Article Text

Abstract
Objective To describe the incidence and epidemiological characteristics of child pulmonary tuberculosis (PTB) notified to the Chinese Center for Disease Control and Prevention (CDC) Tuberculosis Information Management System (TBIMS) from 2009 to 2015.
Study design A database of child PTB for 31 provinces in mainland China over 7 years was retrospectively analysed. The spatiotemporal distribution of child PTB was described.
Results In total, 35,710 child PTB cases were notified to the TBIMS, representing only 0.60% of all 5,991,593 PTB case notifications. The average annual notified incidence of child PTB was 2.44/ per 100,000 children (95% CI: 1.77–3.10) and decreased by 52.53% in all age groups during the study period. Tibet had the highest incidence (15.95/ per 100,000 children), followed by Guizhou and Xinjiang. However, the case numbers were the most in Guizhou. The 0-1 year and 12–14 years of age groups exhibited the most cases. The positive rates of sputum smears, bacteriology and chest X-rays abnormality were 21.5%, 21.7% and 98.1%, respectively, which were lower than those 15 years of age and older (all p-values<0.0001).
Conclusion The notified incidence of child PTB in mainland China decreased substantially over 7 years. Future prevention and control of PTB in children should focus on the 0–1 and 12–14 years of age groups, and Tibet and Guizhou provinces. However, the notified incidence is still low, relative to adults, suggesting substantial under-reporting. Thus, more effective care seeking, identification and registration of children with TB are crucial.
- notified child pulmonary tuberculosis
- epidemiological characteristics
- incidence
Statistics from Altmetric.com
What is already known on this topic?
There have been few studies of the prevalence of child tuberculosis in China.
What this study adds?
Notified child PTB declined by more than 50% from 2009–2015, which was more rapid than that in the ≥15 year age group (21.16%). The spatial distribution of notified PTB in children was similar to that in the other age groups with a high incidence in western China and a low incidence in eastern China. Tibet had the highest incidence (15.95/ per 100 000 children), followed by Guizhou and Xinjiang.
Introduction
Tuberculosis (TB) is a serious infectious disease that affects children worldwide, especially infants and children aged less than 15 years. According to the latest report issued by the WHO in 2018, children with TB comprise approximately 10% (aged <15 years) of all TB cases, and thus, approximately 1 million new cases of TB emerge in children globally.1 However, the number of reported cases of child TB greatly differed from the number of estimated cases. It has been estimated that almost two-thirds of all children with active TB have not been reported.2 The low reporting rate of child TB is partially due to the low detection rate. Therefore, the prevention and control of TB in children still faces enormous challenges.
In China, the data on the prevalence of TB in children are still from the fourth nationwide random survey of TB reported 19 years ago.3 4 To date, few large-scale epidemiological studies relating to TB in children have been performed in China. The characteristics of TB in children differ from those in adults. The diagnosis of TB in children is more difficult than that in adults because most cases are bacteriologically negative and often have non-specific clinical symptoms and signs.5 6
In 2005, the Chinese Center for Disease Control and Prevention (CDC) developed a web-based Tuberculosis Information Management System (TBIMS) to collect real-time TB data, including on child TB, in 31 provinces in Mainland China.7 However, only the notification of pulmonary TB (PTB) is mandatory under the Chinese Law of Preventing and Controlling Infectious Disease. Based on these data, we reported the incidence of children with PTB notified in China and assessed its epidemiological characteristics from 2009 to 2015 in order to formulate the effective and precise strategy for prevention and treatment.
Methods
Incidence
Child TB was defined as TB occurring in children aged under 15 years from the national TB programme. We used the definitions in the 2008 China National Guideline for PTB for bacteriologically confirmed or clinically diagnosed TB in the lung parenchyma or the tracheobronchial tree.8
Data sources
All notified child PTB cases were obtained from the TBIMS of the Chinese CDC. We included all notified child PTB cases in 31 mainland provinces from 2009 to 2015 and extracted the demographic, epidemiological and laboratory data for each patient. The annual population in children in China was obtained from the National Bureau of Statistics of the People's Republic of China and used to calculate the notified child PTB incidence in each province.
Statistical analysis
The annual incidence and annual smear-positive and bacteriologically positive case rates of notified child PTB were calculated and are displayed as a time series figure. The 95% CI of the PTB incidence was estimated with the Poisson methods. The spatial and temporal distributions of the incidence were plotted using ArcGIS software (V.10.2; ArcGIS Development Team, Open Source Geospatial Foundation Project). The other figures were created using R software (V.3.5.1). The χ2 test was used to assess the difference in the positive rate of X-ray abnormality, sputum bacteriology and smear between the notified child PTB group and the ≥15 years age PTB group. The statistical analyses were performed with SPSS software (V.20.0, Chicago, Illinois, USA), and all statistical tests were two-sided. P values <0.05 were considered statistically significant.
Ethics statement
The data used in this study were collected as a part of routine TB surveillance by the CDC. Individual consent was not required as this study was not considered research directly involving human subjects.
Results
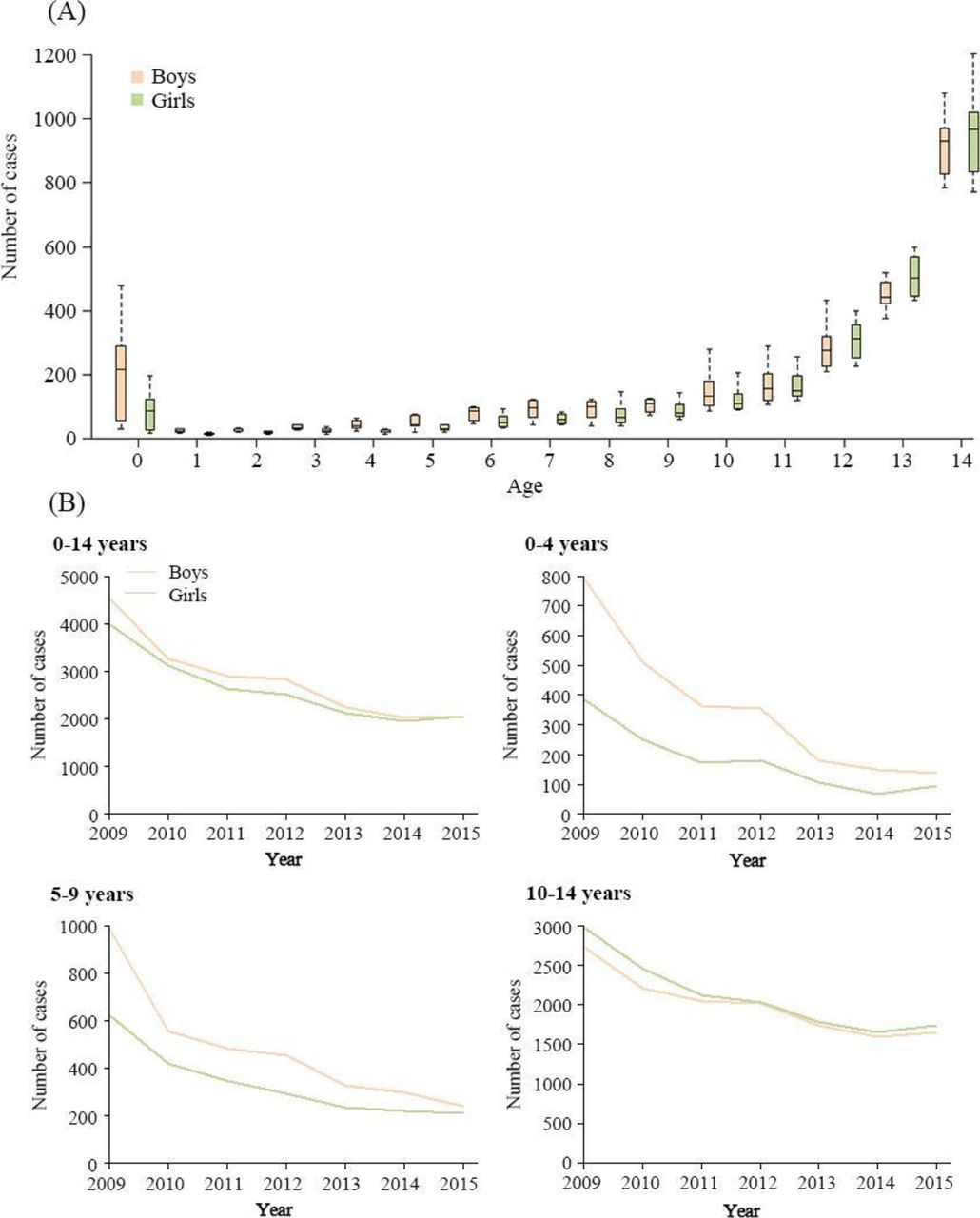
In total, 35 710 child PTB cases were reported in Mainland China from 2009 to 2015. The overall male to female ratio was 1.08:1. The 75.2% (26 857) of the cases were in the 10–14 years age group, followed by 14.7% in the 5–9 years age group (5258) and 10.1% in the 0–4 years age group (3595). Notably, the number of notified PTB cases was relatively high among the younger children (0–1 years old) and older children (12–14 years old) (figure 1A,B).
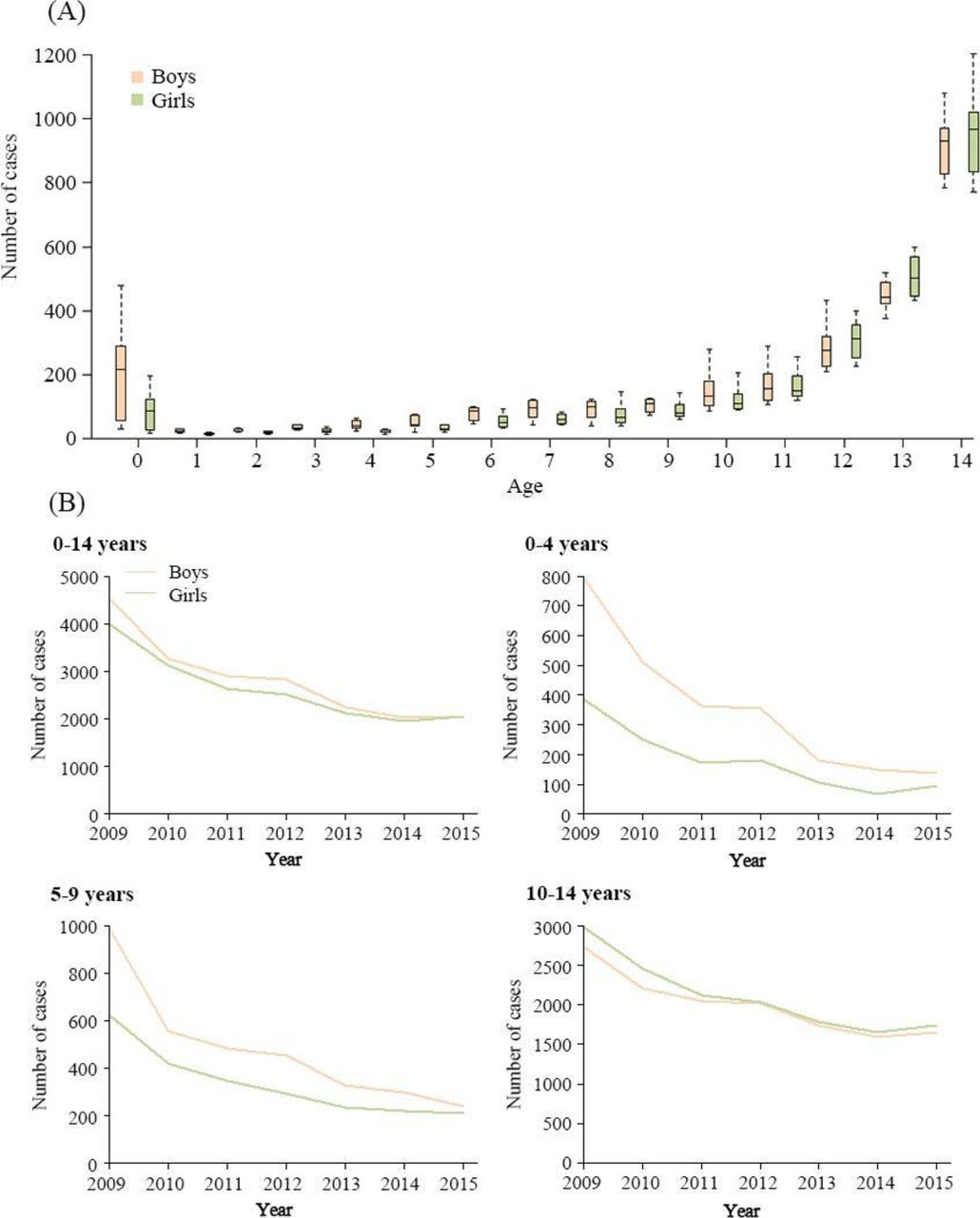
(A) The number of notified child PTB cases by age and sex in Mainland China, 2009–2015. The boxes represent 50% of case distribution, and the lines indicate the IQR. (B) The number of notified child PTB cases by age group, sex and year in Mainland China, 2009–2015. PTB, pulmonary tuberculosis.
Incidence and epidemiological characteristics
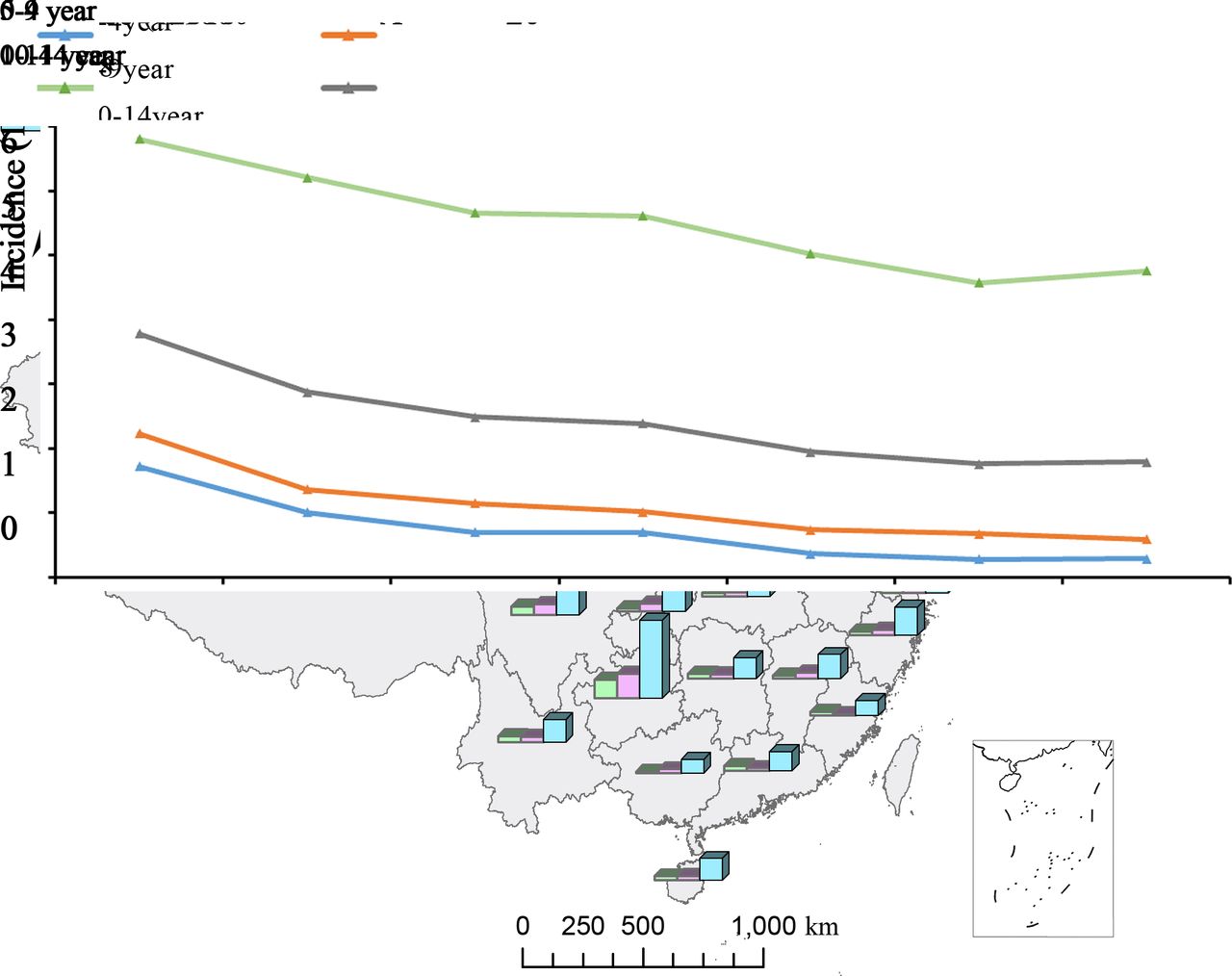
The average annual incidence of children with PTB notified to the TBIMS was 2.44/per 100 000 children (95% CI 1.77 to 3.10). From 2009 to 2015, the PTB incidence in children of all ages decreased by over 50%: from 3.78/105 to 1.79/105. The greatest decline was in the 0–4 years age group (83.1%), followed by 5–9 years age group (73.5%) The lowest decline was in the 10–14 years age group (30%) (figure 2A), which was also the age group with the highest incidence (figure 2B).

(A) The notified incidence of child PTB by age group and year in Mainland China, 2009–2015. (B) The notified incidence of child PTB by age group and Province in Mainland China in 2010. Note: Only the child population data by province and age in 2010 could be collected. PTB, pulmonary tuberculosis.
The highest geographical incidence was observed in the western region (3.86/105, 95% CI 2.80 to 4.92), followed by the central region (2.30/105) and eastern region (1.36/105) (online supplementary figure 1). Specifically, Tibet (15.95/105) had the highest incidence, followed by Guizhou (7.91/105) and Xinjiang (5.36/105) (figure 3). Although the overall incidence showed a decreasing trend, some provinces, such as Qinghai and Guizhou, exhibited small peaks in 2012 (figure 3).
Supplemental material

The spatial distribution of notified child PTB cases in Mainland China, 2009–2015. PTB, pulmonary tuberculosis.
The peak period of notified child PTB appeared from March to July, especially from May to July (figure 4A). Although the meteorology status differed among the different provinces, similar peak periods of notified child PTB were observed (figure 4B).

(A) The seasonal distribution of notified child PTB cases in Mainland China, 2009–2015 (B) The monthly distribution of notified child PTB cases by province in Mainland China, 2009–2015. PTB, pulmonary tuberculosis.
Laboratory test
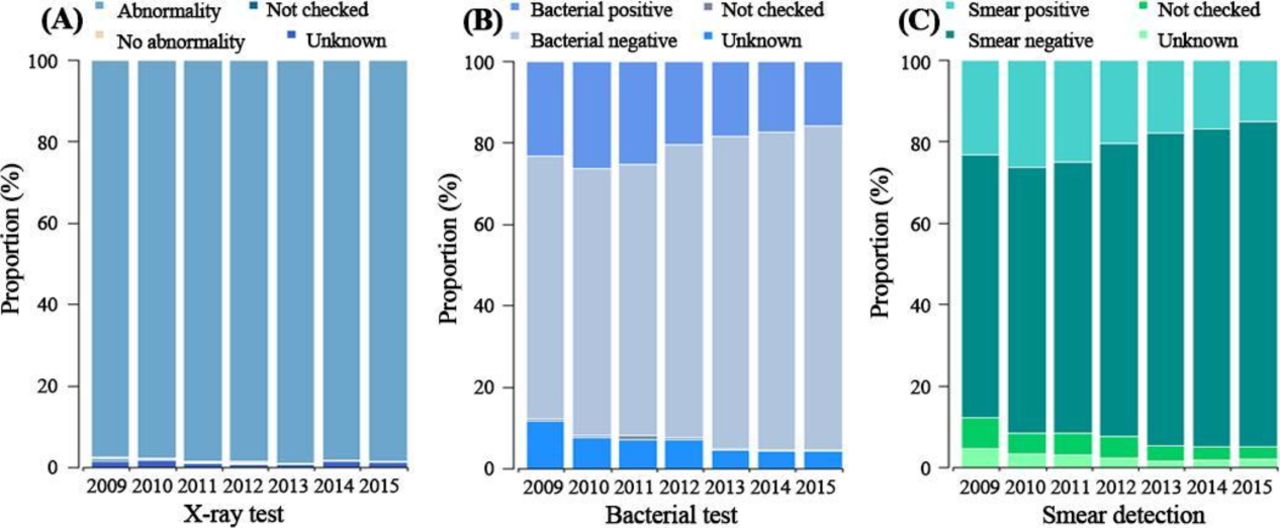
Generally, the positive rates of sputum smear and bacteriology, and chest X-rays abnormality were 21.5%, 21.7% and 98.1%, respectively (figure 5). The total positive cases of sputum smear and bacteriology, respectively, were 8216 and 8631. Specifically, the lowest positive rates of sputum smear and bacteriology were in the 5–9 years age group (5.2% (431/8216) and 5.1% (441/8631), respectively). However, the most positive cases of sputum smears and bacteriology were in the 10–14 years age group (84.3% (6922/8216) and 84.7% (7312/8631), respectively).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Proportions of notified child PTB cases determined by chest radiographs, sputum (gastric juice) smears and bacteriological tests (at least one positive smear or culture) in Mainland China, 2009–2015. (A) Proportions of notified child PTB cases determined by chest radiographs. (B) Proportions of notified child PTB cases determined by sputum (gastric juice) smears. (C) Proportions of notified child PTB cases determined by bacterial tests (at least one positive smear or culture). PTB, pulmonary tuberculosis.
Comparison of PTB in children and the ≥15 years age group
Notifications of child PTB only accounted for 0.6% of all notified PTB cases, with the maximum proportion of child TB cases in Tibet (2.85%) and minimum proportion in Jiangsu (0.28%) (online supplementary table 1). Although the incidence of both populations showed a downward trend over the 7 years, the decline in child PTB was more rapid than that in the non-child age PTB group (52.5% vs 21.2%).9 10 Similar to PTB in the whole population, the spatial distribution of PTB in children showed a high incidence in the west and a low incidence in the east of China (online supplementary figure 1 and figure 3).9 10 However, the peak period of notified child PTB, when mainly occurring from March to July and covering spring and early summer, appeared later and longer than that of all age PTB.9 Regarding laboratory tests, the positive rates of X-ray abnormality and sputum smear and bacteriology in the children with PTB were lower than those in the ≥15 years age group population (all p values <0.001).
Supplemental material
Discussion
Our study was derived from a large sample of more than 6 million notified PTB cases reported to the TBIMS during 2009 to 2015 in Mainland China and provides the most comprehensive epidemiology characteristics of notified child PTB in China since 2000.
We found that the average annual incidence was 2.44/105, which was higher than the average global level, but lower than that in India and Cambodia.11 From 2009 to 2015, the incidence of notified child PTB in Mainland China declined from 3.78/105 to 1.79/105, and the extent of the reduction was as high as 52.5%. This reduction may mainly be attributed to the use of the BCG vaccine and the Directly Observed Treatment Short Course (DOTS) programme. The application of BCG in China can be traced to the ‘Interim Measures for BCG Vaccination’ promoted by the Ministry of Health in 1954. By 2009, the national BCG vaccination rate reached 99%. Recently, a prospective Chinese cohort study suggested that the prevalence of latent TB infection in participants without a BCG scar (as unsuccessful BCG vaccination) were higher than that in those with a scar (as successful) who were younger than 50 years, specially 5–15 years old.12 The DOTS strategy was set on in the 1990s and was first implemented in 13 provinces in China.13 The strategy did not have nationwide coverage until 2005. The other reasons included the Law of Preventing and Controlling Infectious Disease amended since 2004 and TBIMS established and implemented since 2005.14 In summary, the combination, non-fragment of interventions made PTB in children substantially decreased.
The average predicted proportion of TB in children in China estimated by Peter J Dodd’s model was 6%,11 so the numbers of new child TB cases expected were approximately 50 000 per annum. In fact in our study the average annual notified cases of PTB in children were only 5450. The 10-fold difference may be attributed to the following reasons: first, for adults, the constituent ratio of PTB and EPTB was 90%–80% vs 10%–20%, however, for children, the ratio was 50% vs 50%.15 The Chinese law on infectious diseases requires that PTB, but not extrapulmonary TB (EPTB) be notified. Second, child patients with TB are treated at paediatric hospitals or large general hospitals, which are not directly linked to the TBIMS.16 17 Third, although we believed that many child TB, especially EPTB cases are not reported in China, the actual proportion may be less than 6% after 2010.18 19 Because of the above reasons, we are conducting a national survey to obtain the number of actual cases of PTB in children.
Similar to the ≥15 years PTB age group, the spatial distribution of PTB in children showed a high incidence in the West and low incidence in the East.9 10 The possible reasons are as follows: a relatively underdeveloped economy, poor medical resources and several outbreaks of TB in schools in the western region.4 The opposite status contributed to the low TB incidence in eastern China. In addition, the child PTB cases occurred approximately 2 months after the peak in other age patients with TB and lasted for a longer time, which may suggest that children have fast latent TB infection, and similar epidemic to other respiratory and childhood infectious diseases.20 21 We also found a higher incidence in the 0–1 years age group and the 12–14 years age group. The high incidence in infants may be related to immature immunity and close contact with patients with TB in a family.22 23 The status of children aged 12–14 years with TB may be related to the 10-year duration of BCG protection,24 and crowded living and learning conditions in schools.25 And the most positive sputum smear and bacteriology cases of the group may be caused by easily getting sputum and detection rates close to adults.
Sputum smears, culture and chest X-rays are the most common diagnostic methods, especially in primary care hospitals. However, the rate of X-ray abnormality of TB in children was lower than that in adults (p<0.05). The most common symptoms of TB in children are associated with the primary syndrome and hilar lymph nodes, which chest X-ray often fails to detect.6 26 For these symptoms, a low-dose CT has better sensitivity and specificity than chest X-ray.27 Considering the high risks of radiation exposure, CT examination should be considered for final diagnosis and differential diagnosis if all other tests are equivocal; it is not a screening test, like chest X-ray.28 29 Although, sputum smear and culture is the gold standard for TB diagnosis, the positive rate of sputum smear and bacteriology (p<0.001) was lower in children than in adults in our study. Because of difficultly getting sputum and underdetection, it is necessary to find new bacteriology methods for the diagnosis of child PTB. The Xpert mycobacterium tuberculosis (MTB)/rifampin (RIF) detection system, a new rapid TB diagnostic technology, has better accuracy than sputum smear and culture, and was recommended by WHO for the diagnosis of TB in children and in adults.30 31 In order to increase the detection rate of child TB, a series of guidelines and expert consensus, including new diagnostic methods and strategies are being formulated and implemented in China.32 33
Two of the limitations of this study were that our data were notified cases of PTB, no actual cases of PTB in children, and only covered the period from 2009 to 2015. So we can only present the incidence of children with PTB notified and the 7-year epidemiological characteristics of PTB in children in China.
Although the prevention and control of child TB seems to have succeeded in China over the past 7 years, the notified incidence is still low, relative to adults, suggesting substantial under-reporting. Thus, it is important to apply more effective care-seeking and promote identification and registration for children with TB.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
RY and ML are joint first authors.
Correction notice This article has been updated since it was published online. Ruling Yang and Mengyang Liu are the joint first authors. Also, the article type has been changed to Original article and we have added the abstract and the two key message boxes at the beginning of the paper.
Contributors RY and ML conceptualised and designed the study, drafted the initial manuscript, and reviewed and revised the manuscript. YZ, HJ, JY, QL, QL, YL, XW, HX and YY designed the data collection instruments, collected the data, carried out the initial analyses, and reviewed and revised the manuscript. XG and WL conceptualised and designed the study, coordinated and supervised the data collection, and critically reviewed the manuscript for important intellectual content.
Funding National Key Research and Development Program (2018YFC2000300), National Science and Technology Major Project of China (2018ZX10302302001004).
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon request.