Article Text

Abstract
Objective To compare early motor and language development of children <3 years of age growing up in high-income and low-income contexts.
Design Cross-sectional study.
Setting We analysed differences in motor and language skills across study sites in Cambodia, Chile, Ghana, Guatemala, Lebanon, Pakistan, the Philippines and the USA.
Main outcome measure Cognitive and language development assessed with the Caregiver Reported Early Development Instruments (CREDI) tool.
Results 4649 children aged 0–35 months (mean age=18 months) were analysed. On average, children in sites with a low Human Development Index (HDI) had 0.54 SD (95% CI –0.63 to –0.44) lower CREDI motor scores and 0.73 SD (95% CI –0.82 to –0.64) lower language scores than children growing up in high HDI sites. On average, each unit increase in national log income per capita was associated with a 0.77-month (95% CI –0.93 to 0.60) reduction in the age of motor milestone attainment and a reduction in the age of language milestone attainment of 0.55 months (95% CI –0.79 to –0.30). These observed developmental differences were not universal: no developmental differences across sites with highly heterogeneous socioeconomic contexts were found among children growing up in households with highly educated caregivers providing stimulating early environments.
Conclusion Developmental gaps in settings with low HDI are substantial on average, but appear to be largely attributable to differences in family-level socioeconomic status and caregiving practices. Programmes targeting the most vulnerable subpopulations will be essential to reduce early life disparities and improve long-run outcomes.
- neurodevelopment
- child psychology
- epidemiology
Statistics from Altmetric.com
What is already known on this topic?
Recent studies conducted among healthy children suggest small differences in milestone achievement across countries.
Strong within-country socioeconomic gradients in children’s skill development have been documented in most high-income settings.
Comparable data on child development are rare across countries.
What this study adds?
We show substantial gaps in average development between high-income and low-income country sites using a standardised tool.
We also show that these differences are primarily due to differences in caregiver education and home environment.
We found no developmental differences across highly diverse sites for children growing up in similarly supportive homes.
Introduction
A large body of research has emphasised children’s development within the first several years of life as foundational to individual and societal success.1–3 Early language and motor development, in particular, are widely studied as mechanisms that support children’s ability to explore, interact with and learn from the world around them. Empirically, early language and motor abilities have been linked with a number of later-life outcomes, including linguistic and cognitive performance in middle childhood and schooling attainment in adulthood.4–6
Even though behavioural, cultural and environmental factors such as child care practices and parental well-being may be more important for early development than mere resource availability,7 8 research from both high-income and low-income countries has demonstrated that exposure to household poverty can compromise young children’s developmental progression. Compared with children growing up in households of higher socioeconomic status, language and motor development of children from relatively disadvantaged households in the same countries appears to be frequently delayed.9 10 Given the high poverty exposure of children from low-income and middle-income countries (LMICs),1 11 it is generally assumed that children from LMICs develop more slowly than their peers from more advantaged nations in the first years of their life, and that these early developmental deficits have large individual and societal costs in the long run.2 3 12
The presumed negative relationship between country income and early childhood development (ECD) is contrasted by a large body of work from cross-cultural psychology documenting that children from sub-Saharan Africa and other low-income country settings develop specific basic motor skills substantially earlier than children in high-income settings.13–17 This cross-cultural evidence suggests that early development may be less vulnerable to poverty and local environmental conditions than what has been documented for early life physical growth, and that other behavioural, cultural and environmental factors such as child care practices and resource access may be more important for early development than local income levels.18
A recent study assessing samples of healthy, hospital-born children in four middle-income countries found remarkably small differences in the age at which children attained early motor and language milestones.19 Results from the International Fetal and Newborn Growth Consortium for the 21st Century (INTERGROWTH) study also suggest rather minor differences in the development of healthy children in high-income, middle-income and low-income countries in the first 2 years of life.20 This is contrasted by UNICEF’s Early Child Development Index global database, which suggests rather large variation in basic skills among children aged 3 and 4 years in LMICs.21 22
In this paper, we use data on ECD for children from birth to 3 years collected across highly diverse sites using the internationally validated Caregiver Reported Early Development Instruments (CREDI) to assess the extent to which 1) country-level economic development predicts early motor and language development overall, and 2) these associations vary across particular milestones and subpopulations characterised by different home environments.
Methods
Study design
This study was designed as a cross-sectional observational study, comparing children’s development across eight highly diverse country sites. All data were collected as part of a larger effort to establish new measurement tools (CREDI) for children under the age of 3 years globally.23 24
Setting
Data were collected in Cambodia, Chile, Ghana, Guatemala, Lebanon, Pakistan, the Philippines and the USA. These country-specific sites were identified based on locally available research partners able to collect data on early childhood milestones. Estimated income per capita across the countries from which children were sampled ranged from 3504 purchasing power-adjusted dollars per capita in Cambodia (Human Development Index (HDI) rank 146) to 56 207 dollars in the USA (HDI rank 13). As shown in table 1, study sites in Cambodia, Ghana, Guatemala and Pakistan were mostly rural, while a mix of rural, peri-urban and urban populations were surveyed in Lebanon, the Philippines and the USA. In Chile, all children were recruited from Santiago (urban only).
Site descriptions
Participants
Participant recruitment varied by site. In Cambodia, Chile, Ghana, Guatemala and the Philippines, children had been recruited for ongoing research studies, with additional (typically post-intervention) surveys already planned prior to the launch of the CREDI project. Local research teams interested in ECD measurement simply added age-appropriate CREDI items as an additional module to their own surveys. In the USA, participants were recruited through the Mechanical Turk online platform. In Chile and Lebanon, children were actively recruited for this assessment by study partners. In Pakistan, the questionnaire was administered to younger siblings of 4 years of age participating in a longitudinal study.
Variables
The primary variables of interest were caregiver reports on the completion of children’s early language and motor milestones. Survey questionnaires were translated to local languages by local expert teams and administered to caregivers of children under the age of 3 years. The CREDI contains a total of 109 caregiver-reported items. For the surveys, CREDI items were divided into three age groups according to item difficulty. All specific questions (age 0, 1, 2 years) were administered to caregivers in each site. In addition to the CREDI items, all surveys collected information on child age, caregiver education and caregiver-child interactions. Caregiver-child interactions were measured using the Multiple Indicator Cluster Survey (MICS) home stimulation scale, which asks caregivers whether any adult in the household read to, played with, told stories to, counted with, sang to or travelled outside of the home with the child in the past 3 days. Surveys were conducted orally in all sites except for the USA, where questions were administered online to respondents. Prior evidence comparing CREDI online and in-person scores suggests overall high comparability with both modalities.25
Data sources/measurement
Data on specific milestone completion as well as overall motor and language development were collected using the CREDI. The CREDI was created in 2017 with the ambition to generate a low-cost, cross-culturally comparable measure of the motor, cognitive, language and socioemotional skills of children under 3 years. The CREDI have been tested and validated in 16 low-income, middle-income and high-income countries and has been shown to have high acceptability, reliability and validity across diverse cultural and socioeconomic settings.23 26
The CREDI contain 109 items, which are scored as 1 if the caregiver reports that the child has achieved the milestone by the time of the interview, and 0 otherwise. The responses to these 109 items were then used to compute overall development scores in the motor, language, cognitive and socioemotional domains.24
Statistical methods
Our analysis was divided into four parts. In a first step, we compared overall motor and language development on the CREDI by age across HDI sites group. The HDI is a composite index of countries’ overall development based on their life expectancy, average educational attainment and per capita income.27 We divided our sample sites in three groups based on their 2017 HDI ranking: high HDI sites (HDI rank ≤60): Chile and the USA; medium HDI sites (HDI rank 60–119): Lebanon and the Philippines and low HDI sites (HDI rank ≥120): Cambodia, Ghana, Guatemala, Pakistan. For this analysis, we normalise total CREDI scores to mean 0 and SD 1 within age group (with monthly age intervals).
In a second step, we focused on four basic and easily observable motor and language milestones that represent major shifts in children’s early skills. For motor skills, we analysed children’s ability to sit independently, to stand without support, to walk without support and to run without falling. The four language milestones analysed were: ability to make basic (babbling) sounds, to say 1 or more words, to say 10 or more words and to speak in sentences of >3 words. For all eight milestones, we first graphed attainment rates by age and site, and then estimated average time (in months) between the domain-specific milestones.
In a third step, we used random-effects meta-analysis to assess the general relationship between the national income per capita at each study site and the median age of milestone achievement observed. For this analysis, we first computed the median age of attainment for all motor and language milestones in each site, and then regressed the estimated site-specific median age on site-specific income per capita. This yielded a total of 39 (motor) and 40 (language) income gradient estimates, respectively. We used forest plots to summarise the estimated median ages by domain, and used random-effects meta-analysis to estimate an average income gradient for the milestones in the motor and language domains.
Lastly, to assess the extent to which developmental gaps at the country income level depend on home environments, we explored more detailed data on home environments collected in a subsample of children across six sites. The main hypothesis we explored was that country-level income primarily affects children’s outcomes through their home environment, so that we should not observe developmental gaps once we focus on children living in similar households. Using the overall motor and language CREDI scores as outcome variables, we thus estimated pooled models in a first step, and then restricted to households with a high number of MICS caregiver-child activities reported (>3) as well as to households with caregivers who completed secondary education or higher in a second step.
All analysis was conducted using the Stata V.14 statistical software package.28
Ethical considerations
All caregivers consented to participate in the surveys.
Results
In total, 4649 children under 3 years of age were assessed. The average age of children assessed was 18 months, and 49.4% of children were female (online supplementary table 1). Table 2 shows average developmental differences across HDI site groups. On average, children in low HDI sites had 0.54 SD (95% CI −0.63 to –0.44) lower motor scores and 0.73 SD (95% CI −0.82 to –0.64) lower language scores than children growing up in high HDI country sites (Chile and the USA). In both domains, larger developmental gaps were found for children >18 months of age than for younger children. Developmental gaps were smaller for medium versus high HDI country sites, with estimated mean differences of 0.50 SD (95% CI −0.61 to –0.39) for motor and 0.49 SD (95% CI −0.59 to –0.38) for language, respectively.
Supplemental material
Developmental differences across HDI groups
Figure 1 displays overall CREDI subscale scores in the motor and language domains in high and low HDI country sites, by age. For both domains, differences were detected from very early on; increases in the gap over time appear larger for motor skills, where the two groups were more similar initially.

Overall motor and language developmental scores by local socioeconomic context. Figure shows smoothed estimates for high and low HDI sites and CREDI motor (left panel) and language (right panel) subscale scores. High HDI sites are Chile and the USA. Low HDI sites are Cambodia, Ghana, Guatemala and Pakistan. Z-scores are computed relative to a global reference sample of caregivers with completed high school or higher education. Details on CREDI subscale score computation are provided in the study by Waldman et al.24 Higher scores indicate more advanced development in the respective domain. CREDI, Caregiver Reported Early Development Instruments; HDI, Human Development Index.
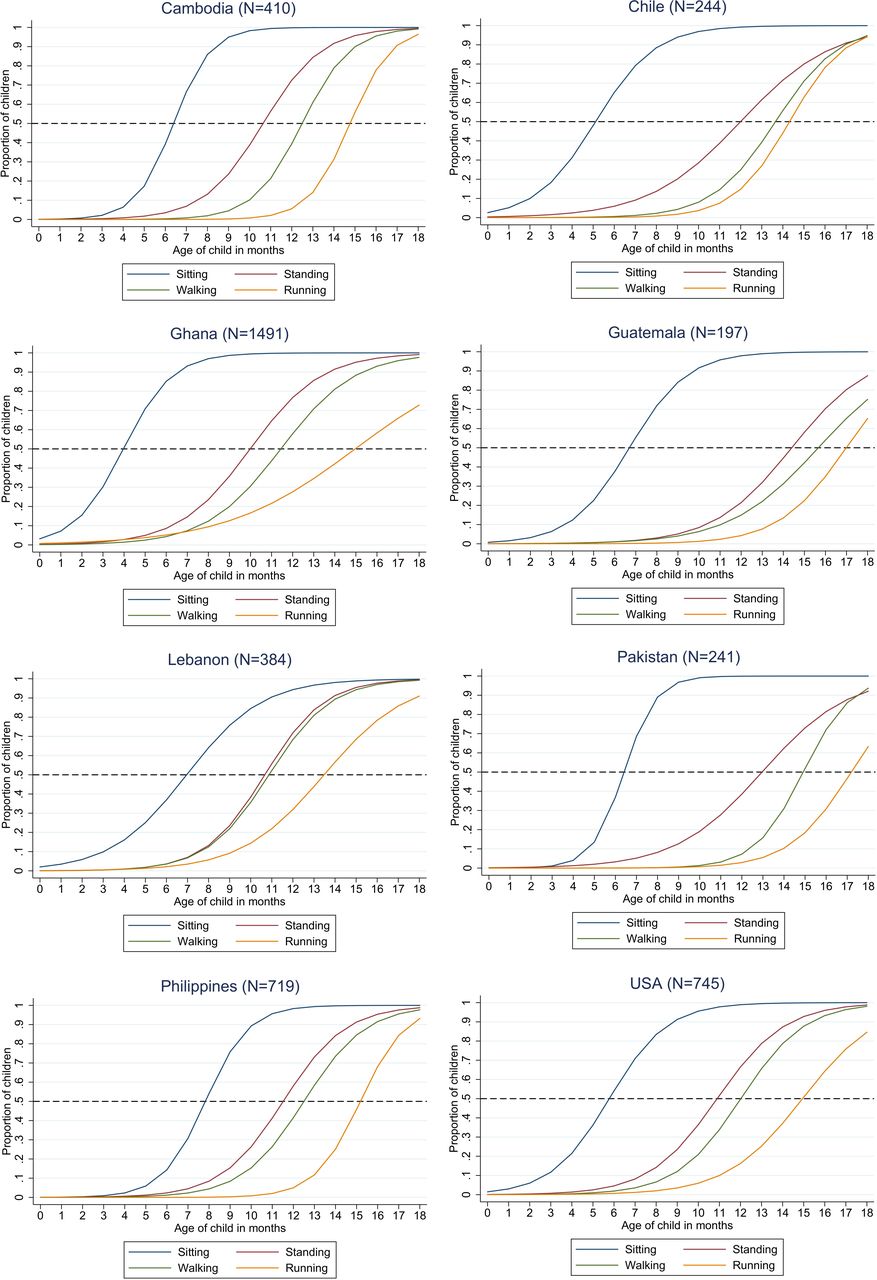
Figure 2 shows site-specific age patterns observed for the four selected motor milestones. For each age, figure 2 shows the proportion of caregivers confirming that the child has reached a given milestone. In the US sample, median milestone attainment ages were 6 (sitting), 11 (standing), 13 (walking) and 15 (running) months, respectively. Age patterns varied substantially across sites: relative to the US sample, children in the Ghanaian site were reported to sit and stand without support significantly earlier, whereas children in the Philippines site acquired these skills significantly later. In terms of motor skills, the largest differentials were found for the age at which children took their first independent steps, with a median age of 11 months in the Lebanon sample compared with a median age of 16 months in the Pakistan and Guatemala sites, respectively (see online supplemental tables 2). Online supplementary table 3 shows the results of quantitative analysis and significance tests.

Basic motor milestones by study site. Data restricted to ages 0–18 months; n=410 for Cambodia, 244 for Chile, 1709 for Ghana, 197 for Guatemala, 384 for Lebanon, 241 for Pakistan, 719 for the Philippines and 745 for the USA.
Figure 2 also highlights the highly heterogeneous transition times between motor milestones. In the US sample, the median lag between independent sitting and standing was 5 months; in the Lebanese and Philippino sites, this transition took on average only 4 months, whereas this transition took 6 months in Ghana and 8 months in Guatemala. As expected, the transition from standing independently to walking was relatively fast in most countries, with a median duration of about 2 months. The transition from walking to running took about 2.5 months on average, but also showed variability across sites (eg, 1 month in Guatemala and Chile vs 3 months in Ghana, Pakistan and the Philippines).
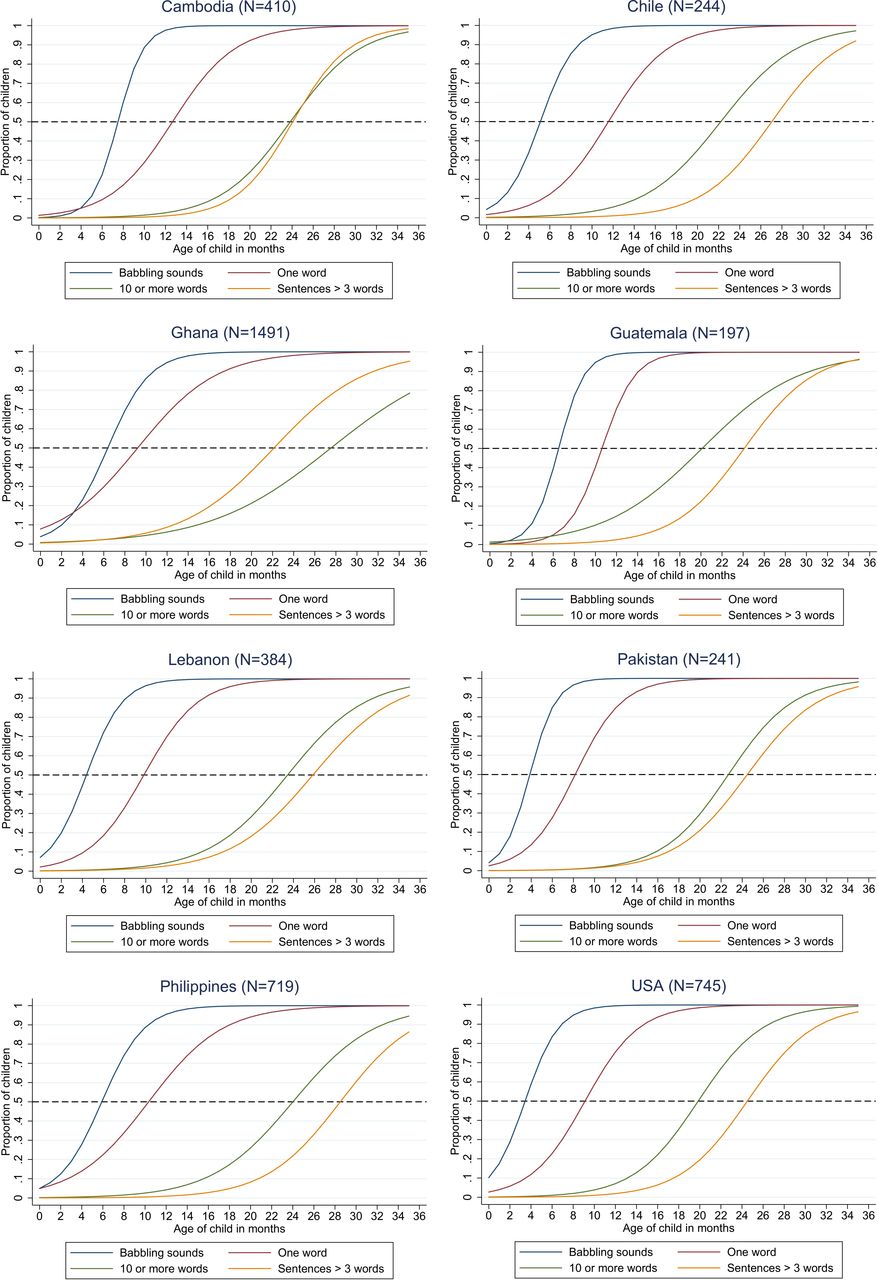
Figure 3 shows the results for the same analysis in the language domain. The age at which caregivers reported first babbling sounds varied widely both within and across sites, with a median age of 7 months overall. The median age for the first word was 10 months in the US, with both Cambodian and Chilean sites reporting substantially later debuts compared with the US site. In the US sample, a vocabulary of 10 or more words was reported at a median age of 20 months, whereas this milestone was reached later in all other sites, with statistically different trajectories in Cambodia, Ghana, Lebanon and the Philippines relative to the USA. See online supplementary tables 4 and 5 for estimation details and results. Differences were somewhat smaller for sentences with more than three words, which on average were reported at 25 months of age.

Language milestones by study site; n=410 for Cambodia, 244 for Chile, 1709 for Ghana, 197 for Guatemala, 384 for Lebanon, 241 for Pakistan, 719 for the Philippines and 745 for the USA.
In terms of transition times between language milestones, the average duration between the first word and a larger vocabulary of 10 or more words was about 12 months, with substantially faster average transitions in Guatemala and the USA (10 months) and substantially slower average transitions in Lebanon (14 months), Pakistan (14 months), the Philippines (14 months) and Ghana (18 months).
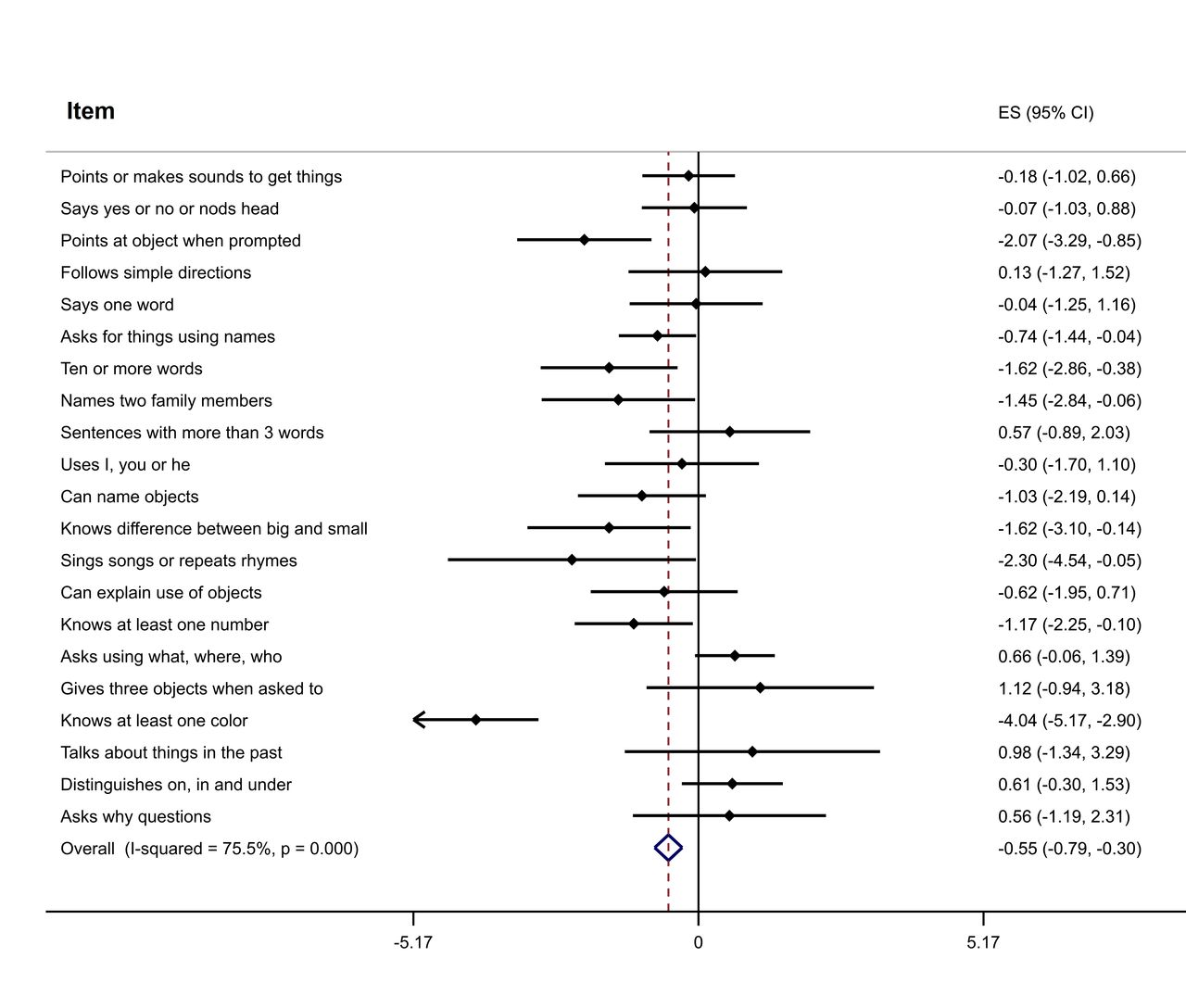
The results of item-specific age-difference regressions are shown in figure 4 (motor) and figure 5 (language). Across all items, the pooled estimate was −0.77 (95% CI −0.93 to 0.60) for motor skills and −0.55 (95% CI −0.79 to –0.30) for language skills, indicating that, on average, each unit increase in country-level log income was associated with achieving motor milestones 2–3 weeks (0.55–0.77 months) earlier. Multiplying this difference with the difference in log income between the wealthiest (the USA) and the poorest country in our sample (Cambodia) yields an average 2.1 months difference in motor milestones, and an average difference of 1.5 months in language milestones between those countries.

Income gradient for individual motor milestones. Figure shows estimates (ES) (with 95% CIs) from linear regression of site-specific median age of skill acquisition on log(national income per capita)–no additional controls are included in this analysis. Milestones ordered from most basic to most advanced. Based on a sample of 4649 children across 8 sites. A negative slope means that, on average, wealthier sites achieve the milestone earlier; since income is measured in logs, a coefficient of −1 implies that a 100% increase in national income per capita is associated with achieving a given milestone 1 month earlier on average.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Income gradient for language milestones. Figure shows estimates (ES) (95% CIs) from linear regression of site-specific median age of skill acquisition on log(national income per capita)–no additional controls are included in this analysis. Milestones ordered from most basic to most advanced milestone. Based on a sample of 4649 children across 8 sites. A negative slope means that, on average, wealthier sites achieve the milestone earlier; since income is measured in logs, a coefficient of −1 implies that a 100% increase in national income per capita is associated with achieving a given milestone 1 month earlier, on average.
Table 3 shows stratified multivariable regression results. Information on maternal education and home stimulation activities was available for a subsample of 2197 children across 6 sites. Out of this subsample, 66% of caregivers reported engaging in at least four out of six home stimulation activities, and 29.5% of caregivers attended some college (<3% in the Cambodian and Pakistan sites, >50% in the USA). In this subsample with full information, each unit increase in country-level log per capita income was associated with a 0.29 SD increase in overall motor development (95% CI 0.098 to 0.489), and a 0.18 SD increase in overall language development (95% CI 0.136 to 0.223). When we restricted analyses to caregivers who reported at least four out of the six home stimulation activities (column 2 and column 5), the estimated associations with country income became smaller, but remained statistically significant. When we restricted to high-stimulation households in which mothers had completed at least a secondary education (column 3 and column 6), developmental differences across country income groups were substantially attenuated and no longer statistically different from zero.
Stratified associations between local income per capita and developmental scores
Discussion
The results presented in this paper have yielded three main findings. First, we find that local socioeconomic context strongly predict average motor and language development of children under the age of 3 years, with children growing up in low HDI settings on average scoring 0.5–0.7 SD lower in the motor and language domains, respectively, than their peers from high HDI sites. This finding is consistent with the large number of children estimated to not reach their developmental potential in the global health literature1 11 21 as well as the literature on children’s physical growth that has extensively documented the continued high burden of growth faltering in LMICs.29–31
However, this average developmental gap does not imply that all population groups growing up in low-resource settings should be expected to have developmental deficits. As two very recent studies have shown, very similar milestone completion can indeed be found among healthy children living in diverse countries.19 20 The second main finding of our paper is well aligned with these studies and suggests that developmental gaps are on average not detectable for children growing up in households with highly educated and engaged caregivers, independent of the economic or human development of their surroundings. Although our sample of children with similarly stimulating home environments is relatively small (n=717), our results suggest that developmental gaps across sites appear to be almost exclusively attributable to the children growing up in less privileged households. Children in these households are likely to experience less stimulation and substantially higher exposure to infectious disease and other health-related risk factors.
We also find that the age at which young children achieve specific motor and language milestones varies widely within sites, and displays large variation across sites. Importantly, when examining this across-site variability more closely, we identify multiple examples where children from more economically disadvantaged sites were reported to demonstrate relatively advanced developmental behaviours. For example, children in Ghana and Lebanon appear to learn to walk before children in high-income settings; similar early advantages in physical skills have been documented in the cross-cultural psychology literature.13–17 Maybe more surprisingly, children in the Pakistani site were reported to say their first words before children in higher HDI sites, and using short sentences was reported slightly earlier in Ghana than in the US sample. Even though this latter difference may to some extent be driven by how sentences are constructed in local languages (primarily Dagbani in the study area), it seems important to highlight that the ages at which children attain individual motor and language milestones are not always linked to the overall economic development of their given setting. The diverging patterns of skill acquisition across settings observed in this paper highlight the likely importance of unmeasured contextual and cultural factors such as child care and parenting practices,32 and can be interpreted as evidence of large developmental potential with sufficient support even in economically disadvantaged environments. The large heterogeneity in the relative timing (and in some cases also sequencing) of specific milestones also highlights the importance of viewing ECD as a complex and multidimensional construct requiring carefully validated tools for valid comparisons within and across countries.
Our analysis has several limitations. First, the data collected do not allow us to directly identify the exact features of children’s home environments that may serve to protect their developmental well-being, as maternal education is likely to be correlated with children’s ECD, and with on average higher household incomes, access to superior child care and better health and nutrition knowledge. All of these factors likely contribute to the empirically observed gaps between children from more versus less advantaged homes globally. Further research is to identify the most critical supports for healthy ECD, and to find the most effective ways to deliver these supports to the children lacking them most. A second limitation of the study is that the data used are not nationally representative. Sites in Ghana and Cambodia were both in particularly poor areas of the country, while children from the USA and Chile were generally from better off neighbourhoods. Children in Cambodia, Guatemala and the Philippines had also previously participated in ECD programmes, and may thus on average have been better developed than other children from these areas. Additionally, rates of survey non-response are not known due to the fact that data collection in most sites occurred through existing research studies. The results presented in this paper should thus not be interpreted as country differences, but rather as differences between sites across a highly diverse range of local environments. Given that nationally representative data on ECD will be urgently needed to track progress on Sustainable Development Goal 4.2, more comprehensive data from the study countries will hopefully become available soon. A third limitation is that the CREDI is—by construction—a caregiver-reported tool, and may introduce bias into children’s developmental scores because caregivers may not be aware of specific milestone completion or may misreport it. Previous validity studies suggest that all CREDI items are well understood by caregivers, and that CREDI scores are highly predictive of direct observation measures of the same children.26 Despite these tests, reporting biases are of course possible, particularly for items that leave room for subjective interpretation such as making babbling sounds or saying the first word.
Overall, the results presented in this study suggest that income-based gaps in motor and language development can be detected rather early in low-income settings. These gaps appear to be primarily attributable to the high prevalence of suboptimal home environments in low-income settings, as children growing up in highly educated and stimulating home environments appear to fare equally well globally. From a programmatic perspective, the results presented in this paper suggest that optimal targeting of ECD programmes will require identifying the populations at highest risk for overall developmental setbacks in each setting, and will also require customising programmes towards the specific developmental needs and strengths of a given sociocultural context.
References
Footnotes
Funding This project was supported by Grand Challenges Canada through the Saving Brains Platform.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Given that no names or other identifiable information were collected from caregivers, this project was designated exempt from review by the (redacted) University’s ethics board (IRB15-3833).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request.