Article Text

Abstract
Objective Investigate the effectiveness and cost-effectiveness of the Lightning Process (LP) in addition to specialist medical care (SMC) compared with SMC alone, for children with chronic fatigue syndrome/myalgic encephalitis (CFS/ME).
Design Pragmatic randomised controlled open trial. Participants were randomly assigned to SMC, or SMC plus the LP (SMC+LP). Randomisation was minimised by age and gender.
Setting Specialist paediatric CFS/ME service.
Patients Aged 12–18 years with mild/moderate CFS/ME.
Main outcome measures The primary outcome was the SF-36 physical function subscale (PFS) at 6 months. Secondary outcomes included the SF-36-PFS at 3 and 12 months, and pain, anxiety, depression, school attendance and cost-effectiveness from a health service perspective at 3, 6 and 12 months.
Results We recruited 100 participants between September 2010 and September 2013. We tested the feasibility of running the trial with a feasibility phase (29 September 2010 to 18 September 2012). The full trial was registered in June 2012 when we had determined it was a feasible study. Of the 100 participants, 51 were randomised to SMC+LP. Data from 81 participants were analysed at 6 months. Physical function (SF-36-PFS) was better in those allocated SMC+LP (adjusted difference in means 12.5 [95% CI 4.5 to 20.5], p=0.003) and this improved further at 12 months (15.1 [95% CI 5.8 to 24.4], p=0.002). At 6 months, fatigue and anxiety were reduced and at 12 months, fatigue, anxiety, depression and school attendance had improved in the SMC+LP arm. Results were similar following multiple imputation. SMC+LP was more cost-effective in the multiple imputation data set (difference in means in net monetary benefit at 12 months £1474 [95% CI £111 to £2836], p=0.03) but not for complete cases.
Conclusion The LP is effective and is probably cost-effective when provided in addition to SMC for mild/moderately affected adolescents with CFS/ME.
Trial registration number ISRCTN81456207.
- chronic fatigue syndrome
- adolescent health
- RCT
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
What is already known on this topic?
Paediatric chronic fatigue syndrome/myalgic encephalitis (CFS/ME) is relatively common with a negative impact on school, mood and quality of life.
Even with effective treatment, a significant number of children have not recovered at 6 months.
The Lightning Process (LP) is used by children with CFS/ME in the UK but with no evidence of effectiveness.
What this study adds?
At 6 months, children who received LP in addition to specialist medical care (SMC) had better physical function, fatigue and less anxiety.
At 12 months, children who received LP in addition to SMC had better fatigue, anxiety, depression and school attendance.
Adding LP is probably cost-effective but not all children wish to take part.
Introduction
Paediatric chronic fatigue syndrome (CFS) or myalgic encephalitis (ME) affects 0.57%–2.4%1–4 of children and is disabling with important impacts on mood,5 6 school attendance,4 7 8 quality of life9 and family functioning.10 It is defined as generalised fatigue causing disruption of daily life, persisting after routine tests, and investigations have failed to identify an obvious underlying cause.11 A minimum of 3 months of fatigue is required before the diagnosis can be made.12 On average, those affected miss a year of school overall and half are bedbound at some stage.13 14
There is a limited evidence base for treatment of paediatric CFS/ME.12 15 16 Three randomised trials have shown that cognitive–behavioural therapy (CBT) delivered individually,17 with biofeedback18 or via the internet19 is effective at 6 months compared with waiting list or usual medical care. All three studies reported improvements in fatigue, school attendance and a reduction in disability. Family-focused CBT appears to be as effective as psychoeducation in terms of school attendance at 6 months and recovery at 24 months.20 21 However, even with effective treatment, over a third of children19 20 have not recovered at 6 and 12 months20 21 and 21%21–36%22 are still unwell (eg, attending school less than 70% of the time) at 24 months. There is therefore an urgent need to find more effective treatments.
The Lightning Process (LP) is developed from osteopathy, life coaching and neurolinguistic programming and is used for a variety of conditions including CFS/ME. Clients read information, attend three group sessions and then receive follow-up phone calls.23 More than 250 children use LP for their CFS/ME each year in the UK (at a cost of ~£620 each), but there are no reported studies investigating its effectiveness, cost-effectiveness or side effects. Having shown that recruitment, randomisation and data collection were feasible and acceptable24 we conducted a randomised trial to investigate the effectiveness and cost-effectiveness of LP in addition to specialist medical care (SMC), compared with SMC alone, for children with CFS/ME.
Methods
Study design and participants
A detailed description of the study protocol has been reported.25 Between September 2010 and September 2013 we recruited participants after clinical assessment by the Bath/Bristol paediatric CFS/ME service, a large regional and national National Health Service (NHS) specialist service. We tested the feasibility of running this trial with a feasibility phase (29 September 2010 to 18 September 2012). We determined the trial was feasible in June 2012 and registered the full trial (31 July 2012). We applied for an amendment to recruit children into the full trial as opposed to a feasibility trial (see online supplementary table 1 for detailed description of amendments). Full trial first randomisation was on 19 September 2012. We continued seamlessly with participant recruitment without any interim between-group comparison of participant outcome data from the feasibility phase. Children from both phases (feasibility and full) were analysed. Children were diagnosed with CFS/ME after a thorough assessment which included screening for other disorders associated with fatigue.12 Baseline data were collected at this assessment. Children were eligible if they had CFS/ME, were aged 12–18, spoke English and were not housebound.
Supplementary file 1
Randomisation and masking
Allocation to trial arms was in equal proportions using minimisation by age (12–15/16–18 years) and gender, weighted towards minimising the imbalance in trial arms with probability 0.8. Allocation was concealed using a telephone-based interactive voice response system, created and maintained by the Bristol Randomised Trials Collaboration and accessed by the recruiting researcher. This was an open study: the randomised intervention was conveyed after obtaining consent, during the recruitment interview so that participants, parents, therapists and researchers were aware of treatment allocation. Data analyses were conducted using masked treatment codes.
Interventions
All participants were offered SMC12 which focused on improving sleep and using activity management to establish a baseline level of activity (school, exercise and social activity) which is then gradually increased. Sessions were delivered by a range of professionals including doctors, psychologists, physiotherapists and occupational therapists in family-based rehabilitation consultations. Follow-up sessions were either face to face or by telephone. The number and timing of the sessions were agreed with the family depending on each adolescent’s needs and goals. Those with significant anxiety or low mood were offered additional CBT. Participants could choose to use physiotherapist-delivered graded exercise therapy (GET), which provides detailed advice about exercise and focuses on an exercise programme rather than other activities.
Participants randomised to SMC+LP were asked to read information about LP and complete an assessment form with their parents to identify their goals and describe what they had learnt. They then had a telephone call with an LP practitioner (online supplementary appendix 1) to discuss attending an LP course consisting of three 4-hour sessions on consecutive days run with groups of two to five young people. Each had a theory session with taught elements on the stress response, how the mind and body interact and how thought processes can be either helpful or negative. This was followed by group discussion where the language used was discussed and in some cases challenged, and where participants were encouraged to think about what they could take responsibility for and change. In the practical session, participants identified a goal they wished to achieve (such as standing for longer) and were given different cognitive (thinking) strategies before and while the goal was attempted. They were also asked to identify a goal to attempt at home. After the course, young people were offered at least two follow-up phone calls with an LP practitioner.
Outcomes
The primary outcome was the SF-36 physical function subscale (SF-36-PFS)26 analysed as a continuous variable collected at 6 months after randomisation. We chose the SF-36 based on qualitative work conducted in the feasibility phase of the study.24 We have reported that parents and participants ‘commented that the school attendance primary outcome did not accurately reflect what they were able to do, particularly if they were recruited during, or had transitioned to, A levels during the study.’ In addition, ‘we were aware of some participants who had chosen not to increase school attendance despite increased activity.’ We therefore concluded that: ‘trials involving 17 and 18 year olds should consider alternative primary outcome measures to school attendance as it is difficult to assess for those transitioning from General Certificate of Secondary Education to A levels, and may not be appropriate for those who do not consider school attendance their primary goal.’ At this stage, our recommendation was that a ‘full study uses other primary outcomes, such as the SF-36 or the Chalder Fatigue Scale and uses school attendance as a secondary outcome.’ These findings informed our application for our ethical amendment to a full study in 2011 (see online supplementary table 1) and were published in our feasibility paper in 2013.24
Qualitative interviews with Specialist Medical Intervention and Lightning Evaluation (SMILE) participants then formed part of a larger study which described the conceptual model for paediatric CFS/ME.27 In this study, physical activity (or disability) is described by children as being pivotal because of the impacts on social participation and emotional well-being. While school was deemed to be an important contextual factor, these qualitative results led us to choose the SF-36-PFS as a primary outcome with school attendance as a secondary outcome. There was no analysis of any outcome data during or after the feasibility phase until the entire trial was completed.
Secondary outcomes were the SF-36-PFS at 3 and 12 months, and school attendance (days per week), the Chalder Fatigue Scale,28 pain (visual analogue scale), Hospital Anxiety and Depression Scale (HADS),29 Spence Children’s Anxiety Scale (SCAS)30 and quality-adjusted life-years (QALY, derived from the EQ-5D-Y)31 at 3, 6 and 12 months. At 3, 6 and 12 months parents completed an adapted four-item Work Productivity and Activity Impairment: General Health questionnaire (V2.0)32 and a resource use questionnaire assessing their child’s health service use (eg, general practitioner or specialist care), educational service use (eg, school counsellor), health-related travel and other family costs.
Time windows for questionnaire return were prespecified as 6 weeks after the 3-month follow-up, 6 weeks before or up to 3 months after the 6-month follow-up, and 3 months before or after the 12-month follow-up. Those who had not responded within 1 week were sent a reminder letter with a reduced set of questionnaires (SF-36-PFS, Chalder Fatigue Scale and school attendance). From February 2011 non-responders were telephoned by a researcher and the SF-36-PFS and Chalder Fatigue Scale were completed over the phone to improve follow-up rates.
Sample size
A consensus definition for a small clinically important difference on the SF-36-PFS at 6 months’ follow-up is 10 points.33 However, we did not want to miss a smaller but still potentially important effect of as low as 8 points. To detect a between-group difference of 8–10 points with 90% power, 1% two-sided significance and SD of 10 requires between 32 and 50 participants per group for analysis. Allowing for 10%–20% non-collection of primary outcome data, we aimed to recruit between 80 (32*2/0.8) and 112 (50*2/0.9) participants.
Statistical analysis
The statistical analysis plan was agreed by the study management group and published on our website prior to analyses. The primary analysis compared mean SF-36-PFS scores at 6 months according to randomised allocation among participants with measured outcomes, using multivariable linear regression adjusting for baseline values of the outcome, baseline age and gender. Similar regression analyses were conducted for secondary outcomes. Sensitivity analyses of the primary outcome adjusted for variables for which there was baseline imbalance; excluded those recruited up to 31 January 2011 preceding the protocol amendment to allow collection of follow-up data by phone; and used multiple imputation of missing data. Missing items in partially completed scales (Chalder Fatigue and SF-36-PFS) or subscales (SCAS and HADS anxiety and depression) were imputed using the mean of completed items, if only one item (or two for the SCAS subscales) was missing. If more items were missing the whole scale or subscale was scored as missing. We conducted a repeated measures analysis using all follow-up SF-36-PFS scores, with and without an interaction between allocation arm and time, to investigate whether between-group differences remained constant over time. We did not analyse 3-month outcomes except in this repeated measures analysis for SF-36-PFS as these were unlikely to be informative since the primary follow-up was at 6 months. We estimated the complier average causal effect (CACE) using instrumental variables linear regression estimated via the generalised method of moments, of LP among compliers, defined as participants in the SMC+LP arm who completed all of the LP course.
Prespecified subgroup analyses explored differences in treatment effect according to baseline age (<15 vs 15–17), gender, severity (none vs some school attendance at baseline) and comorbid anxiety (>12 or ≤12 on the HADS anxiety subscale) for the primary outcome, by adding an interaction term to the primary analysis multivariable linear regression model.
Health economic analyses
We conducted a cost-utility analysis of SMC+LP from the health service and public sector perspective. We estimated the incremental net monetary benefit (iNMB) of SMC+LP versus SMC, at a threshold willingness to pay of £20 000 (~US$30 000) per QALY.34 In the primary analysis, we used the cost of LP charged to the trial (mean £567). In sensitivity analyses we: (1) used the price of LP outside of trial (£620; July 2014 price); and (2) estimated cost of providing the LP intervention within the UK health service (online supplementary table 2). SMC outpatient attendances were extracted from hospital records. Other healthcare use was based on parent report. Resource use was combined with 2013 unit costs (online supplementary table 2).35–38 In the absence of a paediatric valuation for the EQ-5D-Y, we used the UK adult tariff.39 QALYs were estimated using the area under the curve.40 Incremental costs, QALYs and net benefits were adjusted for baseline values, age, gender and for variables where there was baseline imbalance. Non-parametric bootstrapping methods were used to calculate normally distributed 95% CIs around the iNMB. The probability that SMC+LP is cost-effective at varying willingness-to-pay thresholds was estimated using a cost-effectiveness acceptability curve. Where one item of the EQ-5D-Y was missing (n=3), the mean of the other domains (rounded to the nearest integer) replaced the missing value. A high proportion of participants had missing resource use data at 3, 6 and 12 months. Therefore, we conducted two analyses based on the complete case and multiply imputed data sets (online supplementary appendix 2).
All analyses were conducted using Stata (StataCorp. 2013. Stata Statistical Software: Release 13.1. College Station, TX: StataCorp).
Results
Of 657 children assessed in the specialist CFS/ME clinic during the recruitment period, 631 were assessed for study eligibility and 310 were eligible (figure 1). Among those eligible 136 consented to receiving further information and 100 were randomised: 49 to SMC only and 51 to SMC+LP. Fifty-six of these participants were included in the report of whether it was feasible to conduct this randomised controlled trial.24 Recruitment was stopped after the 100th participant was randomised. Eligible children and adolescents who found out more about the trial but were not randomised had lower anxiety and depression scores and attended more school (online supplementary table 3). Participants’ mean age was 14 years, 76 were female and all described themselves as British. Participants were disabled by their fatigue: only seven were attending full-time school and 47 described themselves as attending 2 days or less school a week.

Specialist Medical Intervention and Lightning Evaluation (SMILE): Consolidated Standards of Reporting Trials (CONSORT) trial profile. CFS, chronic fatigue syndrome; LP, Lightning Process; PFS, physical function subscale; SMC, specialist medical care.
Participants’ characteristics at baseline were balanced between arms except for pain and anxiety (SCAS) scores (table 1), which was adjusted for in sensitivity analyses. The imbalance in pain and SCAS scores were in opposite directions suggesting that the two arms were not systematically different. Five participants withdrew from the study: two from the SMC and three from the SMC+LP arm. Outcome data were collected from 92 participants on at least one follow-up occasion. Baseline characteristics were similar between those who did (n=82) and did not (n=18) provide primary outcome data at 6 months (online supplementary table 4). The mean (SD) time between clinical assessment and primary outcome collection was 6.8 (1.0) and 6.8 (0.7) months in the SMC and SMC+LP arms, respectively. Treatment as allocated was received by 46 (94%) and 39 (76%) participants in the SMC and SMC+LP arms, respectively. Three participants (3/39, 8%) in the SMC+LP arm received the LP course after completing the 6-month follow-up, these participants were included in the analyses.
Characteristics of the randomised participants at baseline
Mean SF-36 physical function improved more over time in participants allocated to SMC+LP than in those allocated to SMC (figure 2). Participants allocated to SMC+LP had better physical function at 6 months than those allocated to SMC (table 2, adjusted difference in means 12.5 [95% CI 4.5 to 20.5], p=0.003). This difference increased to 15.1 (95% CI 5.8 to 24.4, p=0.002) at 12 months. These differences were similar when additionally adjusted for baseline anxiety (SCAS) and pain (VAS), when analyses were restricted to participants recruited from February 2011, and with multiple imputation of missing data (table 2). The average between-arm difference in physical function across both 6 and 12 months’ follow-up was 14.4 (95% CI 7.3 to 21.5, p<0.001). When compliance was taken into account using CACE analyses, the estimated effect of LP at 6 and 12 months was increased compared with the intention to treat (ITT) estimate (table 2). There was little evidence that the effect of LP+SMC compared with SMC on the primary outcome differed according to baseline age, anxiety or school attendance (all interaction p>0.3). There was weak evidence (online supplementary table 5) that the effect in males (adjusted difference in means 26.6 [95% CI 8.9 to 44.3]) was greater than that in females (adjusted difference in means 9.0 [95% CI 0.2 to 17.8]) with an interaction p value of 0.08.
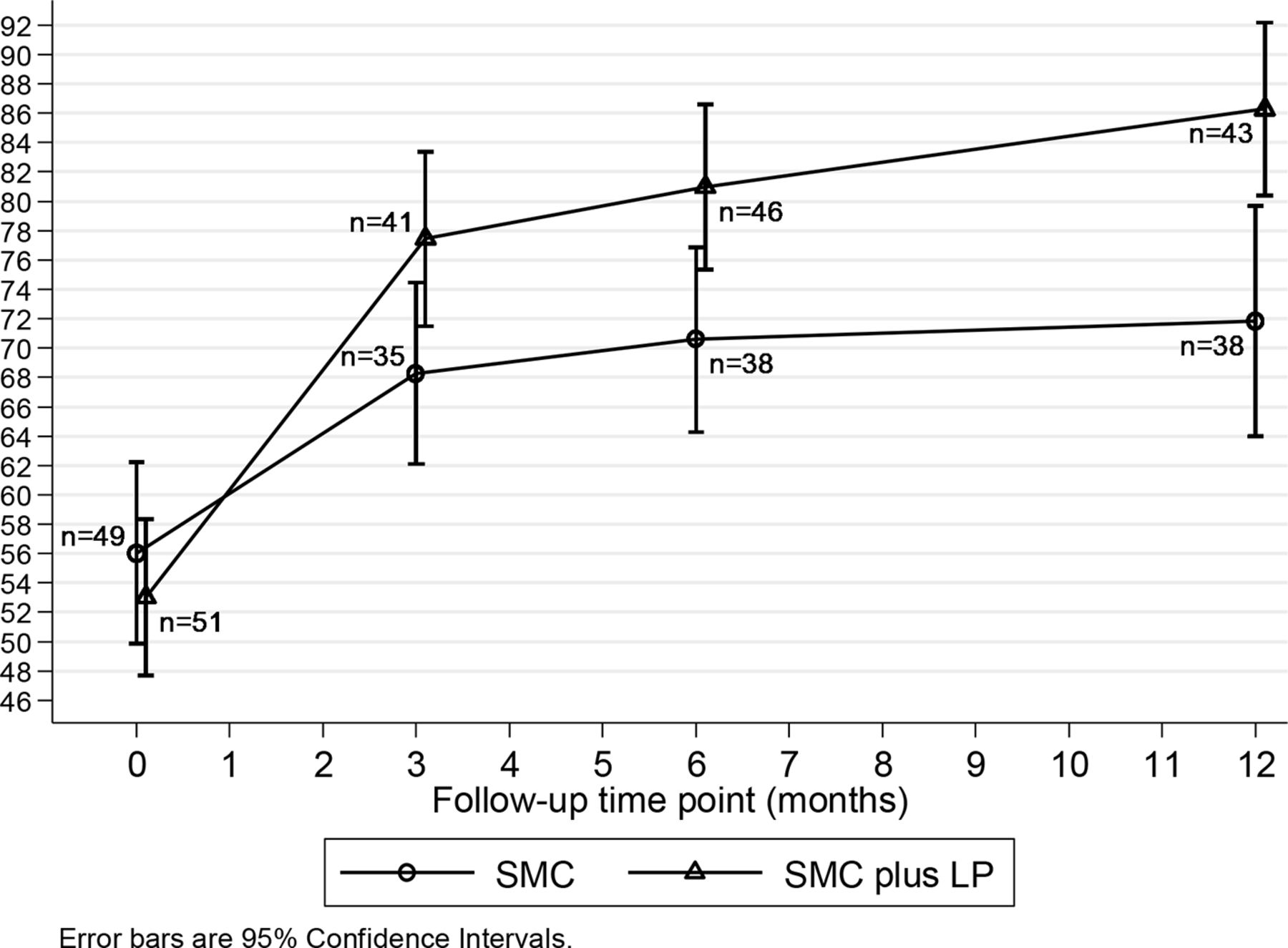
Mean SF-36 physical function over time. LP, Lightning Process; SMC, specialist medical care.
Primary outcome
Participants in the SMC+LP arm had less fatigue (adjusted difference in means −4.7 [95% CI −7.9 to −1.6], p=0.003) (table 3) than those allocated to SMC and a greater improvement in anxiety symptoms measured by both the HADS (−3.3 [95% CI −5.6 to −1.0], p=0.005) and the SCAS (−8.7 [95% CI −16.9 to −0.5], p=0.04) scores at 6 months. The difference in means in fatigue score and HADS anxiety score was smaller at 12 months (−3.2 [95% CI −6.3 to −0.1] and −2.8 [95% CI −4.7 to −0.8], respectively). However, the difference in means in SCAS anxiety was greater at 12 months (−12.1 [95% CI −20.1 to −4.1]) and there was evidence that there was less depression among participants allocated to SMC+LP than those allocated to SMC at 12 months (adjusted difference in means in HADS depression score −1.7 [95% CI −3.3 to −0.2], p=0.03). Participants allocated to SMC+LP had better school attendance at 12 months than those allocated to SMC (adjusted difference in means 0.9 days of school per week [95% CI 0.2 to 1.6], p=0.02). Mean pain scores were lower in participants allocated to SMC+LP compared with those allocated to SMC at both 6 and 12 months, but CIs were wide.
Secondary outcomes
Five adverse events were reported (three in the SMC+LP arm). Four were related to participants and one to a parent. None were attributed to either SMC or LP. Physical function at 6 months deteriorated in nine participants, of whom eight were in the SMC arm. Five of the nine had deterioration of ≤10 on the SF-36-PFS (range 0–100) which is less than the minimal clinically important difference (MCID).
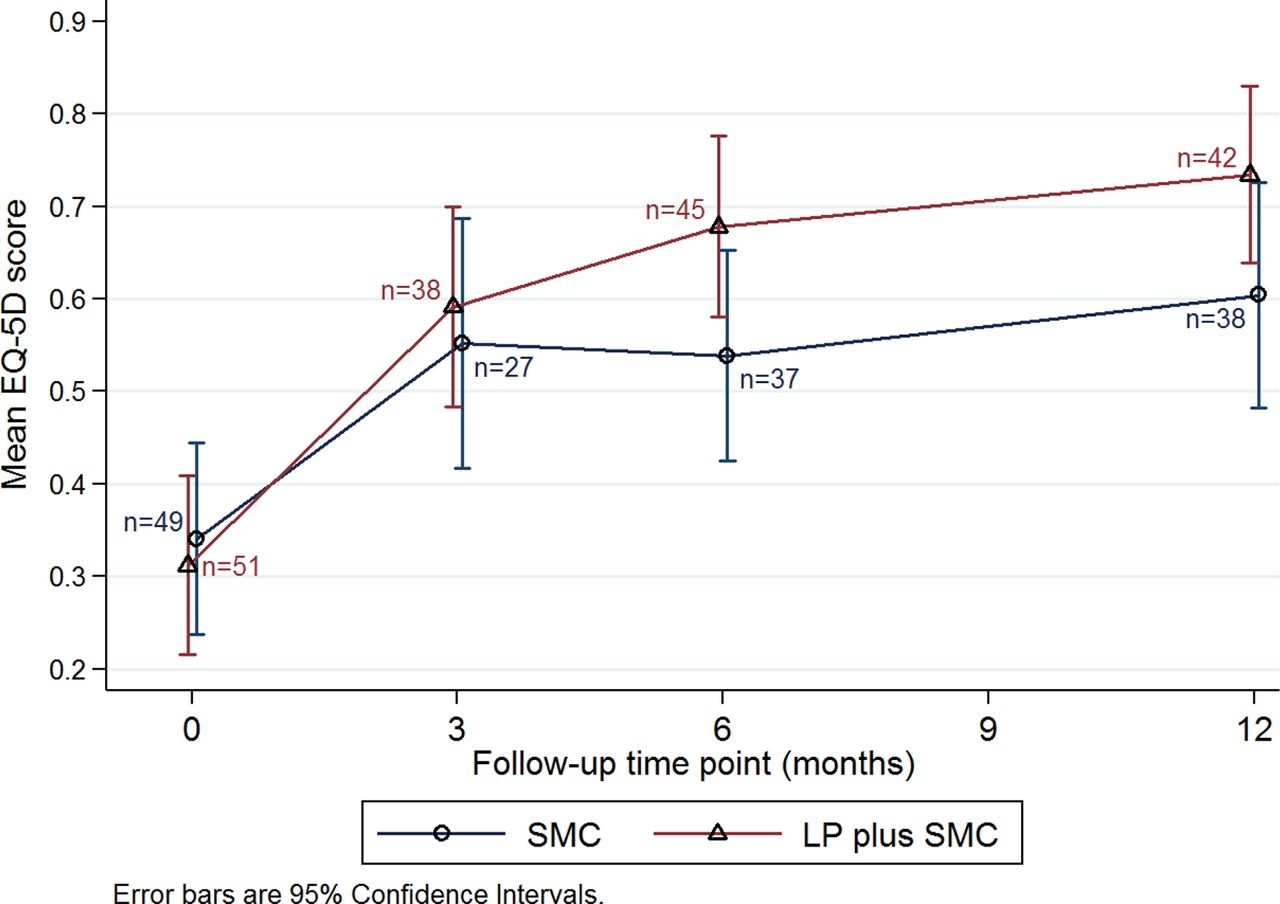
EQ-5D-Y questionnaires were completed by 65, 82 and 80 participants at 3, 6 and 12 months, respectively (figure 3); 56 completed EQ-5D-Y at all three follow-up time points. EQ-5D-Y scores were generally higher in the SMC+LP group. Differences in QALYs were evident at 12 months in the multiple imputation data set (table 4, adjusted difference in means 0.095 QALYs [95% CI 0.030 to 0.160], p=0.004), but in the complete case data set the CI included zero (adjusted difference in means 0.080 QALYs [95% CI −0.064 to 0.225], p=0.3).

Mean EQ-5D scores, by treatment group. LP, Lightning Process; SMC, specialist medical care.
Analysis of multiple imputation and complete case data of total HC+LP costs and QALYs and NMB (£20 000) at 6 and 12 months; by treatment group, all adjusted for baseline value, age, sex, baseline SCAS and baseline VAS
Complete healthcare use questionnaires were returned by 56 participants at 3 and 6 months and 55 at 12 months, but only 30 participants completed these questionnaires at all three time points. The initial cost of LP was not fully offset by marginally lower costs of other care over the 12-month period. The incremental cost (table 4) of SMC+LP was higher in both complete case (difference in means £445 [95% CI −57 to 947], p=0.08) and multiple imputation data sets (difference in means £390 [95% CI 189 to 591], p<0.005).
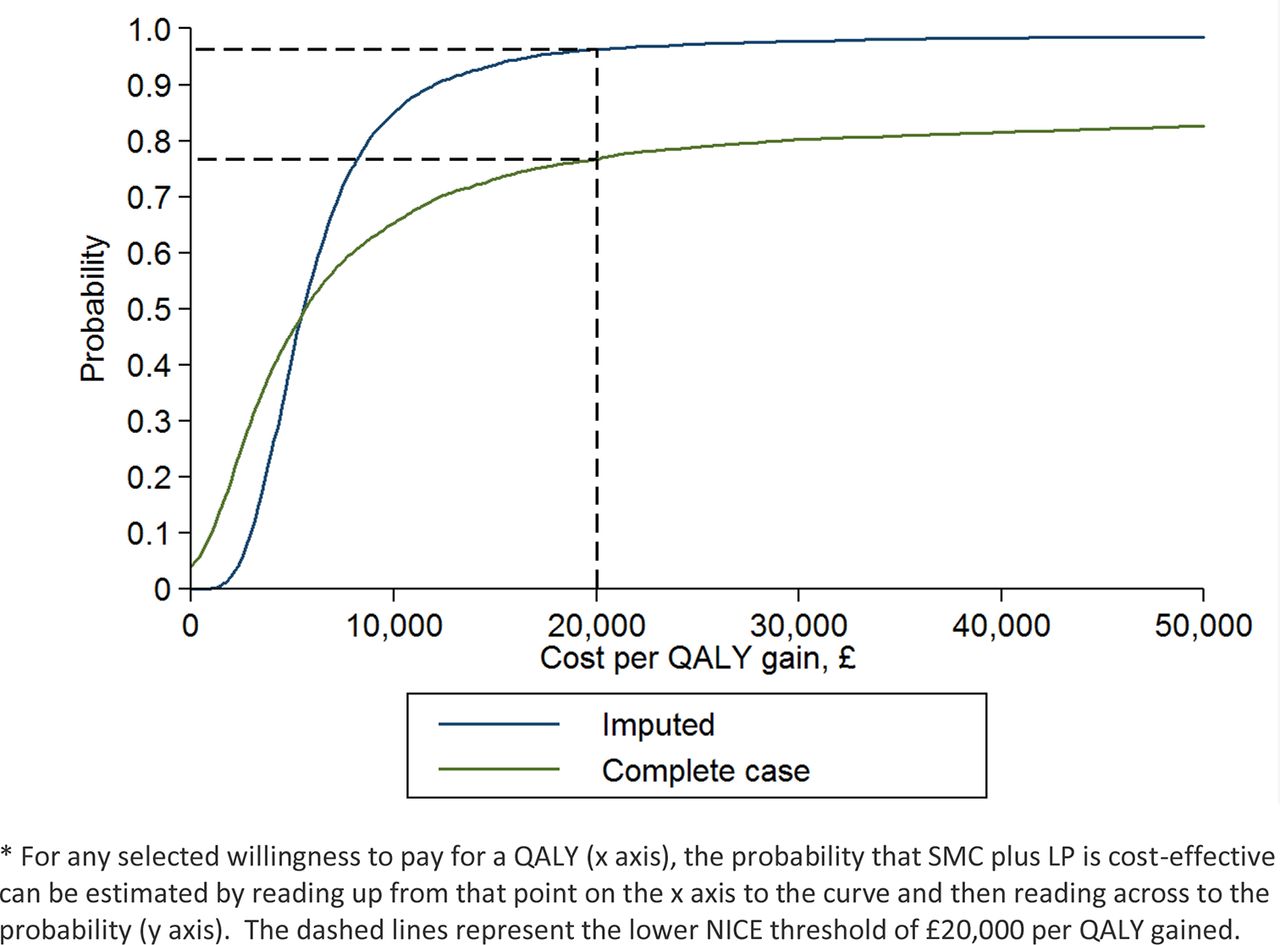
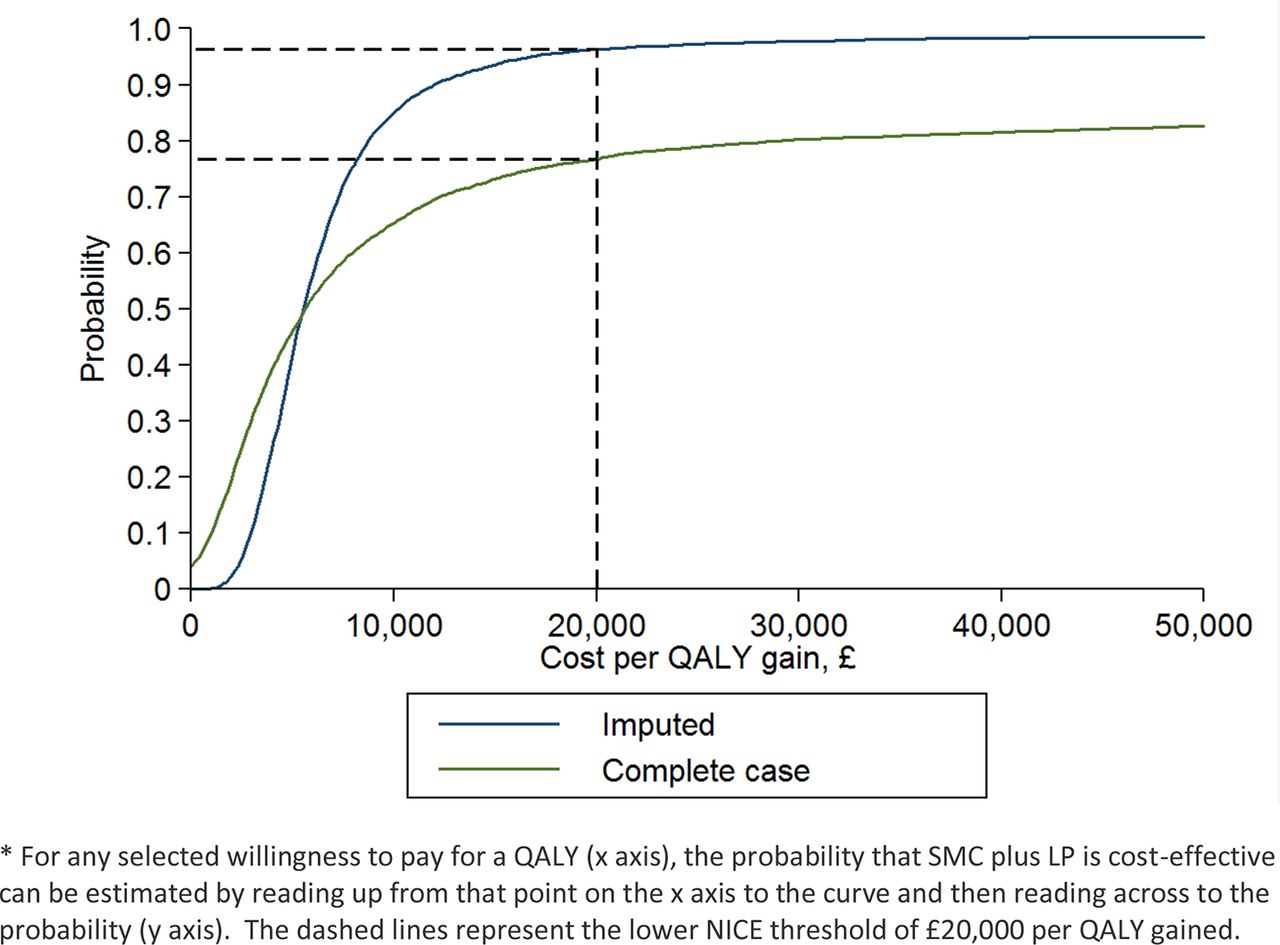
Table 4 shows that in the multiple imputation data set there was good evidence that SMC+LP was more cost-effective than SMC alone (iNMB £1508 [95% CI £148 to £2869], p=0.03), although the evidence was much weaker in the complete case data set (figure 4, online supplementary table 6). Sensitivity analyses varying the unit cost of LP treatment made no difference to this conclusion (online supplementary table 7). Sensitivity analyses assuming costs and QALYs are not missing at random40 reduced the strength of the evidence that SMC+LP was likely to be cost-effective, but did not alter the conclusion.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cost-effectiveness acceptability curves* based on complete case and multiply imputed estimates of incremental costs and QALYs of SMC plus LP at 12 months. LP, Lightning Process; NICE, National Institute for Health and Care Excellence; QALY, quality-adjusted life-years; SMC, specialist medical care.
Discussion
This is the first randomised trial investigating the effectiveness of the LP for any condition. It is the first trial that has demonstrated the effectiveness of an intervention other than CBT for paediatric CFS/ME. Addition of the LP to SMC improved physical function at 6 months in adolescents with CFS/ME and this difference increased at 12 months. The addition of LP also improved fatigue and anxiety at 6 months and fatigue, anxiety and depression at 12 months. Participants in the LP arm were attending 1 day more of school a week at 12 months on average. The initial cost of LP was not fully offset by lower subsequent costs of healthcare, but the improvements in health-related quality of life meant that SMC+LP is probably cost-effective using a threshold for a QALY of £20 000 (~US$30 000). Participants in the SMILE trial did not have any serious adverse events attributable to either treatment arm. The majority of those who experienced a deterioration in physical function had a deterioration of ≤10 on the SF-36-PFS. The lack of serious adverse events is consistent with other treatment trials in CFS/ME.41
Strengths of the study include its randomised design and follow-up for 12 months. Participants received SMC that is currently being delivered in the UK Health Service by a multidisciplinary team, and the LP as it is currently provided. More participants were lost to follow-up in the SMC arm, but baseline characteristics were similar in those followed and not followed up. Complete healthcare use questionnaires were returned by only 55 or 56 participants at each time point. We used multiple imputation to correct for potential bias due to missing data and conducted sensitivity analyses restricted to participants recruited after the protocol changed to collect primary outcome data by telephone, which improved follow-up rates suggesting results were robust. We predefined the clinically important difference (10 points) on the SF-36-PFS and the difference in means was greater than this at both 6 and 12 months. The study was not blinded, so that patient-reported outcomes may have been affected by participants’ knowledge of the group to which they were randomised. We did not have capacity to check school attendance using school records, but this could have provided an objective outcome. Further unpublished work suggests this is highly correlated with the self report measure we used. Only 36 (70%) of those allocated LP attended the full course prior to the 6-month follow-up but we estimated the effect in all those who completed the full LP course. The study was originally planned as a feasibility study and although randomised was not registered on a trial registry, since the aim was to investigate feasibility rather than effectiveness of the intervention. After establishing feasibility, we applied to register the full trial in June 2012. At this time, the results of our feasibility work suggested we could use either SF-36-PFS or Chalder Fatigue Scale or both which we registered as primary outcomes. We decided to use just the SF-36-PFS and published this in 2013 and in our analyses plan. We did not update the ISTCRN site until 2018, however, we uploaded the relevant publications in 2016 and the study website had the updated analyses plan.
The LP may not be suitable for all children and adolescents. Fewer than 30% of eligible children were randomised. We do not know why the majority did not want to take part in the trial but it may be because they did not want to take part in groups or travel for 3 consecutive days. We felt it would be unethical to have a control group without treatment and therefore we only know that LP is effective in addition to SMC and not whether it is effective on its own. We only recruited children aged 12 and over who were not housebound and who spoke English. We do not know whether LP is effective, acceptable or feasible for those who are severely affected, less than 12 years old, or do not speak English. The study was registered after demonstrating feasibility. The analysis includes participants who were recruited prior to registration of the study. This does not comply with ICMJE and BMJ guidance on trial registration. The reasons for this have been explained in the paper.
Participants in both treatment arms improved. Those receiving SMC alone had a mean improvement that was similar to that seen in adults receiving CBT or GET.41 The improvement in SF-36-PFS in those receiving SMC+LP is consistent with those receiving treatment in previous paediatric trials investigating both family-based and individual CBT.17 20 We predefined the MCID as 10 points on the SF-36-PFS based on consensus statements. Subsequent work by our team has shown that this is a clinically significant change in physical function for children with CFS/ME.42 Ten points equates to a minimum of two step changes on the SF-36-PFS. This can be either one-step change on two questions, or two-step changes on one question. The SF-36 asks: ‘Does your health limit you in these activities? If so, how much?’ As an example, one-step change could be: ‘Yes, limited a lot’ to ‘Yes, limited a little’ or ‘Yes, limited a little’ to ‘No, not limited at all’ to different questions such as ‘climbing several flights of stairs’ or ‘walking 100 yards’ or ‘walking half a mile’. The participants in our study who received SMC only did not improve as much as other trials investigating CBT17 20 which may be because on average they had less than half the number of treatment sessions.
Participants in the SMC+LP arm maintained or increased improvements compared with SMC alone at 12 months and this was true for both the ITT and the CACE analyses. This is in contrast to previous trials investigating internet-based CBT where the treatment effects were sustained but the difference between the two trial arms was reduced at 12 months compared with 3 months,19 22 and family-focused CBT versus psychoeducation where treatment differences at 3 months were not maintained at 6 or 12 months.20
There is only one study23 investigating LP which used qualitative interviews to explore the views of nine 14–26 year-olds about their experiences. The main difference between LP and CBT appears to be the emphasis placed on physiological responses and causal attributions23 but we do not know whether these explain the greater effectiveness of LP. We do not know which aspects of the LP are the most important or helpful. Some young people who received LP value the theory, others the practical sessions or the homework.23 Further research is needed to understand why LP improves outcomes at 6 and 12 months and which aspects of the LP contribute to its effectiveness.
Conclusions
The addition of the LP to SMC may be helpful to children with CFS/ME. However, this study needs to be replicated before the LP should be offered in the NHS.
Supplementary file 2
![[archdischild-2017-313375supp002.jpg]](https://adc.bmj.com/content/archdischild/103/2/155/DC2/embed/inline-supplementary-material-2.jpg?download=true){kind=link}
Supplementary file 3
Acknowledgments
We are grateful to all the children and families who took part in this study and to the Bath specialist CFS/ME service who recruited them. We thank Kate White, Anu Ganupathy and Debbie Johnson who helped with data collection and recruitment during the study. We are grateful to Phil Parker and the LP central office who provided advice and information on costs.
References
Footnotes
Correction notice This is a republished, corrected version. For full details please see the correction note, 10.1136/archdischild-2017-313375corr1.
Contributors EMC obtained the funding, and designed and supervised the trial. DMG conducted the statistical analysis and compiled the results tables. KG conducted the health economic analyses and compiled the health economic tables. WH contributed to the study design and supervised the health economic analyses. JACS and AAM contributed to the study design and cosupervised the statistical analyses. LB contributed to the study design and running the trial. SMC managed the data and contributed to the statistical analyses. NM contributed to the study design. All authors contributed to the data interpretation and writing the paper. EMC is the guarantor. The authors had access to all the data. The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Funding This trial was funded by the Linbury Trust (grant number LIN2038) and the Ashden Trust (grant numbers ASH1062, 1063, 1064). EMC was funded by an NIHR Clinician Scientist Fellowship followed by an NIHR Senior Research Fellowship (SRF-2013-06-013) during the trial. SMC was funded by an NIHR Postdoctoral Fellowship during the analyses of the trial.
Disclaimer No member of the LP team had any involvement in the analyses or in writing the paper. No member of the Linbury Trust or the Ashden Trust had any involvement in the design, analyses or in writing the paper. This report is an independent research and the views expressed in this publication are those of the authors and not necessarily those of the NHS, the National Institute for Health Research or the Department of Health. The funders and the sponsor of the study had no role in the design and conduct of the study; collection, management, analysis and interpretation of the data; preparation, review or approval of the manuscript; and decision to submit the manuscript for publication. All researchers involved in this study were independent from both the funders and the sponsor.
Competing interests Financial support for the submitted work was received from the Linbury Trust and the Ashden Trust. EMC and SMC have received fellowship grants from the NIHR. JACS has received grants from the NIHR. EMC runs the specialist CFS/ME service at Royal United Hospital NHS Foundation Trust, has received one grant from MRC, one grant from the NIHR and is a medical advisor to the Sussex and Kent ME/CFS Society. The authors declare they did not receive any funding from the Lightning Process.
Ethics approval A favourable ethical opinion was given on 8 September 2010 (reference 10/H0206/32) by South West 2 Local Research Ethics Committee. Two favourable opinions were provided for amendments to study documents and protocol on 31 May 2011 and 6 September 2012.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Given the nature of this data set, access is controlled. Requests are referred to the University of Bristol Data Access Committee (DAC) for approval before data can be released under an appropriate data access agreement. For details on how to access data please see the repository record at http://dx.doi.org/10.5523/bris.1myzti8qnv48g2sxtx6h5nice7.
Linked Articles
- Atoms
- Correction
- Correction