Article Text

Abstract
Background The BCG vaccine is administered to protect against tuberculosis, but studies suggest there may also be non-specific beneficial effects upon the infant immune system, reducing early non-targeted infections and atopic diseases. The present randomised trial tested the hypothesis that BCG vaccination at birth would reduce early childhood hospitalisation in Denmark, a high-income setting.
Methods Pregnant women planning to give birth at three Danish hospitals were invited to participate. After parental consent, newborn children were allocated to BCG or no intervention within 7 days of age. Randomisation was stratified by prematurity. The primary study outcome was number of all-cause hospitalisations analysed as repeated events. Hospitalisations were identified using The Danish National Patient Register. Data were analysed by Cox proportional hazards models in intention-to-treat and per-protocol analyses.
Results 4184 pregnant women were randomised and their 4262 children allocated to BCG or no intervention. There was no difference in risk of hospitalisation up to 15 months of age; 2129 children randomised to BCG experienced 1047 hospitalisations with a mean of 0.49 hospitalisation per child compared with 1003 hospitalisations among 2133 control children (mean 0.47), resulting in a HR comparing BCG versus no BCG of 1.05 (95% CI 0.93 to 1.18) (intention-to-treat analysis). The effect of BCG was the same in children born at term (1.05 (0.92 to 1.18)) and prematurely (1.07 (0.63 to 1.81), p=0.94). The effect was also similar in the two sexes and across study sites. The results were essentially identical in the per-protocol analysis and after adjustment for baseline characteristics.
Conclusions BCG vaccination at birth did not reduce the risk of hospitalisation for somatic acquired disease until 15 months of age in this Danish study population.
Trial registration number NCT01694108, results.
- Bacillus Calmette-Guérin (BCG
- hospitalisation
- infant
- vaccine
- non-specific effect
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
What is already known on this topic?
BCG is the primary prophylaxis against tuberculosis.
BCG is among the most widely used vaccines globally.
There may be non-specific beneficial effects of neonatal BCG vaccination upon the infant immune system, reducing early infections and atopic disease.
What this study adds?
BCG vaccination did not reduce the risk of hospitalisation for acquired somatic disease during the first 15 months of life in a Danish study population.
Background
BCG, primary prophylaxis against tuberculosis, is among the most widely used vaccines globally.1 Randomised controlled trials indicate that the live attenuated BCG vaccine against tuberculosis may have beneficial ‘non-specific’ or ‘heterologous’ effects on the infant immune system, reducing non-tuberculosis neonatal mortality in low-income settings by reducing severe early infection.2 ,3 The association between BCG and childhood morbidity, primarily atopic disease has been studied with conflicting results.4 The only randomised trial so far among 121 newborns with high risk of atopy found BCG to be associated with a significant reduction in the use of medication for eczema.5 From 1979, routine BCG vaccination at school start was gradually discontinued in Denmark due to low prevalence of tuberculosis. If BCG has beneficial non-specific effects on health also in high-income settings, stopping routine BCG may have deprived children of these beneficial effects. We therefore conducted a large-scale randomised trial in Denmark to test the effect of BCG given at birth on childhood morbidity, including hospitalisation, infections, atopic disease, growth, development and immunological indicators. The present paper presents the effect of BCG on the primary outcome, all-cause hospitalisation from birth to 15 months of age. We hypothesised that BCG vaccination at birth would reduce all-cause hospitalisation by 20%.
Methods
Setting, study population
The procedures of The Danish Calmette Study were published in details elsewhere.6 Briefly, pregnant women planning to give birth at three Danish hospitals were invited. Inclusion criteria were gestational age of 32+ weeks, birth weight of 1000+ grams and a signed informed consent from the parents. Exclusion criteria were maternal intake of immunomodulating medicine during pregnancy, signs of severe illness or major malformation in the infant and no Danish-speaking parent due to concerns about language barrier. Newborns were allocated 1:1 to standard BCG vaccination with the Danish strain 1331, or no intervention within 7 days of birth. The children were allocated 1:1 in permuting blocks of 2-4-6 using an online system. Since in prior studies the strongest non-specific effects on mortality have been seen among the smallest newborns,2 ,3 the allocation was stratified by prematurity defined as gestational age <37 weeks. The allocation was planned stratified also by sex and study site; however, by programme error the allocation was stratified only by prematurity. Parents were not blinded to allocation since the local inflammatory reaction caused by BCG vaccination could not be mimicked, but the parents were asked not to disclose if the child had received BCG to keep study staff blinded during the data collection.
Follow-up
The primary outcome was all-cause hospitalisations. Since the measles-mumps-rubella vaccine (MMR) may also have non-specific effects, follow-up was censored at 15 months of age where MMR is scheduled in the Danish national vaccination programme.7 ,8
All Danish residents have a unique identification number, which was used to obtain information from The Danish National Patient Register on acquired, somatic all-cause hospitalisation, including dates of admission and discharge and categorised by the International Classification of Diseases V.10 (ICD10) diagnosis codes.9 ,10 Outpatient and emergency department hospital contacts not leading to admission, and hospitalisations starting before or at the date of randomisation were excluded. Since the study aimed to examine if BCG reduced acquired somatic morbidity, diagnostic codes due to administrative procedures, admission to the maternity ward in connection with the delivery, congenital and birth-related conditions, psychiatric disease, and injuries were excluded (ICD10-specification in the online supplement).
Supplemental material
Furthermore, follow-up consisted of telephone interviews and clinical examinations at 3 months and 13 months of age; secondary outcomes and adverse events will be published separately.
Power calculation
Sample size estimates were based on 95% CIs and a 90% power. Twenty per cent of the child population in Denmark was expected to be hospitalised during the first 15 months of life.11 To detect a 20% reduction in hospitalisations during the first 15 months of life, 3972 newborns needed to be included. We expected a very small loss to follow-up in the registry-based studies and aimed to include approximately 4300 newborns.
Statistics
Cox proportional hazards models were used to estimate the HR of all-cause hospitalisation between the BCG and control groups. Adjustment for recurrent hospitalisations for each child was done using robust SEs for the estimated HRs. The results are presented as HRs with 95% CIs and corresponding p values. The children were censored at migration, 15 months of age or death, whichever came first. The analyses were stratified by prematurity in accordance with the randomisation procedure. In the main ‘intention-to-treat (ITT) analysis’ hospitalisations within the period from randomisation to 15 months of age were analysed according to randomisation group. We also conducted a ‘per-protocol (PP) analysis’ in which children who did not follow the allocation were excluded and hospitalisations from time since vaccination for the BCG group and time since randomisation for controls was included. Curves for mean number of hospitalisations by randomisation arm as a function of time since randomisation were estimated using the Nelson-Aalen method. Further, we tested the effect of BCG on time to first hospitalisation.
Secondary analyses
Using Cox models, we tested if adjustment for baseline characteristics changed the estimates. Since previous studies indicate that the non-specific effects of one vaccine may be modified by a subsequent different vaccination,12 follow-up was divided into 0–2 months (0–89 days) while the children had received BCG or nothing, and 3–15 months (90–456 days) when the children should have received one to three doses of diphtheria, tetanus, acellular pertussis, polio, Haemophilus influenzae type b and Streptococcus pneumonia vaccine according to the routine vaccination programme.8
We also estimated potential effect modification by caesarean section, administration of antibiotics to the mother during delivery, birth weight <2500 g, ≥one sibling, atopic disposition, vaccination ≤2 days of age, maternal BCG vaccination and by the two vaccine batches used in the study. The analysis by batch was adjusted for calendar months.
All analyses were performed using Stata V.13 (StataCorp LP, Texas, USA).
Results
Randomisation and baseline
At the three hospitals 16 521 pregnant women were invited. No response was given by 6148 families, and 6189 families were excluded primarily because they declined participation after being informed verbally about the study (figure 1). Four thousand one hundred and eighty-four pregnant women were randomised and their 4262 children allocated to BCG or no intervention (figure 1). Baseline characteristics with potential influence on childhood morbidity did not differ between the two allocation groups except for ethnicity other than Danish and smoking, which were more common in families of control children (table 1).
Baseline characteristics by allocation among 4184 Danish mothers in The Danish Calmette Study
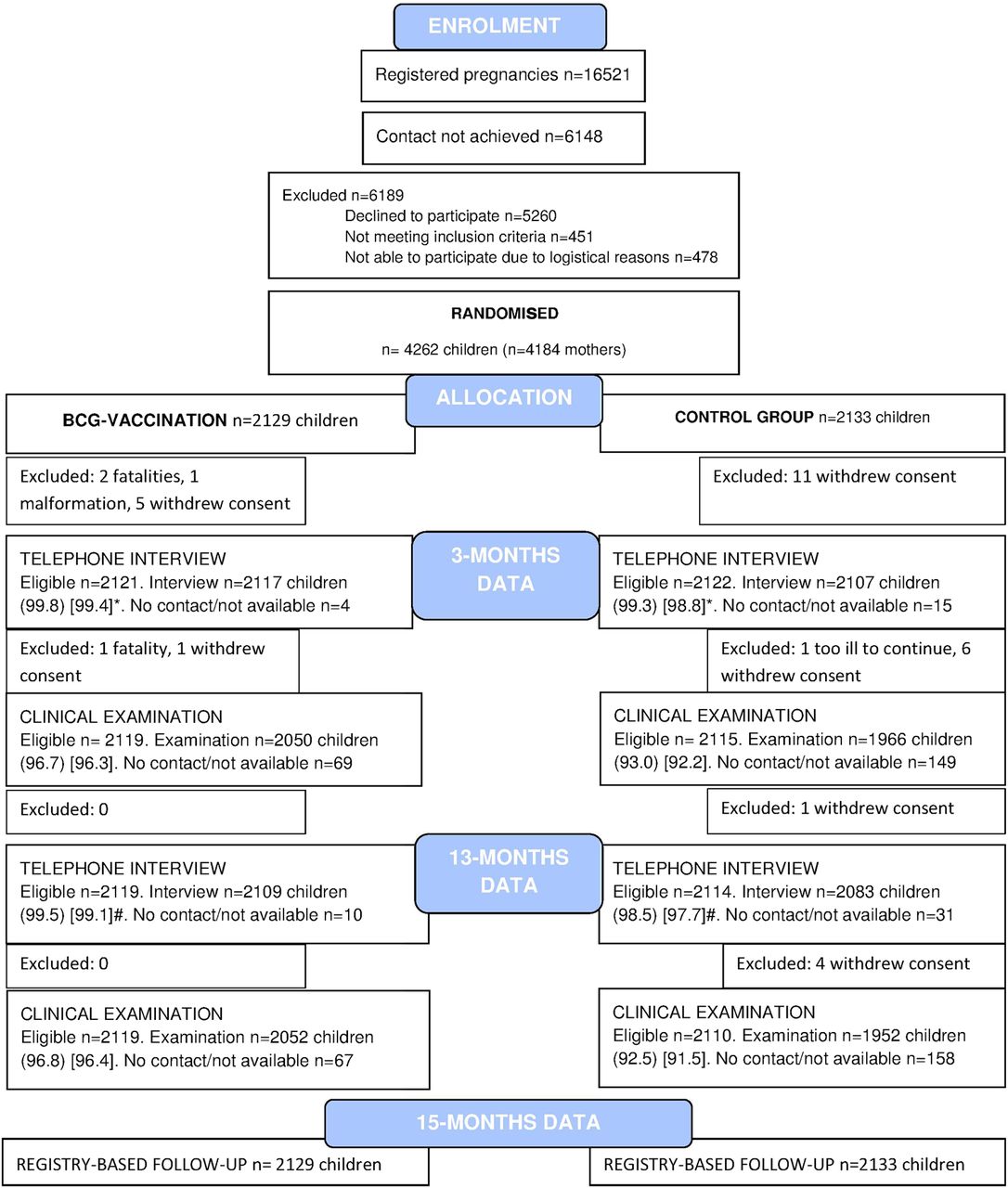
Flow chart. Data collection of The Danish Calmette Study, by telephone interviews, clinical examinations and health registers. Percentages in parentheses (): Percentage among the eligible children. Percentages in square brackets []: Percentage among all randomised children. *Interviews conducted between child age 2–4 months: BCG 98.1% (2089/2129), control 96.8% (2064/2133). #Interviews conducted between child age 10–14 months: BCG 97.9% (2084/2129), control 96.2% (2052/2133).
The study population was characterised by a large proportion of highly educated parents, with a high prevalence of atopic diseases.
Treatment assignments and crossovers
Two thousand one hundred and twenty-nine children were randomised to receive BCG and 2133 children to the control group. Eleven children randomised to the BCG group did not receive the BCG vaccine and 36 children randomised to the control group received the BCG vaccine on their own initiative leaving 2118 children allocated to BCG and BCG-vaccinated groups and 2097 children randomised to control and not vaccinated groups in the PP analysis.
Primary outcome: risk of all-cause hospitalisation
The rate of follow-up was 100% (figure 1). Until 15 months of age, the 2129 children randomised to BCG experienced a total of 1047 hospitalisations, the mean hospitalisation per child being 0.49; compared with 1003 hospitalisations among 2129 children randomised to control, the mean hospitalisation per control child being 0.47. Hence, there was no difference in number of hospitalisations from randomisation to 15 months of age in the ITT analysis (table 2 and figure 2).
Number of hospitalisations among 4262 Danish children by allocation to BCG vaccination at birth or control group (no intervention)

{kind=link}
{kind=link}
Estimated mean number of all-cause hospitalisations per child for children randomised to BCG or no BCG.
There was no effect modification by prematurity, sex or study site (table 2); however, the rate of hospitalisation was lower at the Kolding site where short acute admissions were classified as outpatient consultations. The results were essentially identical in the PP analysis (table 2). If the outcome was defined as time to first hospitalisation instead of recurrent hospitalisations, the HRs were 1.01 (0.91 to 1.13) (ITT) and 1.02 (0.92 to 1.14) (PP), respectively. The inclusion in the analysis of children from multiple births as clusters did not change the estimates (data not shown).
Secondary analyses
Adjustment for all baseline characteristics essentially did not change the estimates (see table 2 and 3), the HR of hospitalisation was 1.05 (0.93 to 1.20) for children randomised to BCG. For children randomised to BCG, the risk of hospitalisation was 0.98 (0.83 to 1.16) until 3 months and 1.09 (0.94 to 1.27) after 3 months of age. No statistically significant effect modification by caesarean section, administration of antibiotics to the mother during vaginal delivery, birth weight <2500 g, ≥1 sibling, atopic disposition, age at vaccination ≤2 days, maternal BCG vaccination and BCG vaccine batch was observed (table 3). However, a tendency towards protection against hospitalisation was observed among BCG-vaccinated children whose mother was also BCG vaccinated (table 3).
Secondary analysis
Discussion
We hypothesised that BCG vaccination at birth would have non-specific beneficial effects and reduce overall childhood hospitalisation for somatic acquired disease (injuries excluded) from birth to 15 months of age by 20% in the high-income setting of Denmark. We were not able to confirm this.
Strengths and weaknesses
The strengths of the present study lie in the randomised clinical multicentre trial design with adequate power. Data on the primary study outcome, all-cause hospitalisation, were collected independently of the study, decreasing the risk of bias. All participants could be followed up through the public registers.
The study may be limited by our choice of all-cause hospitalisation as primary outcome, which was chosen because of its potentially high impact on public health and because this outcome included both hospitalisation-requiring infections and severe manifestations of atopic disease. Given the high incidence of hospitalisations, this outcome, however, may not have been specific enough to detect a potential beneficial immune-training effect of BCG.
Comparison with other studies
In low-income settings, two randomised controlled trials among low birthweight children found BCG to reduce non-tuberculosis mortality until 6 months of age, in particular neonatal sepsis and respiratory infections.2 ,3 Recent immunological studies have provided a potential mechanism by showing that BCG induces trained innate immunity through epigenetic reprogramming of monocytes,13 ,14 which was still present 12 months after BCG.13 ,15 In Guinean babies, BCG was associated with increased responses to heterologous innate stimulation.16
There may be other explanations for the lack of effect of BCG on all-cause hospitalisation in Denmark.
First, in a system with free healthcare, hospitalisation for acquired somatic disease may not represent a sufficiently specific measure of disease. A high level of parental concern in combination with a low professional threshold for hospitalisation of young infants is likely to have inflated the hospitalisation rate. The rate of all-cause hospitalisation was 50% higher than expected.
Second, there are obvious differences in exposure to infection between Denmark and the low-income settings where the beneficial non-specific effects of BCG on mortality have been observed. The majority of children in the present study had no siblings, thus, presumably the exposure to infections was limited until they started day care around 1 year of age.
Third, we previously found that maternal immunity may also be of importance to the non-specific response to measles vaccination in the child;17 we therefore also asked whether the mothers in The Danish Calmette Study had been BCG vaccinated. In low-income settings the majority of mothers will have been BCG vaccinated, whereas in our study only 17% of the mothers had been BCG vaccinated, because BCG was discontinued in the early 1980s. That early exposure may be of importance to the child's response to BCG was also indicated by two studies comparing cytokine responses after BCG in UK and Malawi infants, and finding significant differences, which were ascribed to exposure very early, in utero, or within the first few months of life.18 ,19 Further, it has been shown that foetal T helper cells can be sensitised to mycobacterial purified protein derivative in utero.20 In agreement with this, in a preplanned secondary analysis of hospitalisations for infection within the present trial, a significant beneficial effect of BCG among children of BCG-vaccinated mothers was observed (personal communication, Stensballe LG, Greisen G, Jeppesen DL, et al. The effect of BCG vaccination at birth on risk of hospitalization for infection in Denmark. A randomized clinical multicenter trial. 2015. Unpublished work). If maternal exposure to BCG or mycobacteria is essential for the development of beneficial non-specific effects of BCG, this may explain the beneficial effect of BCG observed in low-income countries but not overall in the present study.
Fourth, genetics differ between the populations of West Africa and Denmark;21–23 however, the influence of this is not clear and it should be noted that others have found evidence of beneficial effects of BCG in Denmark.24
Conclusions
BCG vaccine at birth did not decrease the risk of hospitalisation for somatic acquired disease until 15 months of age in our high-income setting.
Acknowledgments
The authors thank the families and children for their participation, and The Danish Calmette Study staff for their commitment. The authors also thank the Data Safety Monitoring Board members Frank Shann, Professor of Paediatric Intensive Care Medicine, Melbourne, Per Kragh Andersen, Professor of Biostatistics, Copenhagen, and Jørn Olsen, Professor of Epidemiology, Aarhus (chair).
References
Footnotes
Contributors LGS conceived the idea and is the guarantor of the study. LGS, GG, DLJ, P-EK, OP supervised the collection of data by telephone interviews and clinical examinations and NMB, JK, TNN, GTP, LMT participated in this data collection. LGS, GG, P-EK, OP, CSB and PA constituted the Trial Steering Committee. LGS, HR and SS obtained the register-based data. HR, LGS and SS carried out data management. HR and LGS analysed the data. LGS drafted the manuscript. All authors read and approved the final manuscript.
Funding The study was funded by the three involved hospitals and by the Danish National Research Foundation (DNRF108).
Competing interests None declared.
Ethics approval The trial was approved by the Committees on Biomedical Research Ethics (J.no. H-3-2010-087), the Danish Data Protection Board (J.no. 2009-41-4141), and the Danish Medicines Agency (J.no. 2612-4356. EudraCT 2010-021979-85. Protocol 2009-323).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement A check of the validity of the data and analyses for this study can be arranged with the corresponding author. Request for access to a data copy should be directed to the Trial Steering Committee.