Article Text

Abstract
Background Urinary tract infection (UTI) is a common childhood infection. Many febrile children require a urine sample to diagnose or exclude UTI. Collecting urine from young children can be time-consuming, unsuccessful or contaminated. Cost-effectiveness of each collection method in the emergency department is unknown.
Objective To determine the cost-effectiveness of urine collection methods for precontinent children.
Methods A cost-effectiveness analysis was conducted comparing non-invasive (urine bag, clean catch and 5 min voiding stimulation for clean catch) and invasive (catheterisation and suprapubic aspirate (SPA)) collection methods, for children aged 0–24 months in the emergency department. Costs included equipment, staff time and hospital bed occupancy. If initial collection attempts were unsuccessful subsequent collection using catheterisation was assumed. The final outcome was a definitive sample incorporating progressive dipstick, culture and contamination results. Average costs and outcomes were calculated for initial collection attempts and obtaining a definitive sample. One-way and probabilistic sensitivity analyses were performed.
Results For initial collection attempts, catheterisation had the lowest cost per successful collection (GBP£25.98) compared with SPA (£37.80), voiding stimulation (£41.32), clean catch (£52.84) and urine bag (£92.60). For definitive collection, catheterisation had the lowest cost per definitive sample (£49.39) compared with SPA (£51.84), voiding stimulation (£52.25), clean catch (£64.82) and urine bag (£112.28). Time occupying a hospital bed was the most significant determinant of cost.
Conclusion Catheterisation is the most cost-effective urine collection method, and voiding stimulation is the most cost-effective non-invasive method. Urine bags are the most expensive method. Although clinical factors influence choice of method, considering cost-effectiveness for this common procedure has potential for significant aggregate savings.
- urinary tract infection
- urine specimen collection
- health resources
- economic model
- child
Statistics from Altmetric.com
What is already known on this topic?
Obtaining a urine sample from young precontinent children can be challenging.
Samples can be collected using non-invasive (urine bag, clean catch and voiding stimulation for clean catch) or invasive (urethral catheterisation and suprapubic aspirate) methods.
Collection attempts can be time-consuming or unsuccessful, and samples may be contaminated and therefore not diagnostically conclusive.
What this study adds?
Catheterisation is the most cost-effective method of urine sample collection from precontinent children.
Voiding stimulation is the most cost-effective non-invasive method, and urine bags are the most expensive method.
Time occupying a hospital bed is the most significant determinant of cost.
Introduction
Urinary tract infection (UTI) is a common infection in early childhood, with a prevalence of 7% among febrile children aged 0–24 months.1 UTI is the most prevalent bacterial infection in children with fever of unknown origin,2 but clinical signs in young children are often non-specific. Urine collection is therefore required to diagnose or exclude UTI and is part of the diagnostic work-up for many febrile children in primary care and hospital settings. Collecting urine from young precontinent children can be challenging.
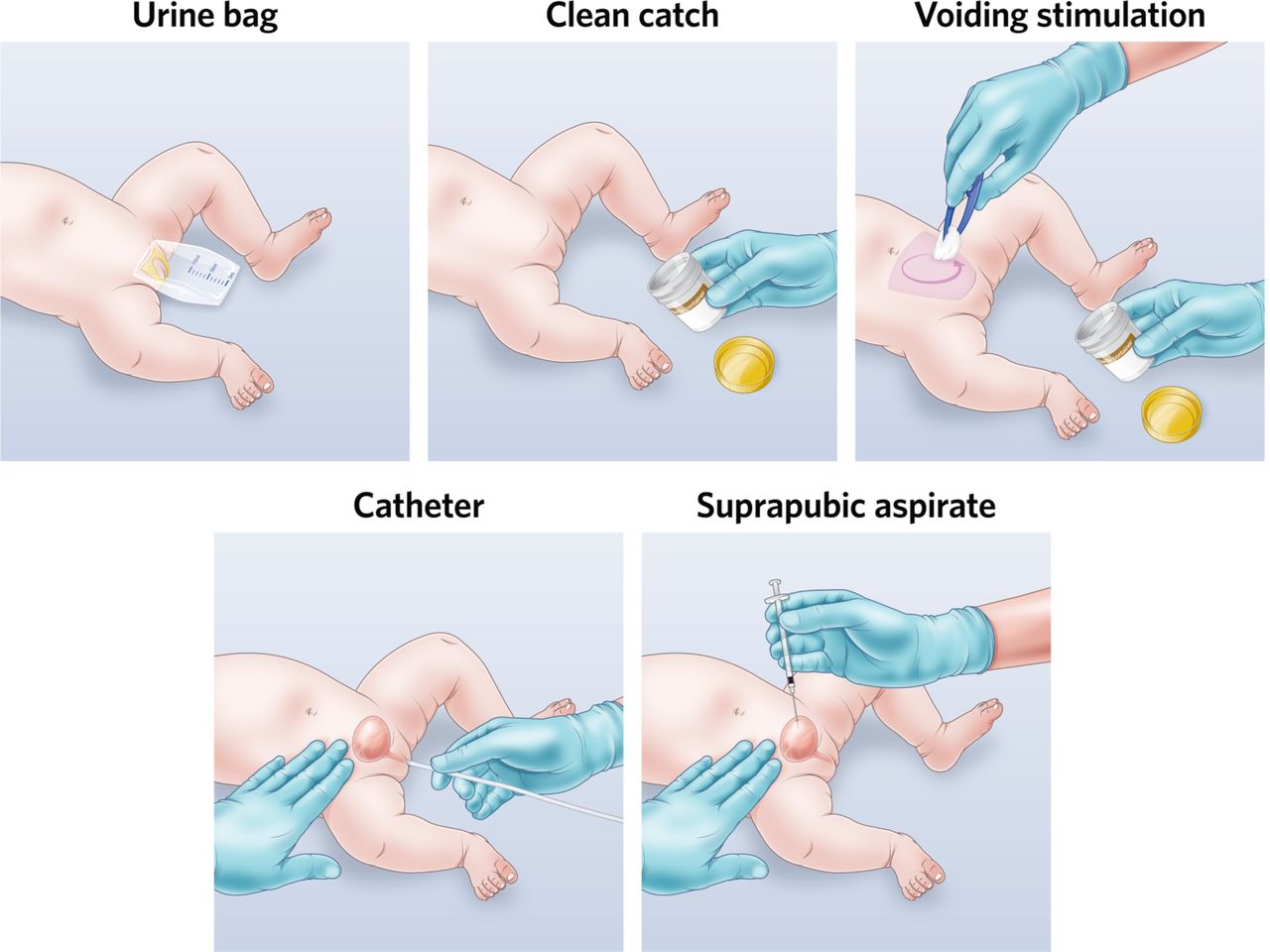
Common collection strategies include non-invasive (urine bag and clean catch) and invasive (catheter and suprapubic aspirate (SPA)) methods (figure 1). Each method has different limitations, clinical practice guidelines have differing recommendations3–5 and clinicians have different preferences for the preferred method.6 7 Non-invasive methods can be convenient but are time-consuming and have higher contamination rates.8 Invasive methods are more reliable, but require expertise and equipment to perform and are painful for the child.9 Collection success also varies between methods, so multiple attempts may be required to actually collect a sample.10 11 Recent studies have demonstrated that voiding stimulation techniques performed for 5 min such as bladder–lumbar manoeuvres and the Quick-Wee method can expedite clean catch collection,12 13 though not all studies are randomised.14 15

Urine sample collection methods for precontinent children. Images by Dr Jonathan Kaufman and Bill Reid, Royal Children’s Hospital. Voiding stimulation figure from Kaufman et al.15
Difficulties collecting urine samples can be costly and detrimental to patient care. Delayed collection will increase resource use and prolong hospital bed occupancy. Poor quality samples lead to missed diagnoses, unnecessary follow-up and investigations. Misdiagnosis leads to inappropriate antibiotic prescription. Complications and morbidity of untreated UTI are uncommon16 17 but can be significant.18 It is therefore important to efficiently obtain samples that are likely to be clinically definitive. Initial UTI screening uses bedside dipstick results.19 However, the gold standard for diagnosis is a positive culture in the presence of pyuria.20 Sample contamination corrupts these results. Choosing the appropriate collection method balances the clinical context, resource availability, speed, invasiveness, likelihood of success, contamination, parental preferences and costs.
Collection costs are potentially modifiable depending on the method used, but economic evidence regarding collection methods is scarce.21 Downs estimated urine bags cost an additional US$429 compared with catheterisation, based on unnecessary treatment of false-positive and contaminated samples rather than collection costs.22 Hollingworth et al estimated collection, testing and doctor time in general practice to cost GBP£33, based on clean catch and urine pad collection for children under 5 years in the Diagnosis of Urinary Tract infections in Young children (DUTY) study, not incorporating sample reliability.23
Current guideline recommendations for urine collection methods do not incorporate evidence of cost-effectiveness.20 23 No previous studies directly compare resource use and cost-effectiveness for different collection methods. While costs to collect a single sample may not be high, as a common procedure aggregate costs may be significant.
Methods
This economic evaluation includes detailed costing and decision analysis of common urine collection methods used for precontinent children in the hospital setting, using an emergency department (ED) health service perspective. The analysis evaluated the costs of sample collection, acknowledging that selecting the appropriate method is influenced by other clinical factors and resource availability. Average and incremental cost-effectiveness estimates are derived for each approach relative to catheterisation.
Diagnostic approaches
These include non-invasive (urine bag, clean catch and 5 min voiding stimulation) and invasive (catheter and SPA) collection methods.
Setting
The population of interest was precontinent children aged 0–24 months requiring urine sample collection in ED to evaluate fever or potential UTI. The Royal Children’s Hospital (RCH) is a tertiary paediatric hospital in Melbourne, Australia, with an annual ED census of approximately 90 000 patient contacts.
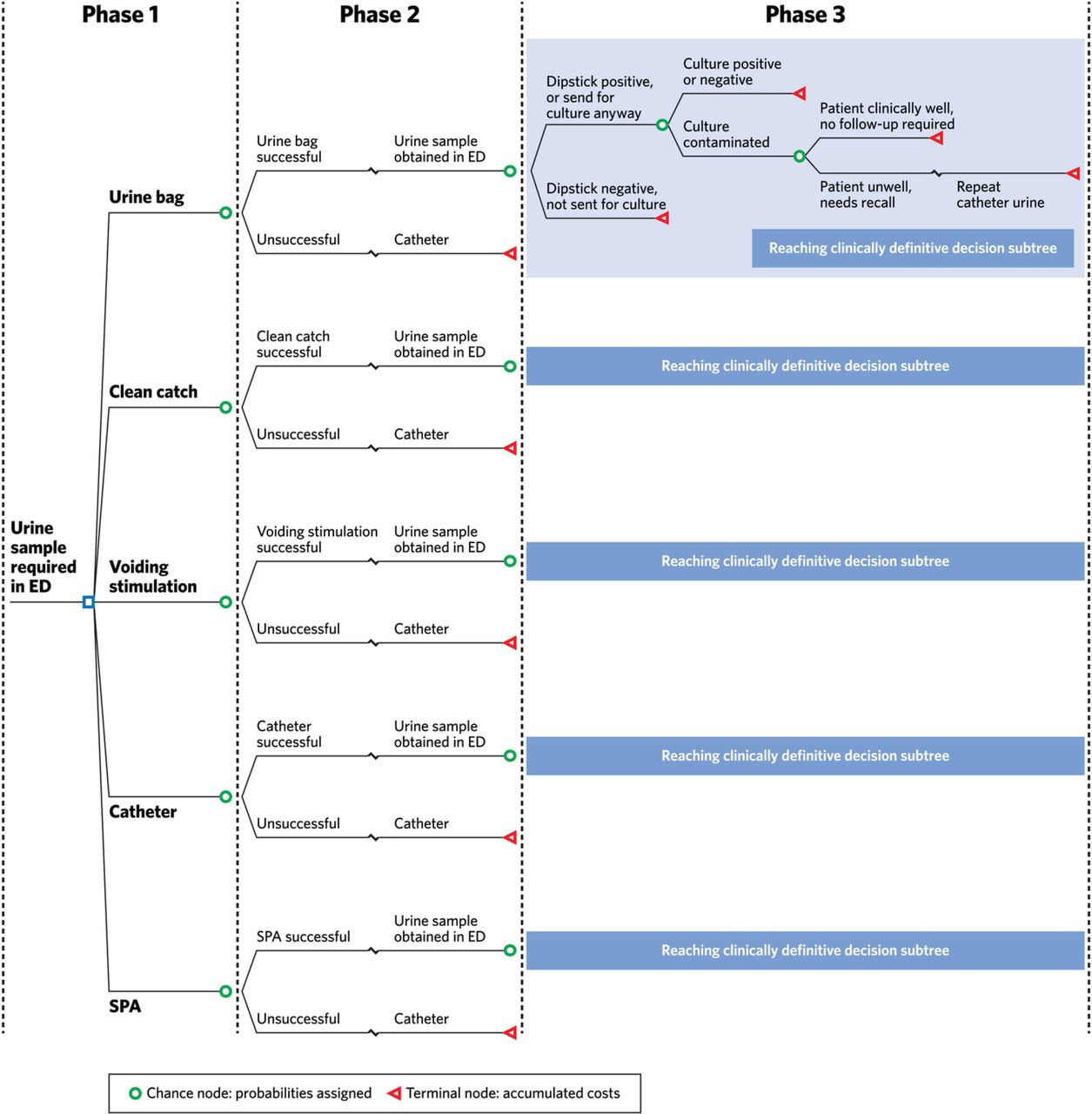
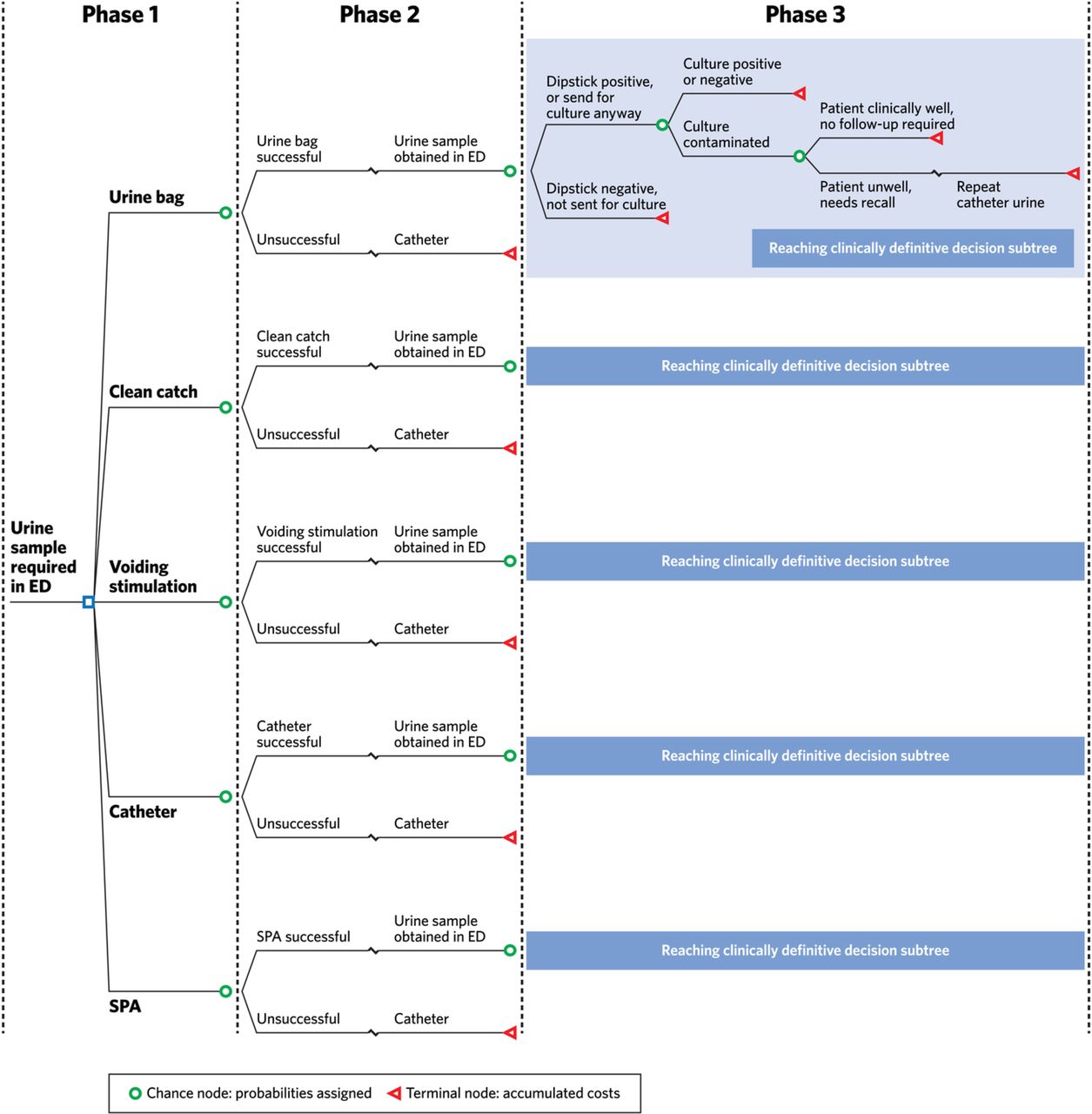
A probabilistic decision analytic model was constructed using TreeAgePro 2017.24 The model consists of three stages of attempting and collecting a urine sample and then reaching a definitive decision to exclude or diagnose UTI (figure 2). The three-stage modelling for each method is summarised as:
{kind=link}
{kind=link}
Decision tree for urine sample collection and UTI diagnosis. ED, emergency department; SPA, suprapubic aspirate.
Choice of urine collection method (first collection attempt).
Urine collection success (if first attempt unsuccessful, then sample collected by catheterisation).
Definitive UTI diagnosis (incorporating dipstick, culture and contamination results).
All children progress through the model until a urine sample is collected and sufficient information is available to reach a conclusive decision regarding UTI diagnosis. Cost-effectiveness is presented for stage 1 of the model only, as subsequent collection by catheter in stages 2 and 3 was assumed to be 100% effective after unsuccessful initial attempts. Further costs were added for stages 2 and 3.
Model parameters
Best estimates for model values and probabilities were obtained from a review of the published literature (table 1). Where multiple data were available, larger studies or those most reflecting the research setting were prioritised.
Model inputs: time, success and urine test results
Outcome assumptions
Some assumptions were required to complete the modelling, and these were based on usual local practice. We assumed non-invasive collection was performed by nurses, and invasive collection was performed by senior trainee level doctors with nursing staff assistance. Urine collection pads are not used in our hospital and were not included in the model. We assumed ultrasound guidance was not used. We assumed after failed initial collection attempts clinicians would go directly to successful catheterisation, consistent with the reported 100% success of catheterisation after failed SPA in previous studies.25 We assumed bedside dipstick testing was performed on all samples, with a binary positive/negative result, with all positive dipsticks sent for culture and some negative dipsticks sent for culture depending on collection method (table 1). We assumed cultures had a binary positive/negative or contaminated result, where contamination was heavy mixed growth and an uninterpretable outcome. We assumed consultant level doctors reviewed culture results, and if patients with contaminated samples were recalled that subsequent catheterisation would be successful and definitive.
Resource use and costs
Resource use was determined using prospective process mapping, directly observing 10 episodes of each collection method, to identify equipment use and staff time (nursing and medical) for each method. Mean equipment and staff costs for each method were calculated from these data (online supplementary appendix 2). Costs are presented in 2016 GBP£ (equivalent to $A2.08) using the 2016 Purchasing Power Parity from the Organisation for Economic Co-operation and Development Statistics (table 2).
Supplemental material
Costs used in economic model
We assumed standardised cleaning used one dressing pack and chlorhexidine ampoule. We assumed dipstick testing required equipment plus 3 min nursing time (£0.98), and culture testing required laboratory costs (which already incorporate microbiology scientist and clinician time) plus 6 min consultant doctor time checking results and contacting some families to revise prescriptions or recall patients with contaminated specimens if they remained unwell (£18.61), consistent with previous studies.23 For patients requiring recall, we assumed another 30 min ED presentation with repeat catheter urine collection plus dipstick and culture to clarify the diagnosis (£73.30). We observed all collection methods except urine bag, which is not routinely performed in our ED. We therefore assumed standard cleaning plus one urine bag and 5 min of nursing time was required for bag collection attempts.
Model validation using clinician survey
We surveyed 20 senior clinicians (consultant paediatricians and paediatric emergency physicians, mean 17 years clinical experience) to determine the face validity of the model and elicit expert opinion for probabilities not available from the literature (online supplementary appendix 1).
We first asked clinicians to estimate critical values used in the model for each collection method (table 1) including time, collection success, contamination, likelihood samples would be sent for laboratory processing after dipstick testing, and likelihood patients would be recalled for review if samples were contaminated.
We then revealed the values obtained from the literature review and asked the clinician if each data point was acceptable and plausibly reflected their local departmental practice. Where <80% of clinicians felt the data plausibly reflected local practice, we performed counterfactual scenario analyses using the mean clinicians’ estimate to determine the importance of that variable.
Analysis
Data from survey and process mapping forms was entered into Microsoft Excel (2017). Costs and probabilities were then assigned to the decision tree model in TreeAgePro (2017).24 The study followed the Consolidated Health Economic Evaluation Reporting Standards reporting guidelines.26
Sensitivity analysis
To determine the robustness of model assumptions, and describe the impact of uncertainty in parameter values, we performed sensitivity analyses for the complete model (stage 3). One-way sensitivity analyses were performed on the following key variables and assumptions (online supplementary appendix 1):
Staff, equipment and hospital bed costs each increased and decreased ±20%.
Non-invasive collection procedures performed by doctors rather than nurses.
All procedures performed by senior doctor (consultant level).
One-way analyses based on survey counterfactuals were also performed (appendices 1 and 3):
Urine bag effectiveness decreased from 96% to 67%.
Probability of bag samples sent to laboratory where dipstick negative reduced from 72% to 48%.
Clean catch time increased from 31 min to 83 min.
We considered any factor affecting the hierarchy of results or shifting final results by >25% to be meaningful.
Probabilistic sensitivity analysis was performed to examine the impact of the joint uncertainty of the model parameters. One thousand simulations were performed using Monte Carlo sampling to randomly sample from relevant parameter distributions (online supplementary appendix 3).
Results
For initial collection attempts, catheterisation had the most favourable average cost-effectiveness with a cost per successful collection of £25.98, and for non-invasive methods voiding stimulation had the most favourable cost-effectiveness with cost per successful collection of £41.32 (table 3).
Average costs and incremental cost-effectiveness of urine sample collection
To obtain definitive samples, catheterisation had the lowest average cost per definitive sample obtained (£49.39) and for non-invasive methods voiding stimulation had the lowest cost per definitive sample obtained (£52.25) (table 3).
Sensitivity analysis
The results of one-way sensitivity analyses of key variables are presented in online supplementary appendix 3. These analyses did not alter the hierarchy of model conclusions, indicating results were robust to changes in key parameters. Having consultant level doctors perform all procedures had the greatest impact, increasing costs by 6%–21% depending on method.
One-way analyses based on survey counterfactuals were also performed (online supplementary appendices 1 and 3). Increasing clean catch time by 170% increased the cost of collecting a definitive sample by clean catch from £64.82 to £118.15, indicating that time occupying a hospital bed is a significant driver of collection costs. Other counterfactuals did not substantially affect conclusions.
When simulated 1000 times, the average costs per definitive sample obtained were £48.60 catheterisation (95% CI £33.54 to £131.71), $50.67 SPA (95% CI £39.72 to £97.93), £51.21 voiding stimulation (95% CI £40.97 to £105.95), £65.03 clean catch (95% CI £30.27 to £313.48) and £126.43 urine bag (£59.92 to £323.38). Uncertainty in these results reflects some variability in the published data used to inform the model (table 1).
Discussion
Summary of findings
This study evaluated the cost-effectiveness of urine sample collection from an ED healthcare system perspective. Invasive methods were more cost-effective than non-invasive methods although with some simulated uncertainty. Catheterisation was the most cost-effective approach to obtain both initial and definitive samples. Catheterisation is highly effective, with moderate procedural costs and low contamination.8 SPA has even lower procedural costs and ultra-low contamination8 but is less effective at obtaining a sample.25 These invasive methods require equipment and technical expertise to perform. Resource availability and clinician experience may limit their utilisation in some settings. Use of invasive methods is also strongly influenced by clinical factors, discomfort caused to the child and parental preferences.9 27 28 Usual care will vary according to these factors, though in some settings urethral catherisation or suprapubic aspiration is already the dominant practice.20 Quality of life was not included in this study, but children’s pain and parents distress are important considerations.29
For non-invasive collection, voiding stimulation was the most cost-effective approach to obtain both initial and definitive samples. It is less effective but uses a shorter timeframe when performed for the recommended 5 min. We modelled voiding stimulation based on the published Quick-Wee method,13 as bladder–lumbar manoeuvres require multiple operators, and there are no randomised studies in the ED setting.12 Urine bags were the most expensive method for all stages of the model, reflecting their time-consuming nature and that high contamination means that samples are often not definitive.
Time spent occupying a hospital bed was the most significant determinant of collection cost. Therefore, expedient methods performed more favourably from this study’s costs perspective. Sample contamination also contributes to cost-effectiveness but was not the major determinant in the hospital setting. However, in the general practice context where parents may collect urine samples at home, contamination is likely to be a much greater determinant of costs.
The 2016 RCH costing data showed non-admitted UTI patients aged <24 months had a mean time in ED of 240 min, with 156 min occupying an ED cubicle, with a cost of £211.34 per episode. National data showed average costs for UTI patients aged <24 months of £261.40 per non-admitted ED episode.30 Urine sample collection therefore accounts for approximately 20%–50% of these costs, depending on collection method.
While ultrasound evaluation of bladder volume can increase the success of invasive collection attempts,31 32 its use is not routine for non-invasive collection, and the required equipment and expertise is not universally available.
Strengths and limitations
This is the first study directly comparing cost-effectiveness of urine sample collection by collection method. Model inputs were based on comprehensive data from the published literature, prospective process mapping and survey of expert clinicians. This is the first study to include all costs of collecting a sample, and the pragmatic considerations of progressively available dipstick and laboratory results used to reach a clinically definitive decision.
We made certain model assumptions, including that if the first collection attempt was unsuccessful, the clinician would proceed to catheterisation. This may not reflect all clinical scenarios but was a necessary simplification. We assumed non-invasive collection was performed by nurses and invasive collection performed by doctors; however, in some settings, non-invasive collection may be performed by doctors and vice versa. In sensitivity analyses, having all procedures performed by doctors did not change model conclusions. Our study was conducted in a tertiary paediatric ED. Results will not be directly generalisable to non-hospital settings such as general practice.
We did not include parental costs such as travel and time off work, although these would likely strengthen conclusions given parental costs likely reflect time taken. Quality of life was not included, but children’s pain and parents’ distress are important considerations.28 29
Clinical implications
Urine sample collection from young children is common in paediatrics, general practice and emergency medicine. Our findings provide new cost-effectiveness data to inform future guideline recommendations. Where invasive collection is indicated, these methods are cost-effective.
Where non-invasive collection is indicated, voiding stimulation methods are cost-effective and also expedite patient care. UK and European guidelines recommend clean catch as the preferred method of urine sample collection,4 33 although urine bag collection is frequently performed.34 In 2016, in our local setting at the RCH ED, 1776 urine samples from children aged 0–24 months were sent for laboratory processing from 87 797 patient presentations from all ages. This represents collecting urine for culture from a young precontinent child in 2% of all paediatric ED presentations. Samples were collected by clean catch (78%), catheter (11%), SPA (7%) or method unstated (4%). Using voiding stimulation in preference to standard clean catch in the ED could save £12.57 per sample and over £17 000 annually.
Conclusion
From a healthcare system costs perspective, the most cost-effective invasive and non-invasive urine collection methods are catheterisation and voiding stimulation, respectively. Urine bags are the most expensive method. Time spent occupying a hospital bed was the most significant determinant of cost. While clinical and patient factors strongly influence the choice of urine collection method, considering cost-effectiveness for this common paediatric procedure has the potential for significant cost savings.
Acknowledgments
We would like to thank the families and clinical staff from the Royal Children’s Hospital (RCH) emergency department who participated in process mapping of collection procedures, Bill Reid from the RCH Creative Studio for assistance with illustrations, Poh Chua from the RCH Library for assistance with literature searching and Max Catchpool from the University of Melbourne for assistance with TreeAge modelling. We would like to thank Thomas Greenhalgh from the Independent Hospital Pricing Authority and Chris Jackson, Malathi Jeremiah and Elin Wee from the RCH Decision Support Unit, for their assistance with costs data collection. We would like to thank Amanda Di Carlo and Nigel Kelly from the RCH Laboratory Services for their assistance with laboratory data collection.
References
Footnotes
Contributors JK was the lead author of the manuscript. All authors contributed to the initial study design. JK completed the literature review and acquired all data for the clinician survey, process mapping and cost analysis. JK designed the economic model and completed the analysis with substantial input from AK and KD who supervised the modelling and interpretation of results. PAB and FEB contributed to clinical aspects of the model. JK wrote the first draft of the manuscript, and all authors contributed to revising the manuscript. All authors had final approval of the version to be published. JK and KD take responsibility for the paper as a whole.
Funding JK is supported in part by an Australian Government Research Training Program Scholarship and Melbourne Children’s Postgraduate Health Research Scholarship. FEB is supported in part by a National Health and Medical Research Council Practitioner Fellowship and Melbourne Children’s Clinician Scientist Fellowship. PAB is supported in part by a Melbourne Children’s Clinician Scientist Fellowship. KD and AJK declare no funding related to this paper. The RCH Melbourne receives infrastructure support from the Victorian Government’s Infrastructure Support Program, Melbourne, Australia.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study protocol (HREC reference 35083E) was approved by the Royal Children’s Hospital human research ethics committee. All participants gave informed consent.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.