Article Text

Abstract
While maternal and perinatal mortality auditing has been strongly promoted by the World Health Organization (WHO), there has been very limited promotion or evaluation of child death auditing in low/middle-income settings. In 2017, a standardised child death review process was introduced in the paediatric department of the National Hospital in Honiara, Solomon Islands. We evaluated the process and outcomes of child death reviews. The child death auditing process was assessed through systematic observations made at each of the weekly meetings using the following standards for evaluation: (1) adapted WHO tools for paediatric auditing; (2) the five stages of the audit cycle; (3) published principles of paediatric audit; and (4) WHO and Solomon Islands national clinical standards of Hospital Care for Children. Thirty-three child death review meetings were conducted over 6 months, reviewing 66 neonatal and child deaths. Some areas of the process were satisfactory and other areas were identified for improvement. The latter included use of a more systematic classification of causes of death, inclusion of social risk factors and community problems in the modifiable factors and more follow-up with implementation of action plans. Areas for improvement were in communication, clinical assessment and treatment, availability of laboratory tests, antenatal clinic attendance and equipment for high dependency neonatal and paediatric care. Many of the changes recommended by audit require a quality improvement team to implement. Child death auditing can be done in resource-limited settings and yield useful information of gaps which are linked to preventable deaths; however, using the data to produce meaningful changes in practice is the greatest challenge. Audit is an iterative and evolving process that needs a structure, tools, evaluation, and needs to be embedded in the culture of a hospital as part of overall quality improvement, and requires a quality improvement team to follow-up and implement action plans.
- child mortality
- quality improvement
- clinical audit
- low/middle-income countries
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Auditing of paediatric deaths has rarely been evaluated in hospitals in low/middle-income countries, although it is vital for improving the quality of care provided in any health facility. The published experience on child death auditing is limited to a few countries only, and some of these reports are retrospective descriptions of case-mix and common causes of death rather than an evaluation of the audit process.1–7 Like many low/middle-income countries Solomon Islands does not have a well-developed coronial service or vital registration system, so only child deaths from unnatural causes are subject to official review.
In early January 2017, a new child death review process was introduced in the paediatric department at the National Referral Hospital (NRH), Honiara, Solomon Islands. The process was developed with tools adapted from the WHO, using forms designed to classify the causes of death, identify modifiable factors and develop action plans (see Annex).8 WHO has not yet published these tools, but they were developed at a WHO meeting on child death reviews held in Geneva in November 2016, attended by staff from the Western Pacific Region.
Setting
Solomon Islands is a Pacific Island nation with a population of 600 000, with nine provinces spread over almost 1000 islands. The under 5, infant and neonatal mortality rates in 2012 were 31, 26 and 14 per 1000 live births, respectively. NRH is the only tertiary referral centre for seven government-run provincial hospitals and four mission-run hospitals in Solomon Islands. Honiara is the capital of Solomon Islands in Guadalcanal province. The estimated population for Honiara city is 84 444 and Guadalcanal province is 139 164. Each year there is an estimated 5% increase in urban migration from other provinces to Honiara. Children requiring medical care are referred by their provincial or community hospitals.
The paediatric department is made up of two clinical areas: the Children’s Ward and the Special Care Nursery (SCN). The department medical team is composed of two consultant paediatricians, five registrar doctors and resident medical officers (RMO). There are 34 registered nurses; 17 nurses in SCN and postnatal ward, and 17 nurses in the Children’s Ward.
There are 32 beds in the Children’s Ward, 8 beds in the SCN and 40 beds in the postnatal ward. Most paediatric patients came through the emergency department or referral clinics where they are triaged before being managed by the paediatric team. High-risk deliveries and sick newborns in the labour ward are comanaged with the obstetric team, before being transferred to the SCN.
Death auditing process
The child death review system was introduced in January 2017. We adapted guidelines for paediatric audit based on tools from the WHO and others.8 9 The process involves summarising the deaths for audit discussions, identifying modifiable factors, deciding action plans, implementing action plan and evaluation. Standard child mortality auditing forms for gathering clinical information, a registry sheet of all deaths and an audit summary and action plan form were used (online supplementary appendix).8
Supplementary file 1
Once a week neonatal and child deaths were audited by the paediatric team after morning handover of the night staff to the day staff. All staff, medical, nursing and administrative, were invited and encouraged to attend. The cases were summarised, discussed and information sent to the Ministry of Health for processing of death certificates.
We aimed to evaluate the nature and quality of information that was generated by these audits and assess how complete the audit process was, based on WHO and other published standards. Specifically, we aimed to: identify areas in the current death audit process that needed improvement; assess the classification of causes of deaths; and assess and refine the classification of modifiable factors that may provide lessons for improvement.
Methodology
Through systematic observations at weekly paediatric audit meetings for 6 months, we described the process of auditing child deaths. The process was assessed based on: (1) adapted WHO tools for paediatric auditing (online supplementary appendices 1–4); (2) the five stages of the audit cycle10; (3) published principles of paediatric audit9 and (4) WHO and Solomon Islands national clinical standards for Hospital Care for Children.11 12
The meetings were chaired by one of the consultant paediatricians. A registrar summarised the cases using a slide presentation. Four meeting participants were given death auditing forms to identify modifiable factors and document action plans agreed to in the discussions. They also had the task of ensuring that vital registration death notification forms were completed. All nurses and doctors were encouraged to attend and participate in the audit discussions.
The child death review meetings were held weekly. In addition, at the end of each month the paediatric team re-presented neonatal cases with the obstetric team and sought to identify any reproductive health or obstetric-related issues and modifiable factors.
Systematic observations were made at each meeting of: (A) whether the principles of problem-solving audit and WHO recommendations on paediatric audit were followed; (B) learning and education opportunities provided by the audit process; (C) documentation; and (D) whether the five stages of audit were achieved.10
The five stages of the audit cycle are:
Identifying deaths, or serious adverse or sentinel events, preparing and conducting an audit;
Summarising information on causes of death and avoidable or modifiable factors using a standardised instrument;
Analysing the results and generating age and cause-specific mortality rates, and trends over time;
Recommending solutions to address modifiable factors and implementing recommendations;
Evaluating whether improvements were effective and sustained.
Data for the clinical case audit were collected from patient medical records and other sources prior to the audit. Patient reporting forms were completed manually, and presented at the audit. The audit meeting was responsible for assigning causes of death and identifying modifiable factors and action plans.
Data entry was done in an Excel spreadsheet. Patient details and descriptions were included in the spreadsheet to avoid double entry. The data on modifiable factors and classification of causes were then grouped for analysis, and specific details of the modifiable factors were also recorded.
The researchers were part of the paediatric team who conducted or participated in the audit, but the evaluation was predesigned to be as objective as possible. MS gathered the data on processes.
Results
Thirty-three child death review meetings were conducted over 6 months, auditing on average two deaths per meeting. The following evaluations were made.
Attendance at the meetings was voluntary, a role was kept at each audit and the average attendance was 13. Staff were encouraged to attend and participate each week as part of routine department activities. Doctors always attended the death meetings, but a lower proportion of nursing staff attended. The combined obstetric–paediatric neonatal death audits were held monthly and the average attendance was 41.
Auditing schedule
The child death review meetings were scheduled weekly. We managed to review all deaths by the end of the calendar month in which the death occurred. On rare occasions, the meeting was postponed due to high clinical workloads, and some weeks two meetings were held to deal with a backlog of cases before the end of the month.
Atmosphere and approach
The meetings had a welcoming atmosphere. Errors were not singled out on individuals but identified in order to improve. The team leader would always encourage a respectful and non-blameful approach to discussing cases.
Confidentiality
For most of the cases discussed, confidentiality was maintained during and after the discussion. This was achieved through verbal reminders by senior doctors during the audit. New staff needed to be reminded of the importance of maintaining patients’ and clinicians’ identifying information confidential.
Searching for common patterns rather than focusing on individual mistakes was consistently exercised during the audit. For example, in looking for reasons why laboratory staff on call were unavailable at night, rather than why an individual was not available during night duty. This identified situations where difficulty getting laboratory staff at night was due to the staff having to be picked up from home to hospital, the team saw this as a limitation in hospital management for not providing prompt transport for laboratory staff or having a room to rest during on-call hours.
Acknowledgement of health workers’ effort was also exercised. The practice of highlighting genuine efforts of staff in managing a case despite the outcome was usually practised during the audits. This approach transferred to improvements made in handing over of cases at changes of shifts, where both positive aspects of management as well as clinical problems remaining and tasks to be completed were discussed.
Learning and education role
The child death review meetings provided a learning time for junior doctors and other staff. Cases were openly discussed with the paediatricians who helped provide relevant information on clinical management and what may be done to improve in future. At times when the number of deaths to discuss was high or the clinical workload demanded, teaching was limited. It might be sometimes that it is best to discuss one or two cases in detail and have the lessons discussed than to cover many more deaths superficially without the learning aspect.
Communication
Doctors sometimes failed to update ward nurses on issues and challenges identified, or actively seek their input. Because night staff were unable to attend communicating with these staff needed special attention.
Modifiable factors
During each audit meeting modifiable factors were identified and the team suggested certain action plans to address them. Initially, most factors identified were medical, nursing or healthcare related, but for many deaths it was apparent that social and environmental factors were critical. A list of commonly encountered modifiable social factors was drawn up to highlight these (online supplementary appendix 5).
Action plan implementation
Although action plans were formulated at each audit meeting, there was not sufficient effort given to implement the action plans. It was sometimes assumed that the doctor preparing the death audit summary was to carry out the tasks. Initially, there was no other identified group of people to assist in implementing the action plans. A quality improvement team has now been identified to implement the action plans.
Summary of cases reviewed
Sixty-six child deaths were audited in 33 weekly meetings over 6 months, out of 969 paediatric admissions (table 1). There were 48 neonatal deaths and 18 deaths on older children: 45 were male, 21 female. Eight of the 66 cases were referred from other hospitals, only two of which were neonatal deaths. There were substantial delays in the referral of seven of these eight cases, including for both the neonates. Delayed presentation was a problem overall: five of the 18 children over 1 month of age had been acutely unwell for more than 2 weeks before presenting to a health facility.
During the period of study, 969 paediatric cases were admitted and 66 children died (6.8%)
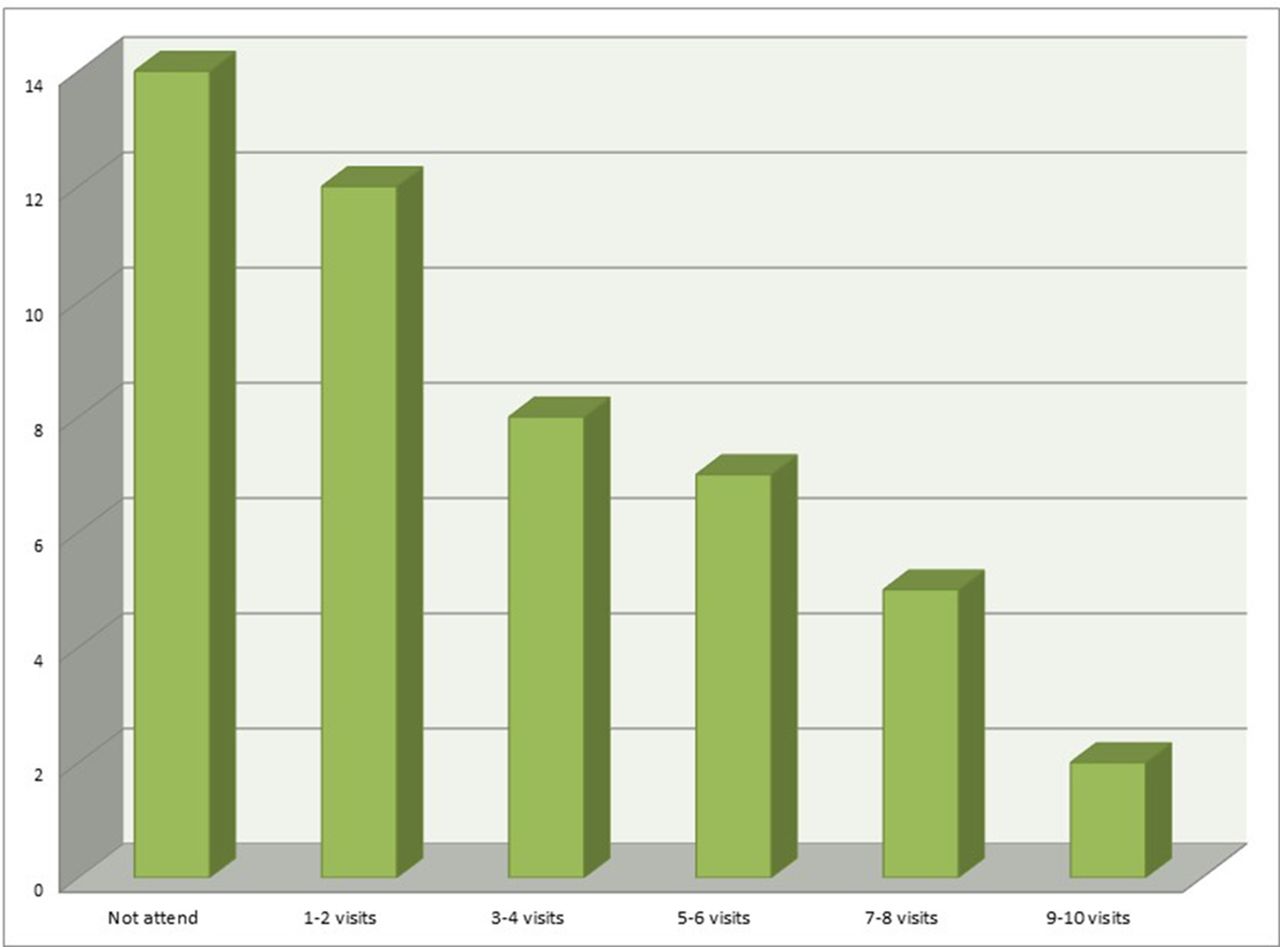
Of the 48 neonatal deaths, 28 and 38 occurred within the first 24 and 48 hours of life, respectively. Twenty-eight neonates had low birth weight; of which 10 had very low birth weight and 7 had extremely low birth weight, and 18 were preterm. Fourteen mothers of neonates who died did not attend antenatal clinic, and deaths were more frequently occurring with fewer antenatal clinic attendances (figure 1). Immediate causes of death are described in table 2. Underlying causes of death were identified for many neonates: 18 prematurity, 6 had congenital anomalies, 3 had antenatal trauma.
{kind=link}
Number of neonatal deaths and the frequency of antenatal visits.
Immediate causes of deaths for neonates
Seven of 18 children older than 1 month died in the first 24 hours of hospital admission. Seven of 18 had moderate or severe malnutrition. Immunisation rates were relatively high; 83% of children older than 1 month were fully immunised for their age.
Immediate causes of death were identified in older children, summarised in table 3. Underlying causes included malnutrition,8 pneumonia,3 acute gastroenteritis3 and congenital heart disease.2
Immediate causes of deaths for children >28 days
Modifiable causes were identified in the child death review meetings (outlined in table 4). Up to 171 instances of modifiable factors were identified. Although modifiable factors were found in more than half of the deaths, 20 (30%) were considered to be potentially avoidable within the confines of existing health resources.
Some of the modifiable factors identified during the audit meetings
Although we grouped modifiable factors (table 4), some require further detail to understand exactly the interventions that might address them. Insufficient patient assessment included poor history taking and poorly documented physical examination that affected the assessment of cases or led to missed diagnoses. Insufficient treatment included inadequate or inappropriate antibiotics, inadequate monitoring with pulse oximetry and inadequate documentation of fluids administered. Unavailability of medical laboratory tests included delays in blood collection or test ordering, tests not being followed up by doctors, shortage of reagents for testing, dysfunctional machines or laboratory staff not being available.
Delayed referral and presentation were identified in some deaths. Lack of availability of transport was the most common reason for delayed referral from outer provinces or rural areas to Honiara. Most transports used open boats with outboard motors, with inadequate referral support (table 5). This leaves children exposed to environment during the often lengthy time of travelling across the sea often in the rain. In Solomon Islands, there are no referral ambulance services and no standard equipment for safe transfer of medically unstable patients. At times transfer is done in boats by relatives or friends who lack the knowledge and skills to manage very sick infants and children.
Mode of first line of transportation to hospital for referred and non-referred cases
Discussion
While there has been considerable descriptions of the process of maternal and perinatal death auditing,13–24 and WHO has provided tools and resources to scale up and evaluate Maternal Death Surveillance and Response,25 26 there has been very little research on child death auditing and how to make it effective in low-resource settings. This study builds on recent efforts by WHO to provide a framework for this. Even in an era of ‘big-data’27 28 learning the lessons from detailed analysis of individual cases has an important value.7 WHO held a meeting on Child Death Review in Geneva in November 2016, and this study was an attempt to pilot the tools developed and evaluate the process.
The first 6 months of our child death review process succeeded in some ways and fell short in others. The weekly audit meetings were well attended, and provided opportunities for teaching. Confidentiality was achieved, as well as a positive atmosphere of voluntary participation and no blame. Regular reminders of the confidential nature of discussions were important, and nursing staff needed encouragement to attend. Causes of deaths were classified, although there was a need among health workers to clarify what constitutes an immediate and underlying causes of death, as there was overlap.
On occasions, time was a limitation and it was not possible to review all cases scheduled in the session due to ward work pressure and the team postponed a case to the next meeting. Although much of the discussion was based on written documentation, delaying audit reduces the clarity of recall by staff involved.
At least 171 instances of modifiable factors being present were identified. However, formation and implementation of action plans were the main challenges in the current process. Some of the modifiable factors were systemic or cross-cutting issues between various medical disciplines and other departments at the hospital. These require systemic approaches, interactions between departments, or the hospital management for decision-making. Limited knowledge and skills and lack of human resources capacity, especially low numbers of nurses, were limitations to implementing change. Some of these can be improved by continuing professional development, but other factors such as staff morale, perceived value of the individual, role expectations, ethics and attitude have to be addressed as part of a positive and supportive organisational culture. Some modifiable factors require changes beyond the hospital to peripheral health settings, community child health and outside the health sector, and thus require wider engagement.
It was identified that with current facilities neonatal care in Honiara is under certain stresses. An earthquake in Honiara in December 2016 caused damage to the walls of the labour ward; the delivery rooms were condemned and in 2017 the labour ward was in a makeshift building. Infection control and Early Essential Newborn Care practice were not always properly observed and neonatal resuscitations equipment was not always available. There was significant overcrowding in the SCN. Although the current space was built decades ago for eight neonatal cots, more often there would be more than 15 newborn babies cramped in the same space at any one time, with 60–80 admissions per month. Hand washing is a major issue in the SCN, with only one hand wash basin for the ward and intermittent availability of running tap water and soap or alcohol for hand washing.
Most neonatal deaths occurred within early hours of the day, from 02:00 to 05:00. During this period, the night shifts have limited number of nurses on duty, between one and two nurses/nurse aids for the SCN with on-call RMO or registrar who would be called from home. There are no on-call rooms provided in the hospital for staff to stay or rest. The overwhelming nurse-to-patient ratio, sometimes 1 nurse to 20 patients, results in poor monitoring and nurses being tired and exhausted.
Communication was commonly identified as a modifiable factor that was amenable to improvement. This included communication and escalation from nurses and interns to registrars and consultants when children are critically ill to review and reassess. Initiatives arising through the audit process included better handing over of cases on the Children’s Ward by the day team to the on-call team. Lack of systems for managing the sickest children was identified, and plans for an intensive care section in the Children’s Ward to adequately monitor and treat severely ill patients were made.
The designation of deaths as not avoidable or potentially avoidable was decided by consensus after a thorough analysis of the cases and consideration of its modifiable factors. The decision was based on assessment of actual practice against standards, and a knowledge of the health resources available. However, we acknowledge the process is inherently subjective. We realised that many deaths occur because of an intersection of modifiable factors, from home, community to primary healthcare to referral hospital. Our child death reviews are now including more community-based modifiable factors which we identified commonly in the first 6 months (online supplementary appendix 5). Closer links with social and community services will be required for these modifiable social factors to be addressed, but we can at least start by systematically identifying these and bringing them to attention.
Improving on death auditing requires the following:
Formation of a quality improvement team to implement action plans and provide ongoing evaluation of the process.
Hospital management and ministry of health involvement for death audits to address modifiable factors outside a department, including within the community.
The process of death auditing should continually evolve and improve, aiming to reach the stage of implementing and evaluating changes. It should remain a simple process that is easily understood by clinical staff.
Standardisation of the cause of death classification (online supplementary appendix 3).
Inclusion of social risks and community-based modifiable factors (see online supplementary appendix 5).
Encouraging more nursing staff to attend and participate in the audits.
Sometimes auditing ‘near misses’ or complications as well as deaths.
A communication strategy to ensure lessons from the audits go to the clinical teams and other stakeholders.
Conclusion
Child death review meetings can be effective and educational, but it is an iterative and evolving process that needs a structure, tools, evaluation, and needs to be embedded in the culture of a hospital as part of overall quality improvement. A quality improvement team to implement action plans is vital. Our experience using adapted WHO tools and standards for audit has been positive, and with further experience lessons will continue to be learnt. Further research is needed on actions and outcomes following implementation of death reviews.
References
Footnotes
Contributors The study was designed by all authors. MS coordinated the child death review meetings and evaluation. TN and CT led the meetings. TD designed the audit tools in conjunction with WHO. MS and TD wrote the manuscript and all authors reviewed and contributed to the final version.
Funding This study was funded by the RE Ross Trust, Victoria, and grant number (2017 Pacific child health research grant).
Competing interests None declared.
Ethics approval The Board of Solomon Island National Research and Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.