Article Text

Statistics from Altmetric.com
It would be hard to imagine providing care for an acutely unwell child without giving him/her supplemental oxygen. This is what we do, what advanced paediatric life support courses require; it is also what the public expects of us. Oxygen—in the developed world at least—is seen as the panacea that can do no harm, to not give it in a child’s hour of need would be considered by some to be negligent. Every television medical drama we are exposed to contains images of unwell patients, all with an oxygen mask to signify the degree of severity of their illness. So how did this potentially toxic byproduct of photosynthesis become the most commonly administered drug in hospitals? Oxygen unlocks the energy stored within the food we eat during the mitochondrial production of ATP: ‘oxidative phosphorylation’. If this process ceases, energy failure and hypoxic death usually follows. Thus, for decades our focus has been to ensure a steady flow of oxygen from the air we breathe to every cell in the body to maintain cellular aerobic respiration. Taking no chances, and supplying patients with excessive amounts of supplemental oxygen, was assumed to be the safest strategy. But as we know from other walks of life, too much of a good thing is rarely in our best interest. Joseph Priestley eloquently pointed this out to the world when reporting his discovery of oxygen: ‘…for, as a candle burns out much faster in dephlogisticated than in common air, so we might, as may be said, live out too fast and the animal powers be too soon exhausted in this pure kind of air’.1 His wise words seem to have been forgotten over the subsequent centuries.
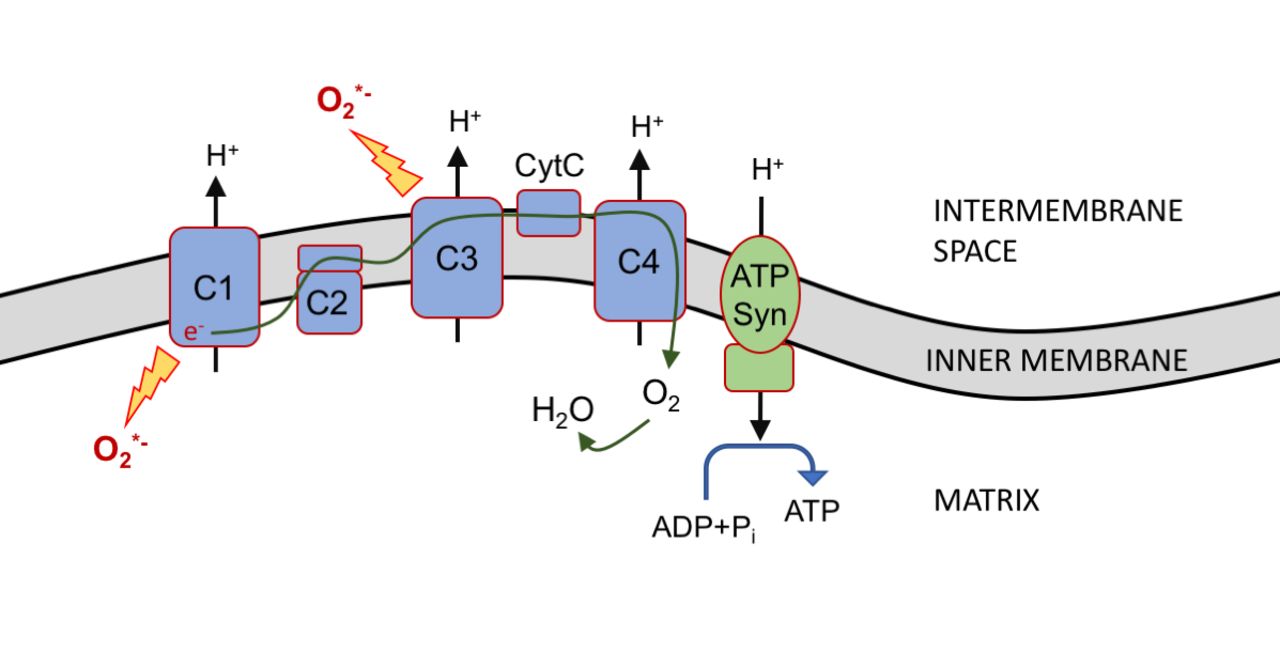
Respiration involves the oxidation of fuel substrates and reduction of oxygen during reactions catalysed by the electron transfer system. ATP is generated through the coupling of this process. Reactive oxygen species (ROS) are released from complexes 1 and 3.
The paradox is that this life-giving gas also has the potential to cause harm. This requires some explanation. A number of key intracellular enzymes that are involved in oxygen metabolism ‘leak’ slightly and as a result release ROS. These molecules play an essential role in cell signalling and homeostasis, but in excess they take on a rather more sinister role. One of the sites of ROS generation is the inner mitochondrial membrane, emanating from complexes 1 and 3 during oxidative phosphorylation (figure 1). Cellular oxygen tension has a significant effect on the rate of ROS production, with even modest increases in oxygen PaO2 leading to substantial radical release.2 Natural defence from excessive ROS comes from innate antioxidants, primarily enzyme systems that neutralise them to more innocuous molecules. However, these systems are easily overwhelmed when ROS production is high, causing an imbalance of reduction-oxidation that leads to oxidative stress. In this state, ROS wreak havoc throughout the cell, destroying mitochondrial and cellular DNA, structural proteins, enzymes and lipids. Like the inevitability of iron rusting in the presence of oxygen and water, cells struggle to withstand the onslaught of ROS when oxygen is in abundance. Altered mitochondrial membrane permeability leads to them swelling, becoming dysfunctional and ultimately to autophagy. High levels of oxidative stress can result in apoptosis and necrosis which clinically manifests as organ dysfunction and failure.

{kind=link}
Oxidative phosphorylation and the production of mitochondrial reactive oxygen species. ADP, adenosine diphosphate; ATP Syn, ATP synthase; C1–4: complexes 1 to 4 ; CytC: cytochrome C; O2 *−: superoxide radical; Pi, inorganic phosphate.
Current guidance for acutely unwell adults and children advises that oxygen should be titrated to achieve an oxygen saturation of 94%–98%3 4; however, no evidence-based guidelines exist for patients admitted to a critical care unit. Recently, a spotlight was focused on the clinical implications of oxygen therapy for acutely unwell patients with the publication of Chu et al’s systematic review and meta-analysis of oxygen use in acutely unwell adults.5 In this well-constructed study the authors brought together literature from 25 randomised controlled trials (16 037 patients) that compared conservative to liberal oxygen administration. Their conclusion was that liberal oxygen therapy was associated with a higher mortality than more conservative oxygenation, without improving other patient-important outcomes (relative risk 1.21, 95% CI 1.03 to 1.43). Perhaps this is evidence that unrestricted oxygen may cause harm and that we need to reconsider the traditional notion that little harm can be done when overoxygenating patients. However, like many meta-analyses, the information gained from the computations is only as reliable as that which is fed into the formula. The studies included in this analysis were highly diverse. Clinical scenarios ranging from emergency surgery to stroke were included. This makes it difficult to determine the validity of the results in any individual setting. The nature of the intervention also varied across studies, with some comparing selected oxygen concentrations (administered) and others comparing selected arterial oxygenation targets (measured).
More importantly though, Chu et al’s meta-analysis does not provide any information about the management of acutely unwell children. Only one group relevant to the Archives of Disease in Childhood readership has been studied in detail to date: extreme premature infants (<28 weeks, n=4965 in five trials) have been randomised to lower (85%–89%) versus higher (91%–95%) oxygen saturation targets. Complex trade-off between retinitis of prematurity and necrotising enterocolitis have been observed with no net benefit or harm on death or major disability at a corrected age of 18–24 months.6 Risk/benefit profiles from extremely premature infants cannot be reasonably extrapolated to older infants or children. Data are now emerging in this population. Cunningham et al randomised 615 ward admissions with bronchiolitis to SpO2 target of ≥94% or≥90% and showed this to be equivalent in terms of safety and clinical effectiveness.7 The lower target was associated with a clinically significant reduction in amount of time participants received oxygen: 27.6 (0 to 68.1) hours vs 5.7 (0 to 32.4) hours HR 1.37 (1.12 to 1.68), p=0.0021 and time to discharge 50.9 (23.1 to 93.4) vs 40.9 (21.8 to 67.3), p=0.003. The recent Oxy-PICU trial from the paediatric intensive care society study group studied 120 emergency admissions to paediatric intensive care units receiving mechanical support for respiration and supplemental oxygen. Randomisation was to either a more restrictive oxygen therapy peripheral oxygen saturation (SpO2) target (88%–92%) or standard care (SpO2 >94%). No safety concerns have been identified, and a definitive trial is both feasible and considered a priority by the specialty.8
What mechanisms may underlie an apparent benefit of a lower than normal SpO2? Maybe the explanation is a simple one; that a normal SpO2 is not harmful in itself, but attempting to achieve it in patients with hypoxaemia may be. In other words, our efforts to improve a patient’s arterial oxygenation with a high fractional inspired oxygen leads to oxidative stress in the lung parenchyma, ‘rusting’ the lungs and exacerbating the original lung injury. The additional damage caused by positive pressure ventilation compounds the issue. Thus, tolerating a lower SpO2 may reduce the magnitude of these interventions and avoid their unnecessary harm. This ‘less is more’ approach to the administration of oxygen in acutely unwell patients (both children and adults) clearly requires a great deal more research in order for us to fully understand its potential merit in different circumstances. Our previous love affair with oxygen is entering a turbulent time. As our knowledge of physiological rusting expands, we become ever more aware of the harmful side of oxygen. But should we blame oxygen radicals and seek to limit them or should we blame our clumsy use of oxygen and modify this? While the results of the recent meta-analysis may tempt us to dial down the oxygen, we should wait until the results of ongoing and planned studies become available.
Footnotes
Contributors DM and MJP contributed equally to the writing of this article.
Funding None declared.
Competing interests None declared.
Provenance and peer review Commissioned; internally peer reviewed.