Article Text

Abstract
Objective The objective of this study was to develop a Hirschsprung’s disease (HD) core outcome set (COS).
Methods Candidate outcomes were identified from a systematic review and stakeholder nomination. A three-phase Delphi process and consensus meeting were used to prioritise candidate outcomes based on scores assigned by stakeholder participants using a nine-point scale. In phases two and three, participants were shown graphical representations of their panel’s scores and all panels’ scores respectively for each outcome from the previous phase. After the third phase, outcomes prioritised by two or three panels were taken forward to the consensus meeting. The COS was formed from the 10 highest scoring outcomes meeting the threshold for inclusion (≥70% 7–9 and <15% 1–3).
Results Eighty-nine stakeholders (82%) completed all three phases of the Delphi process. Seventy-four outcomes were assessed in phase one of the Delphi process, the following 10 of which met criteria for inclusion in the COS: (1) death with cause specified, (2) long-term faecal incontinence, (3) long-term voluntary bowel movements without need for enemas, or rectal or colonic irrigation, (4) long-term psychological stress for the individual with Hirschsprung’s disease, (5) long-term urinary incontinence, (6) objective score of quality of life, (7) objective score of bowel function, (8) unplanned reoperation, (9) >need for a permanent stoma, (10) enterocolitis.
Conclusions This HD COS is formed of 10 outcomes deemed important by key stakeholders. Use of this COS in research will reduce outcome reporting heterogeneity and increase our ability to identify gold standard treatments for HD.
- Hirschsprung’s Disease
- Core Outcome Set
- Paediatric Surgery
- Gastroenterology
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: http://creativecommons.org/licenses/by/4.0/
Statistics from Altmetric.com
What is known on this topic?
Outcome reporting heterogeneity in published research is preventing identification of gold standard treatments for infants with Hirschsprung’s disease.
Developing and using core outcome sets in research reduces outcome reporting heterogeneity.
What this study adds?
This study has identified 10 outcomes of importance to key stakeholders including people with Hirschsprung’s disease, parents of children with Hirschsprung’s disease and healthcare professionals managing children with Hirschsprung’s disease.
Use of this HD core outcome set will reduce outcome reporting heterogeneity, making it easier to identify gold standard treatments for children with Hirschsprung’s disease.
Background
Hirschsprung’s disease (HD) affects 1.8 in 10 000 live-born children in the UK and Ireland and is caused by failure of complete development of the nerves of the enteric nervous system. Definitive treatment requires excision of the affected colon, with anastomosis of the remaining normal colon to the anus or rectum. Globally, there are differences in management strategies.1 Operative strategies include open, laparoscopic and purely transanal approaches, and the Duhamel,2 Swenson3 and Soave4 anastomotic techniques. Each strategy has potential advantages and disadvantages and at present it is not possible, either with primary data or through conduct of systematic reviews, to identify a gold standard approach.5 6 The reasons for the lack of clarity are multifactorial. Specifically, most studies are small, single-centre, observational, of short duration and retrospective,7 with significant heterogeneity of outcome reporting.8
Outcome reporting heterogeneity makes the evidence base difficult to interpret in three ways. First, it creates a risk that studies fail to address outcomes of relevance to patients, clinicians and commissioners of healthcare. Second, it suggests and increased risk of reporting bias within the published literature, and finally, it limits the conduct of meta-analyses.
Core outcome sets (COS) are groups of standardised outcomes that have been identified by key stakeholders as being the most important in determining success of an intervention or treatment of a particular condition.9 Once a COS has been developed for a condition, the intention is that all future studies of that condition should report data for every outcome within the COS. Development and use of COS in this manner reduces outcome reporting heterogeneity,10 making it easier to identify gold standard treatments. Journal editors, the National Institute for Health Research Health Technology Assessment Programme and the IDEAL collaboration have endorsed this approach (http://www.comet-initiative.org/about/COMETendorsement). The objective of this work was therefore to develop a COS that could be used in studies comparing interventions for infants with HD.
Methods
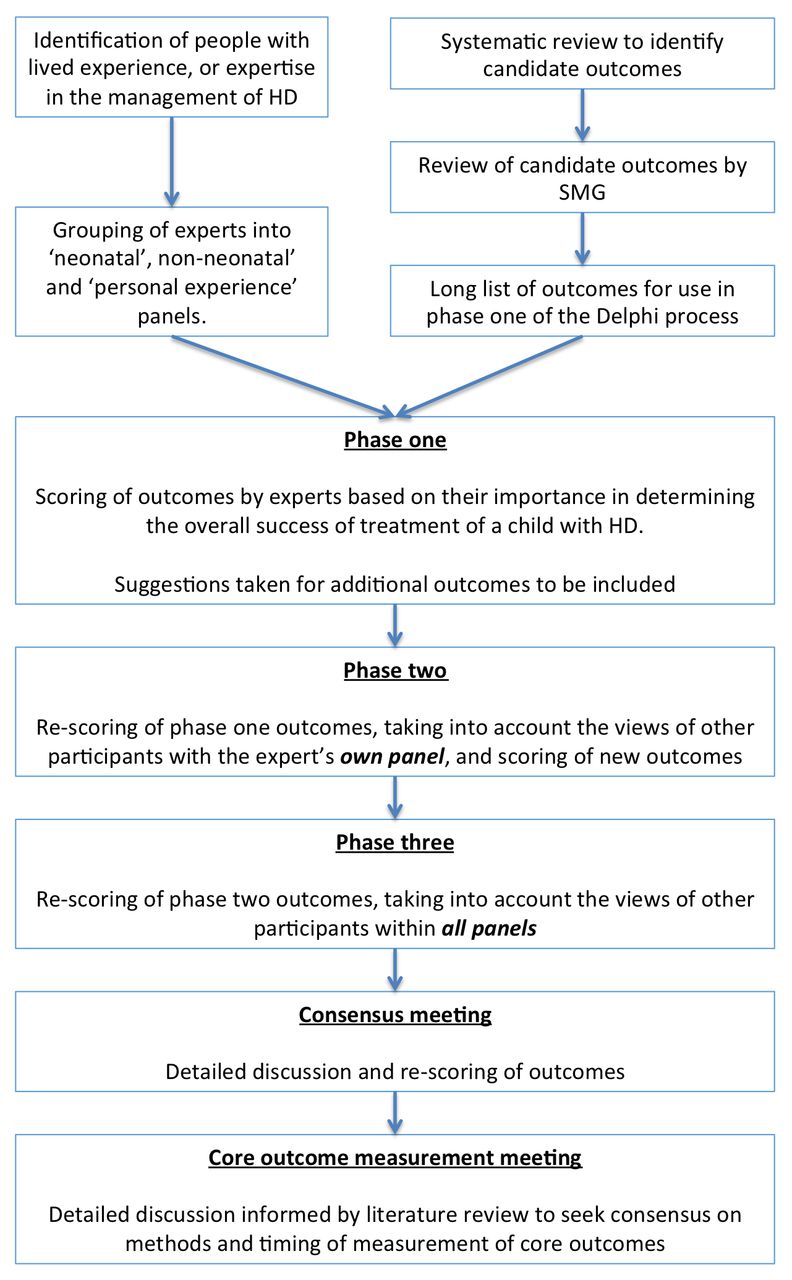
The COS was developed according to a prospectively registered protocol,11 using methodology recommended by the COMET initiative (figure 1).

Study overview. HD, Hirschsprung’s disease; SMG, study management group.
Scope
The aim was to develop a COS for use in studies comparing interventions for the treatment of infants with HD in high-income countries. It may need adaptation for low-income and middle-income countries.
Participants
Participants were recruited from key stakeholder groups with either expertise in the management of infants with HD or lived experience of HD (table 1). UK and international participants were recruited.
Recruitment targets for key stakeholder groups
An iterative process12 was used to recruit participants across stakeholder groups, including among others, paediatric surgeons, gastroenterologists, people with HD and parents of children with HD. Members of all stakeholder groups had an equal role in the prioritisation of outcomes, so as to ensure that the final COS represented as best as possible, the views of those with expertise in managing children with HD and those with lived experience of HD. Members of the study management group (SMG) identified experts known to them, and then nominated groups from which additional experts could be recruited (table 1). Electronic media for each of the appropriate organisations were used to distribute adverts to their membership. Experts registering to participate in the study were asked to provide information relating to their experiences of HD and to nominate other potential participants. Registration details for all experts were reviewed by the SMG to ensure they had sufficient expertise to participate. Target recruitment was a minimum of 50 experts with two or more from each stakeholder group.
Participants were deemed to have withdrawn from the development process if they did not complete a phase of the Delphi process prior to the prespecified deadline, and were thus ineligible for participation in later phases or the consensus meeting. A representative sample of participants completing the Delphi process were invited to the subsequent consensus meeting and measurement meeting.
Information sources
Candidate outcomes were identified from a systematic review of surgical interventions for the primary, definitive treatment of infants with HD.8 Additional outcomes of importance identified by the SMG but not identified in the systematic review were added to this list. At the end of phase one of the Delphi process, participants could suggest additional outcomes that were of importance to them, and if within the scope of the COS, these were added to phase two. Lay equivalent language for each outcome was developed in conjunction with parents without a medical or scientific background. Each outcome was assigned by the SMG to a core area of the OMERACT 2.0 filter (death, life impact, pathophysiological manifestation or resource use/economical impact) and identified as an adverse event if appropriate, using the guidelines described by Boers et al.13
Consensus process
A three-phase online Delphi process was conducted in parallel for the three panels and was followed by a face-to-face consensus meeting.
In phase one, participants were asked to score candidate outcomes based on their importance in deciding whether the overall treatment of a child’s HD had worked well. Participants were provided with written instructions to score from 1 to 9 where 1, 2 and 3 were ‘not that important’, 4, 5 and 6 were ‘important’ and 7, 8 and 9 were ‘really important’. In phase two, participants were shown graphical and numerical representations of their panel’s median score and distribution of scores for each outcome from phase one and asked whether they would like to change their scores based on this information. In phase three, participants were shown graphical and numerical representations of all panels’ median scores and distribution of scores for each outcome, and again asked if they would like to change their scores based on this information.
Outcome dropping and modification
Following phase two, outcomes where ≥50% of participants in any panel had scored them 1–3 and <50% of participants in all panels had scored them 7–9 were dropped. Following phase three, outcomes were deemed to meet the threshold for automatic discussion and rescoring at the consensus meeting if two or more panels deemed them to meet consensus for inclusion in the COS. Consensus for inclusion was defined as scores of ≥70% 7–9, and <15% 1–3. Other outcomes were only discussed and rescored if there was unanimous agreement among consensus meeting attendees that they warranted further review.
Consensus definition
Outcomes with scores of ≥70% 7–9 and <15% 1–3 following discussion at the consensus meeting were eligible for inclusion in the COS. However, to ensure practicality of use, it was prespecified that 10 or fewer outcomes would be included in the COS. If more than 10 outcomes were eligible for inclusion, then only the following 10 would be included:
the highest scoring outcome meeting consensus for inclusion in each of the four OMERACT 2.0 filter core areas
the highest scoring adverse event outcome meeting consensus for inclusion in the COS (if not already included as the highest scoring outcome in one of the four core areas)
the next five highest scoring outcomes meeting consensus for inclusion in the COS, regardless of OMERACT 2.0 filter core area.
As the highest scoring adverse event outcome meeting consensus for inclusion in the COS was already included as one of the highest scoring outcomes from the core areas of the OMERACT 2.0 filter; the sixth highest scoring outcome (not already included) meeting consensus for inclusion in the COS was also included.
Highest scoring was defined as greatest percentage of participants allocating scores of 7–9. Where outcomes were tied based on this score, then the highest scoring outcome was the one with the greatest percentage of participants allocating a score of 9, then 8, then 7, continued through to 1 if necessary.
Outcome definition and measurement
A literature review was conducted to identify existing definitions and methods of measuring the outcomes included in the COS following the consensus meeting. This review informed discussion at a meeting attended by a representative sample of study participants, where outcome definition and measurement were identified by group consensus.
Results
Changes from protocol
The following changes to protocol were made after registration but prior to data analysis.
No dropping of outcomes between phases of the Delphi process or between the Delphi process and the consensus meeting was originally planned. However, it was decided that outcomes should be dropped as described to allow participants to focus on discriminating between those outcomes most likely to form the COS.
No limit on the number of outcomes to be included in the COS was originally planned. However, in order to ensure practicality of use, it was determined that the COS would be limited to 10 outcomes.
Participants
One hundred and forty-five experts registered to participate in the study, 108 (74%) of whom completed phase one of the Delphi process. Ninety-six eligible participants (89%) completed phase two, and 89 eligible participants (93%) completed phase three. Seventeen participants were selected to attend the consensus meeting, and 14 attended the measurement definition meeting (tables 2 and 3).
Summary of participants
Characteristics of participants who completed the Delphi process and those who dropped out of the study
Outcomes: initial phase one list
Seventy-four outcomes were identified by the systematic review, nine were added by the SMG, and nine were excluded as outside of the scope of the COS (online supplementary material 1).
Outcomes: addition, dropping and formation of the COS
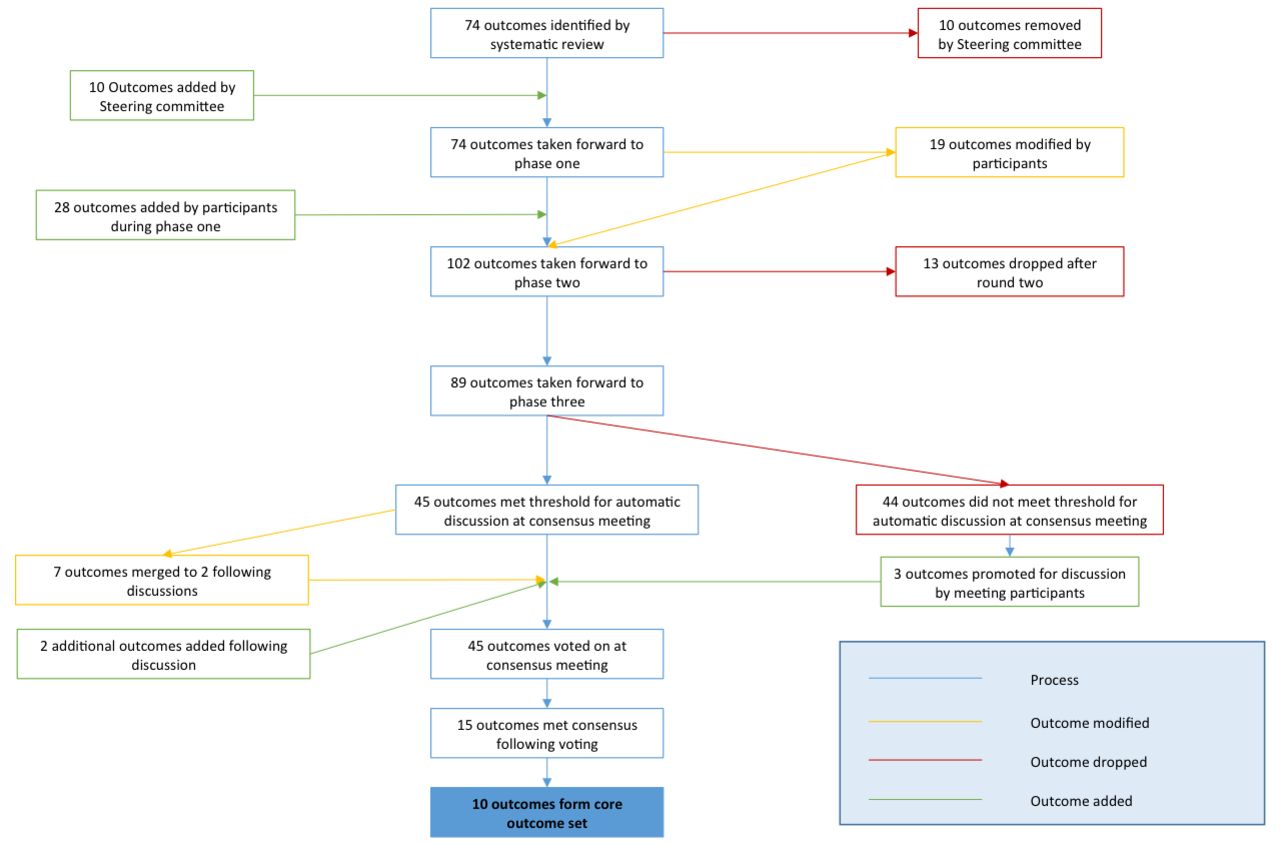
Overall 140 individual comments were made by participants during phase one, 62 of which (44%) were made by 15 members (44%) of the neonatal panel, 73 (52%) by 35 members (57%) of the personal experience panel and 5 (4%) by 2 members (15%) of the non-neonatal panel. Based on these comments, the SMG clarified 19 outcomes (26%) and added 28 new outcomes for assessment in phase two. Six of these outcomes (21%) were proposed by the personal experience panel, 6 (21%) by other panels, and the remaining 16 (57%) by multiple panels. Overall, 102 outcomes were taken forward to phase two. Following completion of phase two, 13 outcomes (13%) were dropped, and following phase three, 44 outcomes (49%) did not meet criteria for automatic progression to the consensus meeting. Forty-five outcomes were taken to the consensus meeting, following which 15 outcomes met the criteria for inclusion in the COS, and 10 were retained (figure 2, tables 4 and 5 and online supplementary material S1). These 10 core outcomes are described in table 5.
{kind=link}
{kind=link}
Outcome flow.
Outcomes scored at the consensus meeting
The Hirschsprung’s disease core outcome set
Proposed timing and measurement of outcomes
Consensus from meeting attendees was that outcomes should be measured at standard surgical and paediatric time-points determined by study design. For studies where infants entered at the point of surgical intervention, these were defined as 30 days, 90 days, 1 year, 5 years, 10 years and every subsequent 10 years postintervention. For studies where infants entered at a set age, outcome measurement points were defined as 28 days of age, 1 year of age, 5 years of age, 10 years of age and every subsequent 10 years. It was agreed that six outcomes (table 5) should not be reported prior to 5 years of age, as early data on these outcomes are likely to be misleading.
Discussion
This development process identified a COS consisting of 10 items for use in studies comparing interventions for the treatment of infants with HD. These outcomes represent factors important to stakeholders and span the breadth of the OMERACT filter 2.0. When used in appropriate studies, they will provide a rounded assessment of different interventions for HD. All studies comparing interventions for the treatment of children with HD should report data at the specified time-points for the outcomes within the COS.
We believe this to be the first paediatric general surgical COS. However, paediatric COS have previously been developed, including for asthma and otitis media in children with cleft palate.14 15 Some common themes emerge from all three, including the prevalence of factors relating to quality of life, which are likely to be common to many paediatric COS, but which are currently infrequently investigated.8 The COIN study (http://www.comet-initiative.org/studies/details/842?result=true) will develop a COS for neonatology, and the NETS1G study16 is developing a COS for gastroschisis. Following completion of these, it will be important to compare and contrast the outcomes of importance in each so as to identify areas of overlap from which a unified neonatal surgical COS could potentially be developed.
This HD COS has been developed using robust methodology in accordance with recommendations from the COMET initiative. Participation rates were significantly above our target recruitment of 50 experts, with a good spread across stakeholder groups and good retention throughout the process. We therefore believe the COS to be representative of the views of the HD community as a whole. Increasingly however, there is a move towards undertaking qualitative work with key stakeholders in addition to a systematic review to inform the long-list of outcomes assessed during the Delphi process. This methodology is being promoted as there is a suspicion that outcomes identified through systematic reviews may be biased in favour of clinicians and researchers.17
Instead of using qualitative methods to inform the Delphi process, we opted to conduct the Delphi in an adaptive manner. All participants were asked to recommend additional outcomes of importance to them at the end of phase one and could suggest modifications to outcomes at all stages of the consensus process. The low number of additional outcomes proposed by the personal experience panel suggests that either they felt the initial list covered the majority of outcomes of importance to them or that they felt unable to propose additional outcomes. As over 50% of comments made in phase one were from members of the personal experience panel, and nearly 60% of the personal experience panel made at least one comment during phase one, we believe the former theory to be more likely. It is also reassuring that there was similarity in the number of outcomes suggested by each panel and that there was overlap in the domains from which additional outcomes were suggested by each panel.
There are three areas that may affect the representativeness of the COS. First, from the personal experience panel, there was a larger proportion of women taking part than men, meaning that the views of fathers, and men with HD, are potentially under-represented. Second, there was a slightly greater proportion of participants with long-segment and ultra-short segment HD within the study population than would be expected within the general population. This may skew the priorities of the personal experience panel more towards the extremes of the disease population. Third, the non-neonatal panel consisted of fewer participants than either the neonatal or personal experience panels. By giving equal weight to each panel as opposed to each individual participant throughout the Delphi process, individual participants within the non-neonatal panel will have had a proportionately greater influence on the scoring of outcomes throughout the Delphi process than participants in other panels. At the consensus meeting however, the meeting attendees were treated as one group, not individual panels. Within this setting, therefore, where there were less experts from the non-neonatal panel than from other panels, there is potential for the views of members of the non-neonatal panel to have been under-represented in the final COS.
This study has incorporated the views of key stakeholders to develop a COS for use in studies conducted in high-income countries comparing interventions for the treatment of infants with HD. It is important to promote the use of this COS in future large-scale observational and interventional studies but also in smaller, retrospective studies that still comprise the vast majority of paediatric surgical research.7 Doing so will ensure studies are relevant to patients and their family, reduce the risk of reporting bias and, importantly, make meta-analysis possible. In the long run, this will improve the evidence base used to support clinical management of infants born with HD and should eventually allow translation through into improvements in patient care. It is now incumbent on funding bodies, journal editors and key decision makers in the field of paediatric surgical research to ensure that the COS is widely implemented and the benefits of its use realised.
Acknowledgments
The Next stage in Evidence-based paediatric surgery Treatment Strategies (NETS) programme of work is designed to develop and implement the use of COS in paediatric surgery. As part of this programme of work, the NETS1HD collaboration was formed to develop an HD core outcome set.
Footnotes
GW and MK contributed equally.
Contributors BSRA was responsible for design of the study, day-to-day management of the study, analysis of data and drafting of the manuscript. TB, SK, GW, JJK and MK were responsible for design of the study, management of the study and contributed to critical revisions of the manuscript. Members of NETS1HD contributed critically to the academic content of the study and have reviewed and critically revised the manuscript.
Funding MK is funded by a National Institute for Health Research (NIHR) Professorship. BSRA is funded by an NIHR Doctoral Research Fellowship.
Disclaimer The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health. The NIHR had no role in design and conduct of the study; collection, management, analysis and interpretation of the data; and preparation, review or approval of the manuscript; and decision to submit the manuscript for publication.
Provenance and peer review Not commissioned; externally peer reviewed.
Collaborators The members involved in NETS1HD Collaboration who went through completion of all three phases of the Delphi process contributed significantly to the development of this HD core outcome set: Martin Ward Platt, Sridhar Ramaiah, Nim Subhedar, Anna-May Long, Mike Stanton, David Burge, Kokila Lakhoo, Stefano Giuliani, Paul Johnson, Silke Wagener, Graham Lamont, Nigel Hall, Isaac Philip, Richard Lindley, Catherine Bradshaw, Ian Sugarman, Simon Clarke, Claire Clark, Clare Rees, Ivo de Blaauw, Bala Eradi, Janne Suominen, Mark Tighe, Andrew Barclay, Diana Flynn, Sara Jones, Keith Hipkin, Kelly Arnold, Clare Lambert, Tracey Fuller, Stella Taylor, Patricia Umney, Lacey Edwards, Poly The, Michelle Luckett, Claire Ryder, Jennie Kennerley, Elizabeth Faulkner, Claire Radtke, Holly Stowell, Lucy Somers, Rachel Tabone, Toni Colgan, Helen Sanderson, Lorina Woodward, Raeley Grant, Helen Fowler, Cynthia Rauscher, Marianne Woller, Katrina Randon, Katherine Brandist, Vanessa Riordan, Vicky Taylor, Nicola Purdy, Lorraine Pearce, Kylee Murray, Lisa Coleman, Lucy Nall, Lisa McIntosh, Nicola Krijger, Macaley Smith, Sharon Magalona, Carolyn Walker, Alison Broadbent, Stephen Caldwell, Christeen Smith, Ali Wright, Claire Bohr, David Pambakian, Geoffrey Piper, Neil Woller, Katherine Woller, Osvaldo Borrelli and Marion Lambourne. Based on their attendance at the consensus meeting, the following people form the NETS1HD collaboration: Sarah Almond, Rebecca Craven, Karen Dick, Richard England, Alan Fenton, Susan Grieve, Jonathan Hind, Vicky Hogg, Gemma Jordan, Victoria Lane, Marc Levitt, Gerry McGregor, Alison Sharrard, Jonathan Sutcliffe and Katie Yearsley.