.0; 95% CI 0.6 to 3.7). On comparing measurements for the two methods, when paired according to each participant, a mean difference of 2.5 mm (SD 7.6, 95% CI 1.0 to 4.0) was found by paired samples T-test (p=0.001).
For the children who moved for either one or both methods, swing and jab had a mean measurement of 8.3 mm (SD 17.4, 95% CI 3.4 to 13.3), whereas place and press had a mean measurement of 3.5 mm (SD 11.0, 95% CI 0.4 to 6.6). By comparing paired measurements for those children that moved, the mean difference was 4.8 mm (SD 10.1, 95% CI 1.9 to 7.7) using paired samples T-test (p=0.001).
For the children who did not move for either method there was no significant difference between the paired measurements (p=0.402; mean (SD) swing and jab=1.0 mm (1.6), mean (SD) place and press=0.8 mm (1.5)).
The largest recorded measurement for swing and jab was 102.1 mm compared with 76.9 mm place and press. Figure 2 compares results of both methods for children who moved and children who did not move. Table 1 details means and SD for both methods of administration according to movement and age strata. Numerical data for figures 1 and 2 can be found in the online supplementary file.
Supplemental material

{kind=link}
{kind=link}
(A) Movement of epinephrine auto-injector (AAI) made by children who moved for one or both methods (n=50). (B) Movement of AAI made by children who did not move for either method (n=50).
Mean (SD) results presented for swing and jab and place and press data by age strata and whether the child moved
Discussion
EpiPen is the only AAI that recommends the swing and jab method1 in the UK. Generally, primary school-age children are unlikely to be able to administer an AAI to themselves, and so a caregiver (eg, parent) will usually administer it. After the age of 11, when the child attends secondary school, they are expected to be able to manage injecting themselves. All children recorded with lacerations in the literature were under 11 years. Under-fives were not deemed able to participate in the service evaluation due to concerns about their comprehension. A child aged 5–11 years may worry about being injected with an AAI and so may be at greater risk of moving their leg in an understandable response. Thus, our evaluation focused on children aged 5–11 years.
Without actually firing the pens into a child, which would be unethical, any simulation is subject to various limitations. The method of asking a child to move when they hear the AAI click is not perfect as can be seen by our results; 50% of children did not move when asked. However, this practical method was the most ethical way of evaluating EpiPen laceration risk without using real AAIs and involving needles.
Literature on this topic is scarce, with only two retrospective case history/series that observe lacerations using AAIs.13 14 All cases were in young children, many with severe long lacerations. We recently raised concerns suggesting that swing and jab is more likely to cause lacerations due to both the adult moving and the potential for the child to move, as well as generating ‘excess activation force […] increased pain and movement of the child’.13 Our current evaluation found that swing and jab leaves a much longer paint mark than place and press overall for all children. For those who moved the difference in length size was even more marked when the swing and jab method was used. There was no statistical difference in the methods for those children who did not move.
No significant difference was found in numbers of children who moved when swing and jab was used (44) compared with place and press (38) (p=0.47). In those who moved there was a significantly longer mean length of mark left by swing and jab (8.3 mm) than place and press (3.5 mm; p=0.001). Half of the children who took part did not move when they heard the click signifying the trainer AAI firing and in real life use, the needle being inserted. This may be due to children either not understanding they needed to move, especially younger participants, or not feeling that they would have moved in that situation anyway. The results showed that in these children who did not move for both methods there was no significant difference between swing and jab and place and press movements. This, as one would expect, suggests that if the child does not move then they are less likely to suffer a laceration with whichever method is administered.
Although a mean measurement was made of ‘no movement’, actual results showed a wide variation in measurements for both methods when children did not move (2.3–9.4 mm) during data collection. These were most likely due to paint smudging or slight movements by the participant or data collector causing the EpiPen to move. Occasionally, air bubbles were caught in the needle indentation with the paint which could account for smaller measurements than expected and therefore giving a negative value once the mean ‘no movement’ measurement has been subtracted.
Overall, this evaluation has shown a significantly longer length of paint-mark made by the swing and jab rather than the place and press method. This is most marked when the child moves, something that happened slightly more often for the swing and jab method. The place and press method produced shorter paint-mark lengths, probably reflecting a lower risk of laceration in young children. Previous cases13 14 have shown that there is a risk of laceration when administering an EpiPen to children using the recommended swing and jab method. Thus, immobilisation of the child’s leg should be used whichever method is preferred. However, we feel it is advisable to change practice to teaching the place and press method for young children under 11 years of age to families instead of the currently recommended swing and jab technique. This change should reduce laceration injury risk in primary school-age children.
Acknowledgments
The authors would like to thank the Children’s Hospital for Wales REACH allergy team for their encouragement of this student project. The authors would also like to thank the families and children for their help in this patient safety work.
Footnotes
Contributors DT derived the original idea of evaluating the two different methods after noticing and publishing a case history on a young child who had suffered a laceration from the swing and jab method. LP came up with the method of measuring laceration length, collected and then analysed the data. Both authors have had input in writing the original paper.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This service user evaluation was approved as a student project by Cardiff University. Ethical approval was not required as this was a non-randomised service evaluation to improve safety of the outcome of our two routine training methods for administering an epinephrine auto-injector.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information. All deidentified participant data are available in an online supplementary file. Please contact the author(s) for permission to reuse data from this publication: david.tuthill@wales.nhs.uk.